Chief Complaint: 31-year-old male with "floaters and blurry vision" in the right eye (OD).
History of Present Illness: In August 2007, a healthy 31-year-old truck driver from Nebraska started noticing floaters in his right eye. The floaters gradually worsened and clouded his central vision. His family doctor tried changing his blood pressure medications, but this did not help. He later saw an ophthalmologist in his home state who told him there was a "mass" in his right eye. He was referred to the University of Iowa Department of Ophthalmology and Visual Sciences.
Past Ocular History: The patient has had no prior eye surgery or trauma.
Medical History: The patient reports prior excision of a benign skin nevus. He also has hypertension.
Medications: Metoprolol and triamterene/hydrochlorothiazide
Family History: The patient's mother has a history of neurofibromatosis. His father had an enucleation for an "eye cancer" and subsequently died due to metastatic spread of the cancer. His grandmother had skin melanoma.
Social History: The patient lives in Nebraska with his wife and child. He has never smoked and only drinks on "special occasions".
Review of Systems: Negative, except as noted above.
Ocular Examination:
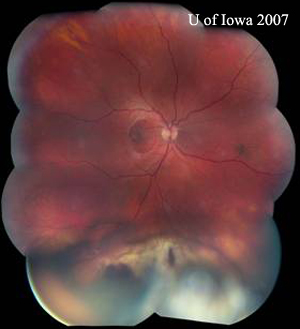
Figure 1A: Slit lamp examination shows cystic and solid components to the lesion. |
Figure 1B: Retroillumination further delineates the cystic portion of the lesion. |
|
|
|
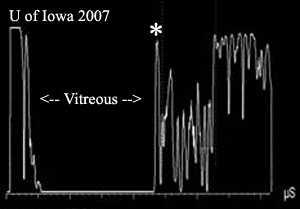
Standardized echography: Echography revealed a dome-shaped lesion at 5:30 measuring 6.2mm in height. There was a spherical-shaped extension over this lesion, consistent with the above-noted pigmented mass. The lesion was irregular with low reflectivity and 2+ vascularity. There was no evidence of extraocular extension. There was a long, low reflective tail extending posteriorly into the choroid from 5:30 o'clock.
| Figure 3A: Standardized B-scan echography of the lesion, OD. | Figure 3B: A-scan reveals low and medium reflectivity of throughout the lesion (posterior to the highly-reflective retinal surface spike indicated by the asterisk *). Low internal reflectivity is defined as a signal that is 40% or less than the height of the retinal spike. |
|
|
Course: In summary, the patient's findings included an amelanotic, low reflective, ciliochoroidal mass with associated retinal hemorrhages in his right eye. There was mild vitreous cell and an epiretinal membrane. The lesion also had a pigmented, partially cystic component extending into the ciliary body and a sentinel vessel anteriorly on the ocular surface. The ocular findings were discussed extensively with the patient and his family; they were told that the mass might represent a primary uveal melanoma. Other possible explanations included metastatic disease to the eye or an atypical inflammatory lesion.
A metastatic evaluation was performed on the same day of presentation. Physical exam, laboratory evaluation, PET scan and CT scan were negative for metastatic disease. When the metastatic workup failed to reveal a primary tumor, a primary uveal melanoma seemed much more likely. At that point, we determined with the patient to definitively rule out an inflammatory lesion. After 10 days of oral prednisone, the lesion remained unchanged, which suggested primary melanoma as the diagnosis. At this point, a biopsy was recommended. The patient refused biopsy because he did not like the possibility of having two procedures. The patient was given the options of radiation, observation or enucleation. Radioactive plaque implantation (brachytherapy) was explained to the patient as an option for saving the eye, although he was told that he would likely lose most or all his vision over the ensuing few years and that he would need to return at least twice a year for follow-up. After a lengthy discussion, the patient preferred to have a single procedure and be "finished with the issue" rather than have to make further trips from Nebraska to Iowa for follow-up.
