73-year-old male, with no prior past ocular history, presented at the referral of an optometrist for the possibility of retinoschisis in both eyes. He was asymptomatic without any flashes, floaters, or peripheral vision loss. He had no family history of any retinal problems.
BCVA: OD 20/20, OS 20/30 with correction
SLE: 3+ NS OU; no PVD OU
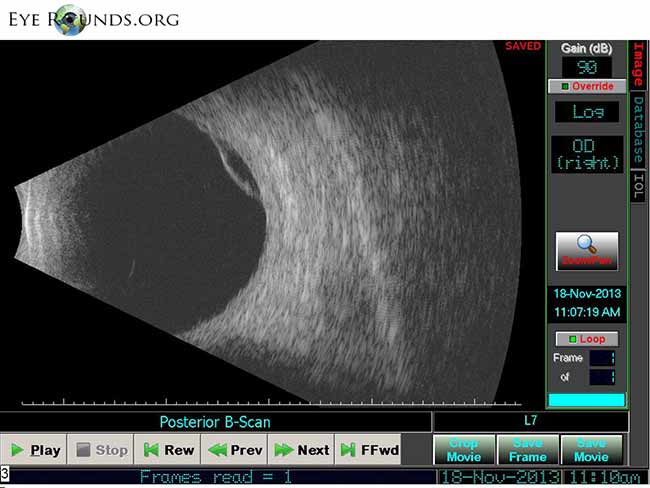
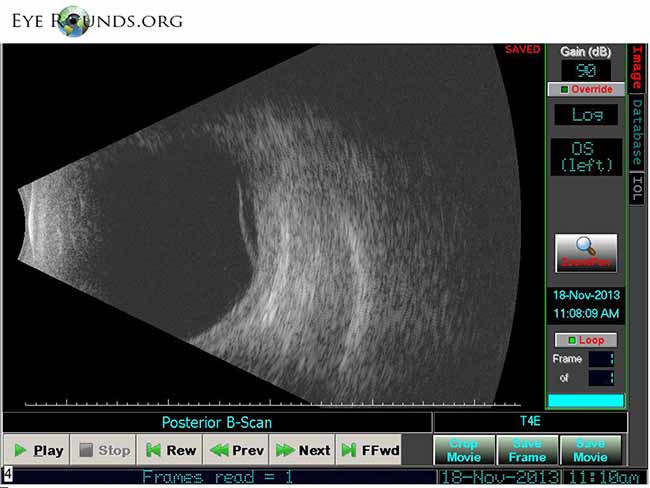
DFE: normal without any peripheral retinal tears, holes, or detachments; inferotemporally there was a dome-shaped 'boggy-area' of elevated retina near the retina in both eyes.
B-scan OU: mild vitreous opacities, dome-shaped retinal elevation inferotemporally consistent with retinoschisis.
"Retinoschisis" is splitting of the neurosensory retina. It can resemble the appearance of a retinal detachment. The most common form of retinoschisis is "acquired retinoschisis", where the split is in the outer plexiform layer. The inferotemporal quadrant is most commonly involved.
Most acquired retinoschisis remains stationary over many years, but some eyes do progress to rhegmatogenous retinal detachment.
B-scan ultrasound is a useful adjunct to confirm splitting of the retinal layers in the periphery. Bilateral symmetry and an inferotemporal location are highly suggestive of retinoschisis. Also, A-scan measurements showing splitting of the retinal layers are helpful.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.


Address
University of IowaLegal
Related Links