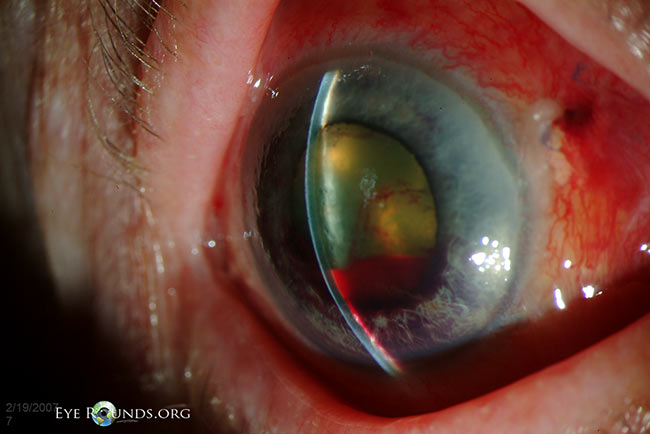
This 73-year-old woman presented with eye pain and nasuea/vomiting one day after pars plana vitrectomy for a macula-off rhegmatogenous retinal detachment that included gas-fluid exchange with 10% C3F8. Her intraocular pressure was 50 mm Hg. As evidenced in this photograph, she had 360 degrees of iridocorneal touch. The anterior chamber was extremely shallow and only present directly over the lens. There was a small hyphema. The view to the posterior chamber was poor, but it appeared there was a 100% gas bubble. It was felt her angle closure was secondary to posterior pressure from over-expansion of intraocular gas. A component of aqueous misdirection was also considered a possibility, though the patient already had undergone a vitrectomy. Pupillary block was also on the differential, but typically the central anterior chamber is not this flat in pupillary block. Multiple vitreous taps were performed, but these were not adequate to maintain a normal pressure. Eventually, an air-fluid exchange was performed and the size of the gas bubble was decreased to 25%. The anterior chamber was also reformed with balanced salt solution. Her pressure normalized and she eventually did well.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.


Address
University of IowaLegal
Related Links