In November 2007, the patient returned to Iowa for enucleation of his right eye. He tolerated the procedure well and the globe was assessed by the F.C. Blodi Ocular Pathology Laboratory.
|
|
|
|
|
|
|
|
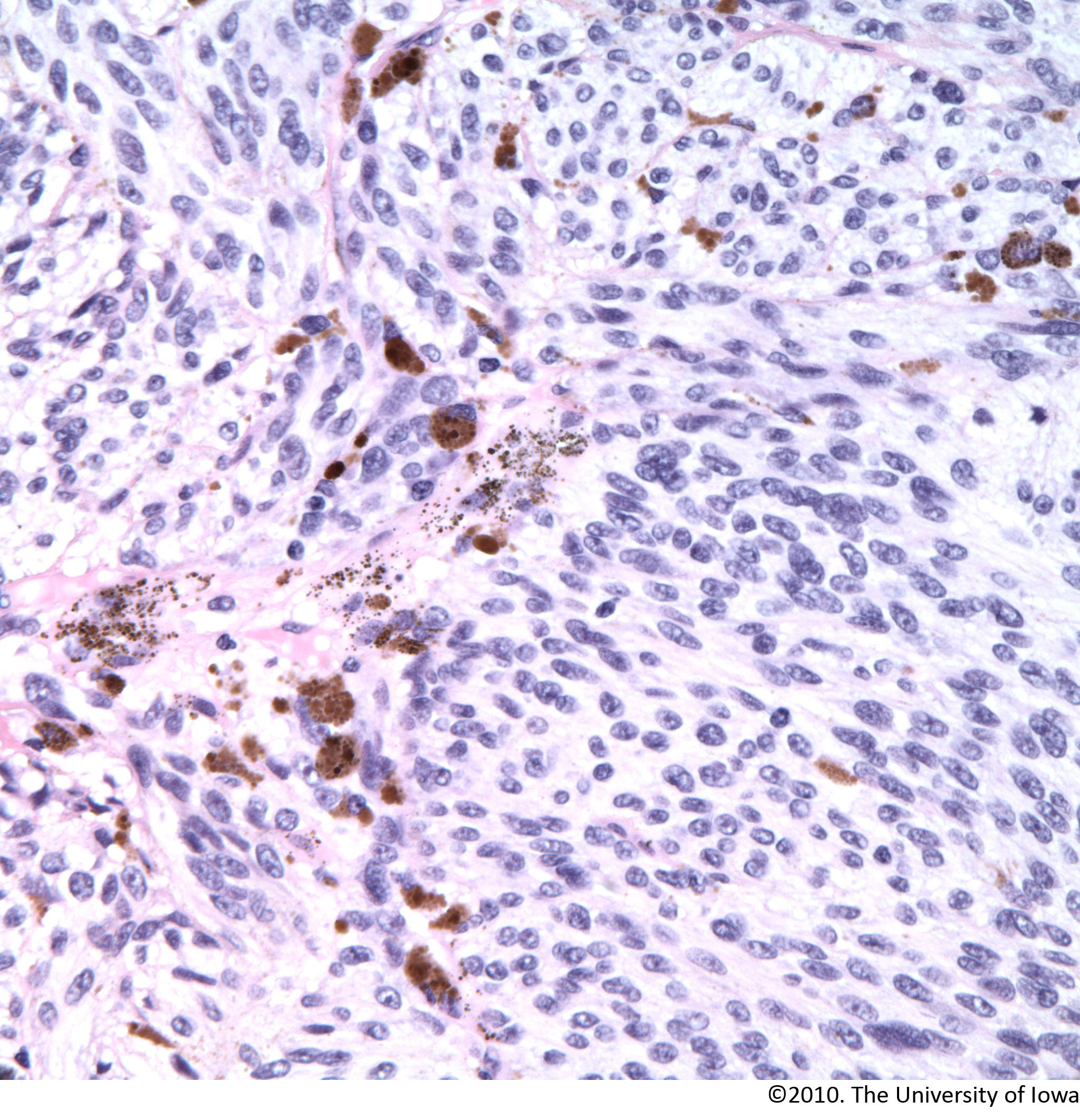
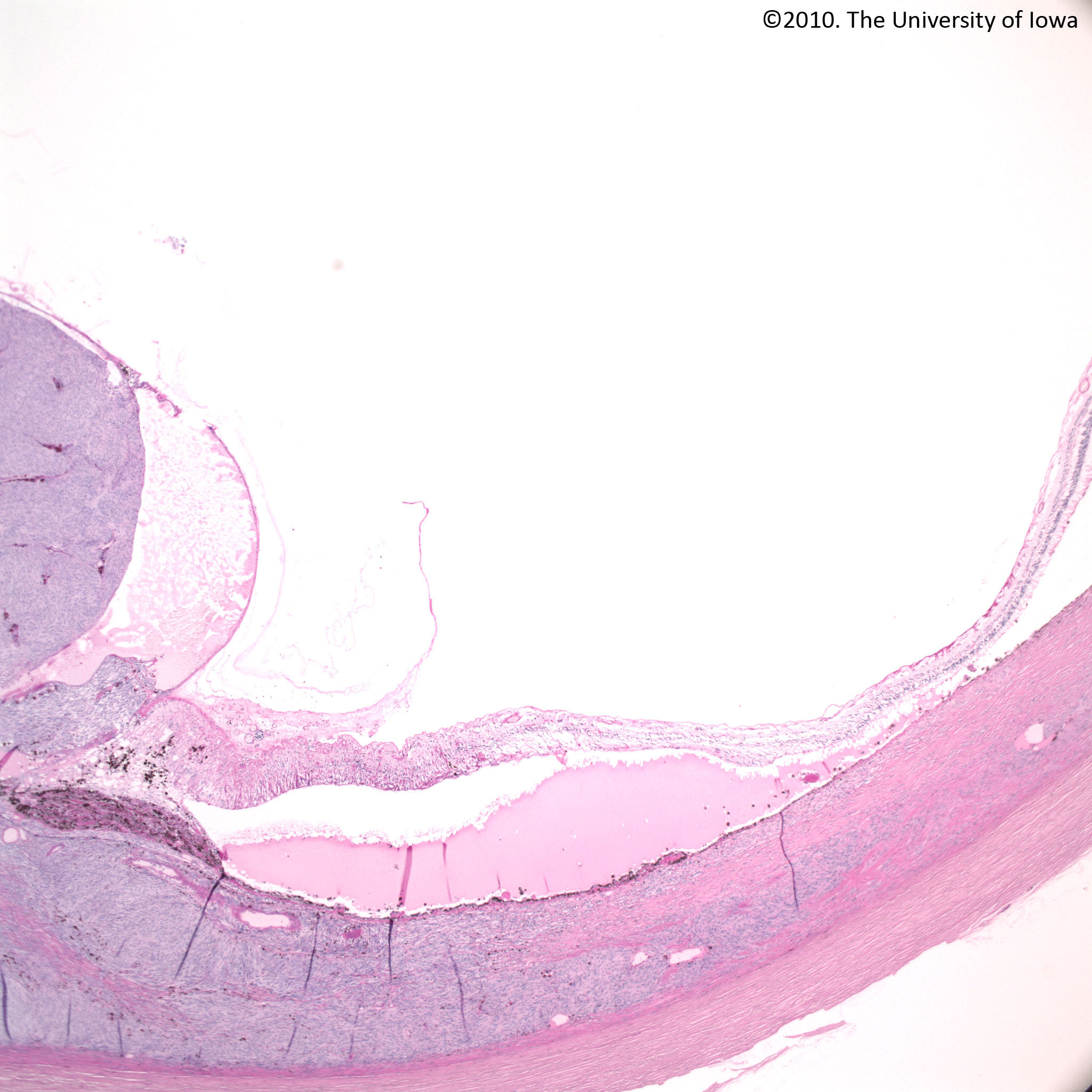
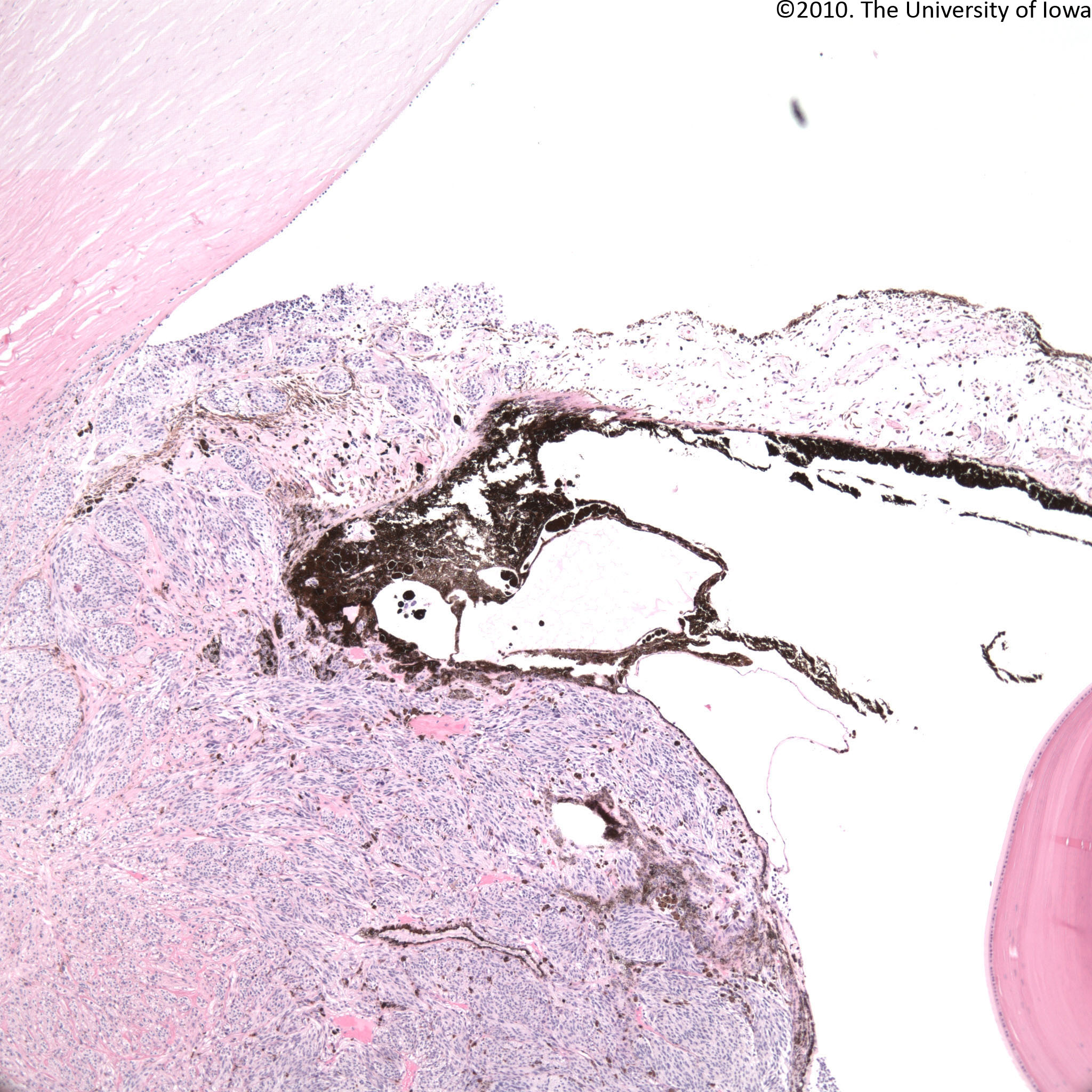
Histopathology: Microscopically, the inferior angle and iris structures are infiltrated by tumor cells. Tumor cells extend into the root of the iris and consist of nests of spindle A and B melanoma cells with little to no pigment. Tumor cells demonstrate a fascicular and nesting pattern in the iris and ciliary body. The majority of the mass is located in the region of the ciliary body and replaces ciliary muscle and epithelium. The mass breaks through the ciliary epithelial basement membrane and grows inward toward the vitreous. A few areas of erosion of the basement membrane are present at the apex of the tumor with spillage