
INITIAL PRESENTATION
Chief complaint: Firework injury left eye
History of Present Illness
A 48-year-old male presented to the University of Iowa Emergency Treatment Center on July 4th due to a firework injury to his left eye. The injury occurred when the patient leaned over a repeater firework after it had malfunctioned. The firework launched and directly contacted the left orbit. The patient experienced severe eye pain and had immediate loss of vision in the left eye (OS). He denied loss of consciousness or right eye involvement.
Past Ocular History: None
Past Medical History: None
Past Surgical History: None
Medications: None
Allergies: No known drug allergies
Social History: The patient denied smoking or illicit drug use
OCULAR EXAMINATION
Visual Acuity (without correction):
Pupils:
Ocular Motility:
Confrontation Visual Fields:
External Exam: (Figures 1a and 1b)
 |
 |
| Figure 1a: External photograph of the left eye demonstrating brow lacerations, full-thickness left upper lid laceration, periorbital ecchymosis, and inferior orbital rim step-off | Figure 1b: External photograph of the left eye demonstrating chemosis, scleral laceration, and a 100% hyphema. There was no view of the posterior pole. |
Slit Lamp Exam:
Dilated Fundus Exam:
Imaging
A maxillofacial and head CT showed an irregularly shaped left globe, a left orbital floor blowout fracture and a lamina papyracea fracture on the left.
DIAGNOSIS: Open globe OS, multiple left orbital fractures, and left eyelid and brow lacerations
CLINICAL COURSE
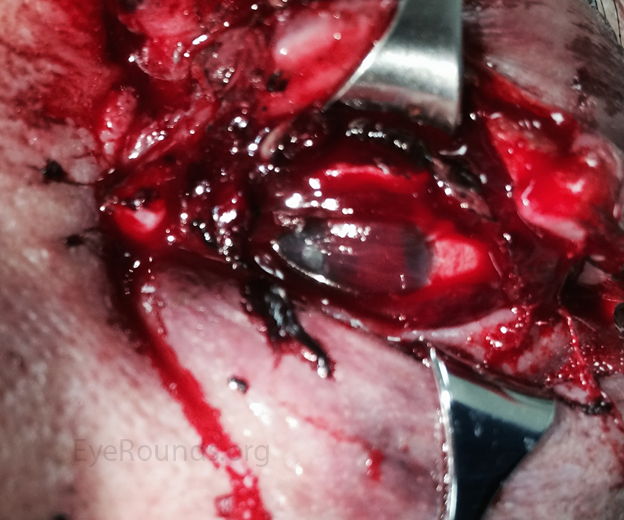
The patient was taken to the operating room for a primary globe repair by the ophthalmology on-call team. Intra-operative findings included a scleral laceration from 9:00 at the nasal limbus extending superiorly to 3:00 temporally behind the lateral rectus and then extending 20 mm posterior from the limbus with uveal contents prolapsing through the scleral laceration. The eyelid and brow lacerations were repaired by the oculoplastics service while in the operating room. The surgery lasted approximately 8 hours in total. On post-operative day 1, the patient's left eye remained blind and painful. A discussion was held introducing the possibility of an enucleation. The patient was discharged from the hospital, and returned to the ophthalmology clinic as an outpatient on post-operative day 2, where a B-scan ultrasound showed disorganized intraocular contents. Further discussion was held regarding enucleation. The patient agreed to proceed with enucleation, which was performed without complication on post-operative day 4. Over the following few months, the patient was fitted for a prosthesis (Figure 2), and resumed his previous activities of daily living with monocular precautions.

Figure 2: External photograph six months after the injury with a prosthesis in place.
Of the nearly 9,000 firework injuries that occur in the United States each year, approximately 45% are sustained by children age 15 and under.
- American Academy of Ophthalmology (2)
This patient provides an unfortunate case of a severe firework-related ocular injury. Each year, many injuries occur as a result of firework displays. According to data from the U.S. Consumer Product Safety Commission (CPSC) on non-occupational fireworks-related deaths and injuries, there were 600 firework-related ocular injuries in the United States that occurred in the calendar month of June 22 - July 22, 2012 alone and on average 230 people per day go to the emergency room in the month around July 4th(1). Of the nearly 9,000 firework injuries that occur in the United States each year, approximately 45% are sustained by children age 15 and under (2) and about 20% affect the eyes (1). Around 75% of firework-related ocular injuries occur in small family-type firework displays, and a majority of the injuries are due to mishandling of explosive pyrotechnic devices (3). Fortunately, most firework injuries do not cause severe vision loss and the enucleation rate remains low at 3.9% (4). In a study of 46 consecutive firework-related ocular injuries in the Zhongshan Ophthalmic Center in Southern China, the average age was 14.3 +/- 8.5 years, and the best corrected visual acuity after treatment was 20/100 or less in 76% of eyes (5).
Unfortunately, our patient experienced a severe injury that ultimately led to an enucleation after a primary globe repair. An alternative treatment option was a primary enucleation, though our ophthalmology department strongly leans towards attempting primary globe repair before consideration of enucleation. This offers several benefits including:
Although a primary enucleation may significantly decrease the likelihood of a second surgery, a primary globe repair is felt to be the preferred approach in the vast majority of cases in our department. There may be times when primary enucleation is appropriate, such as if the eye already had poor visual potential prior to the trauma or if there is no eye to be found after the trauma, however, these instances are rare.
Nearly half of all firework injuries (47%) occur to those who are bystanders or observers of firework shows (4).
 State regulations range from restricting purchases only to sparklers all the way to a complete ban on all consumer fireworks (6). The Consumer Product Safety Commission (CPSC) is responsible for enforcing firework regulations and places great emphasis on working toward a reduction in fireworks-related deaths and injuries. The CPSC has developed a list of safety tips to encourage responsible use of fireworks (1). The commission warns that though there are legal consumer fireworks that adhere to regulations and are comparatively safe, "all fireworks, by their nature, are hazardous and can cause injuries" (6).
State regulations range from restricting purchases only to sparklers all the way to a complete ban on all consumer fireworks (6). The Consumer Product Safety Commission (CPSC) is responsible for enforcing firework regulations and places great emphasis on working toward a reduction in fireworks-related deaths and injuries. The CPSC has developed a list of safety tips to encourage responsible use of fireworks (1). The commission warns that though there are legal consumer fireworks that adhere to regulations and are comparatively safe, "all fireworks, by their nature, are hazardous and can cause injuries" (6).
Research has demonstrated that legislation affects the incidence of firework-related injuries (3). An 87% reduction in the rate of trauma incidence was observed in areas with restrictive firework legislation based on a meta-analysis of 7,742 firework-related ocular injuries (4). While firework displays are traditional in the celebration of major holidays in the United States and around the world, it is important to recognize the danger imposed by explosive devices. Laws restricting consumer firework use may be indicated to promote public safety. Most notably, nearly half of all firework injuries (47%) occur to those who are bystanders or observers of firework shows, further emphasizing the public significance of this issue (4).
The Consumer Product Safety Commission's tips for responsible fireworks use (1):
Niles PI, Cohen A, Sacher B, Kitzmann A, Shriver EM, Allen RC. Firework-Related Ocular Injuries. Jan 29, 2015; Availble from https://eyerounds.org/cases/202-fireworks.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
