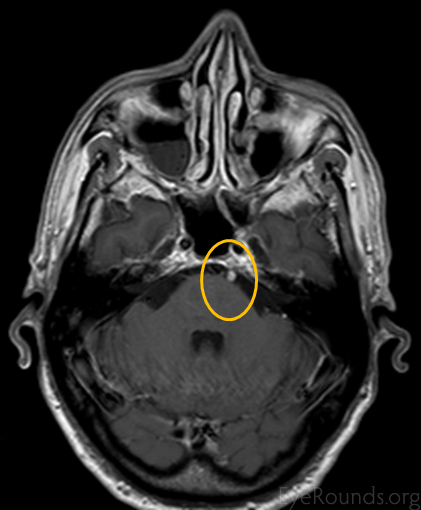
This patient presented with slowly progressive, painless, horizontal, binocular diplopia that worsened with left gaze and resolved in right gaze. She has adopted a mild left face turn and has an esotropia in primary gaze. The esotropia worsens in left gaze and there is an abduction deficit of the left eye. Her findings are consistent with a cranial nerve VI palsy on the left. MRI showed nodular enhancement near the pons along the tract of the sixth nerve on the left that is consistent with a schwannoma of cranial nerve VI.
Cranial nerve VI (CNVI or abducens nerve) innervates the lateral rectus muscle that is responsible for abduction of the eye. Weakness of the lateral rectus will result in binocular, horizontal diplopia that worsens in gaze to the affected side. Patients will have an abduction deficit with an incomitant esotropia that is worse on attempted gaze to the affected side.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links