of a few tumor cells into the overlying vitreous. The lesion extends posteriorly into the choroid where there is marked sclerosis associated with tumor cells. The tumor extends just beyond the equator of the globe. The basal dimension of the tumor is approximately 16 mm and the apical height is 6 mm. Focal areas of retinal pigment epithelial hyperplasia and metaplasia are present overlying the tumor and a small serous detachment of the retina is present over the posterior portion of the tumor. Occasional drusen are seen along Bruch's membrane overlying the tumor (suggestive that some component of the lesion has been chronic). PAS without hematoxylin demonstrates the presence of linear and arc-like intrinsic microvascular patterns. There are two mitoses in 40 high-power fields. Scattered melanin-containing macrophages are present throughout the tumor, particularly surrounding blood vessels. Ciliary epithelium can be seen engulfed within the tumor in many regions. The tumor does demonstrate focal areas of scleral invasion that reach approximately 50% in depth. MART-1 is positive in tumor cells when compared with appropriate positive and negative controls.
Histopathologic diagnosis
1. Ciliochoroidal malignant melanoma with the following features:
2. Peripheral exudative retinal detachment overlying tumor.
Discussion: In our patient, the clinical differential diagnosis included amelanotic choroidal melanoma, choroidal metastasis, and an inflammatory lesion (such as granulomatous disease). Even though the ultrasound was suggestive of melanoma, other clinical features made the diagnosis more complicated. First, the lesion was amelanotic ophthalmoscopically. Most choroidal melanomas have some pigmentation. Second, the patient was only 31, which is younger than average for this disease. Shields lists an extensive differential to be considered for an amelanotic choroidal mass (see below).
Posterior uveal malignant melanoma (that arises in the choroid and ciliary body) is the most common primary intraocular malignancy in adults (Albert and Jakobeic 1994). Most uveal melanomas occur in the choroid (85%) and some occur in the ciliary body (10%) and iris (5%). Overall, posterior uveal melanoma is a highly aggressive neoplasm, and about half of patients die of disseminated tumor within 10 to 15 years of diagnosis.
The clinical presentations of posterior uveal melanomas are determined by the location and size of the tumor (see Symptoms section below). In general, the farther away the tumor is from the optic nerve and fovea, the larger size it can reach before the patient notices a visual field defect. Ciliary body melanomas may be asymptomatic in the early stages as they remain hidden behind the iris. The typical choroidal melanoma is a pigmented, elevated, dome-shaped, sub-retinal mass (Shetlar 2007). The degree of pigmentation ranges from totally amelanotic to dark brown. Serous detachment of the retina is common.
Choroidal melanomas, when small, are confined to the uvea by Bruch's membrane and the tough collagenous sclera and are usually disc shaped. With enlargement of the tumor, the relatively weak Bruch's membrane eventually ruptures. This phenomenon allows the by now medium-sized tumor to expand into the subretinal space, first forming a collar button and then (with proportionally more subretinal than choroidal expansion) a mushroom appearance. Large, nodular tumors may eventually invade and destroy adjacent intraocular tissues, filling the posterior chamber. Subsequent enlargement may displace the iris and lens anteriorly, causing progressive narrowing of the anterior chamber angle and eventual obliteration of the anterior chamber.
Extraocular extension can be a consequence of tumor expansion. The sclera is a major barrier to expansion, so when tumors extend beyond the globe they usually do so at points where blood vessels (vortex veins, ciliary arteries, etc.) penetrate the sclera. Spreading tumor cells, however, will usually spread through the scleral channels around the vessels rather than within the vessels themselves; intravascular invasion is rarely seen in vortex veins. The relatively low frequency of observed intravascular tumor invasion of vortex veins probably indicates that invasion of small intratumoral blood vessels is the most important source of hematogenous metastasis. Peripapillary choroidal malignant melanomas often invade the optic nerve head, but retrolaminar invasion of the optic nerve is rare, unlike the extension pattern of retinoblastoma.
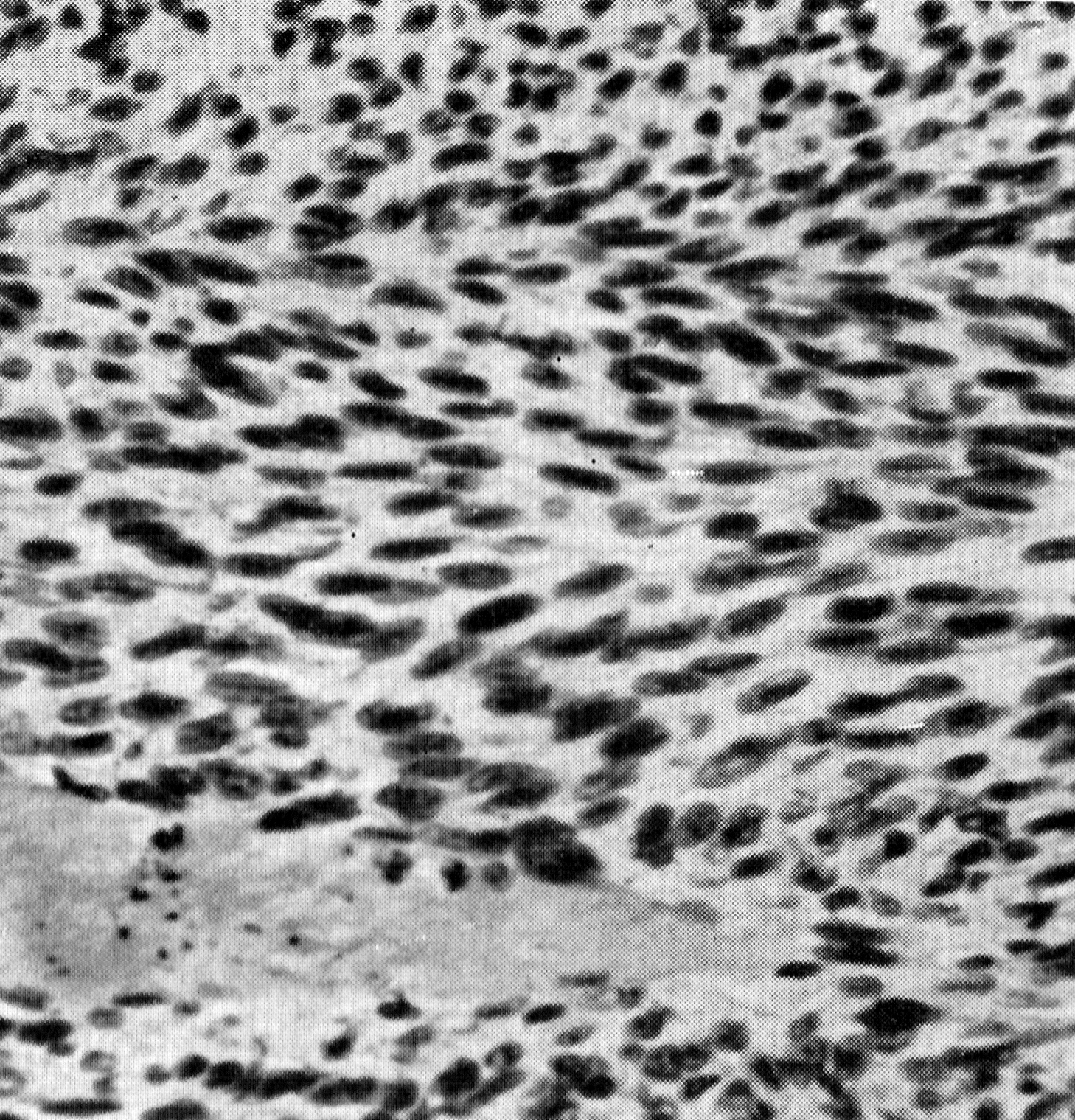
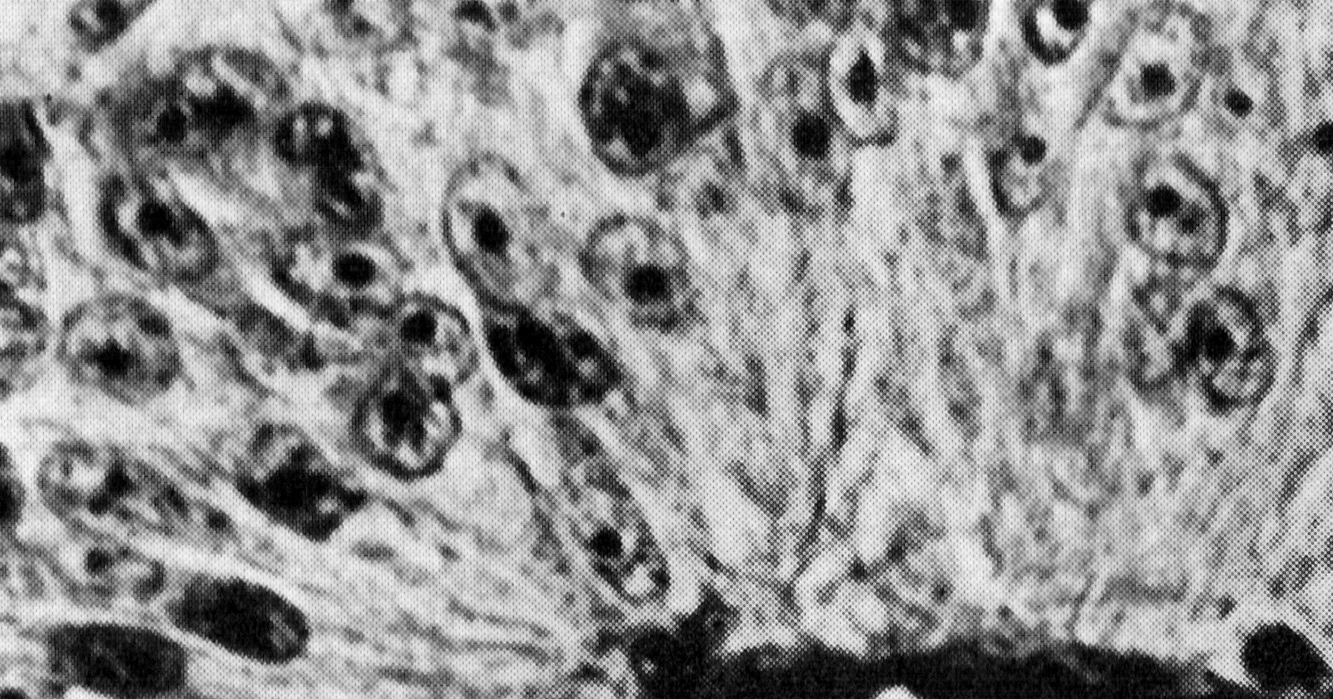
The most important microscopic feature is the morphology of the tumor cells, and this remains one of the most reliable indicators of prognosis for individual tumors (Albert and Jakobeic 1994). In 1931, Callender described two main types of tumor cell type, spindle cells and epithelioid cells, and identified two subtypes of spindle cells on the basis of nuclear characteristics. The resulting three cell types are spindle A, spindle B, and epithelioid (see Figure 5).
| Figure 5A: Spindle A cells have a slender nucleus with a fold | Figure 5B: Spindle B cells are more plump with prominent nucleoli |
|
|
|
|
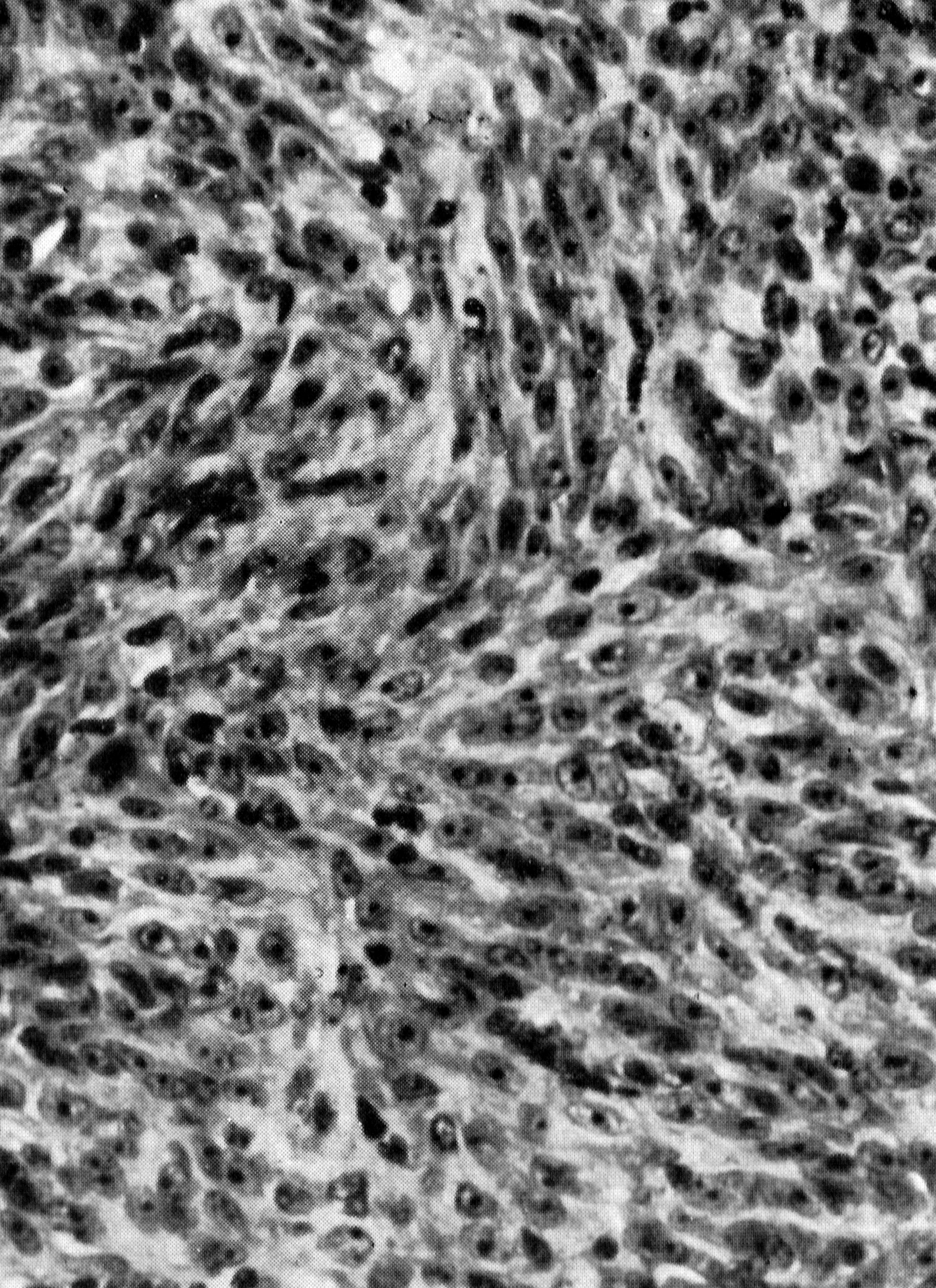
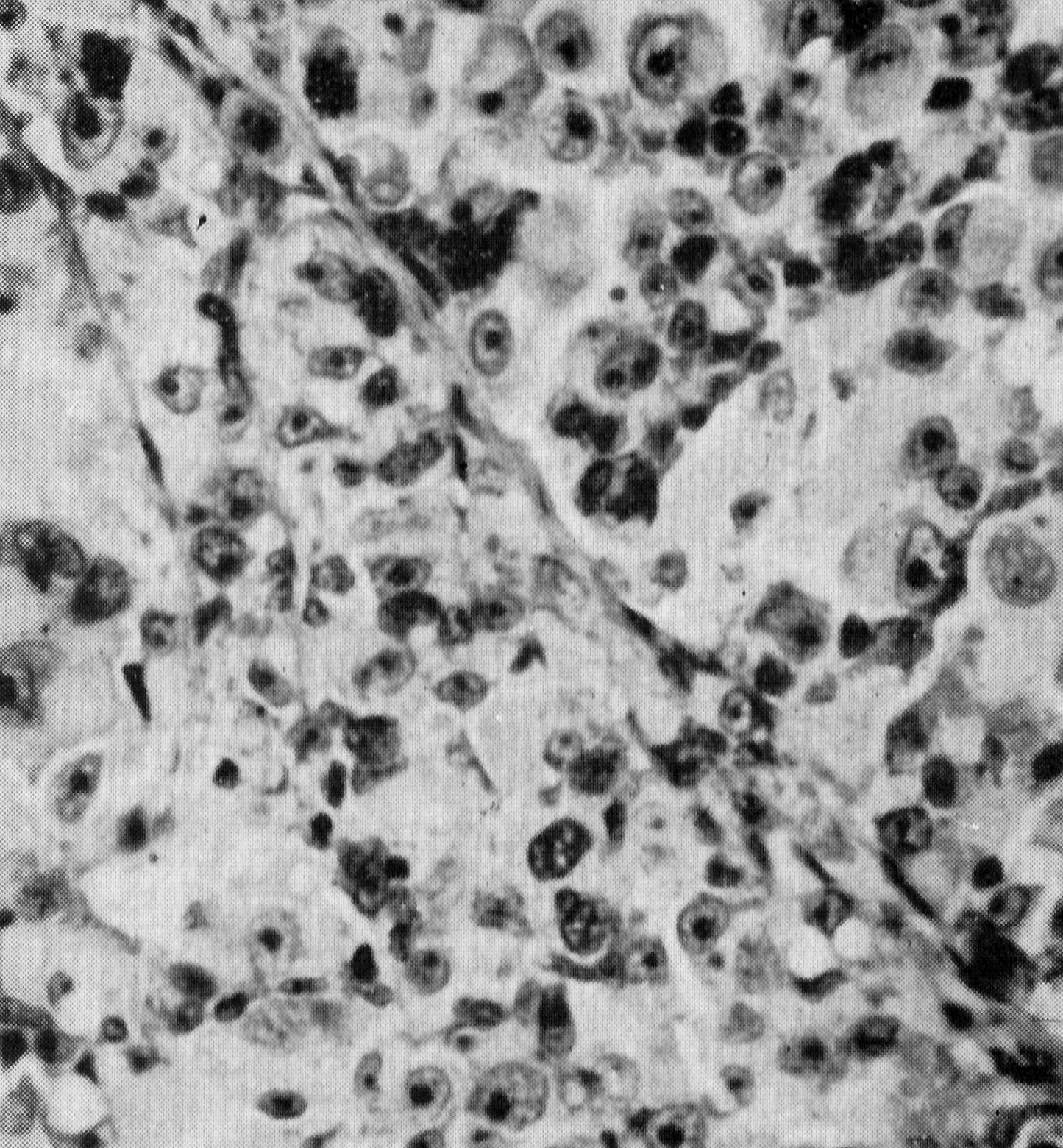
Figure 5C: Epithelioid cells have more cytoplasm and a rounded shape with large nuclei and prominent nucleoli |
Figure 5D: Fascicular cells showing a palisading pattern above vessel |
|
|
(Click on any image for higher resolution.) Images from Callender 1931 |
|
The modified Callender classification contains A) spindle cell melanoma, B) epithelioid melanoma, and C) mixed-cell type (mixture of spindle and epithelioid cells). Occasionally, a melanoma undergoes extensive necrosis, which precludes proper classification. Spindle cell melanoma has the best prognosis and epithelioid melanoma the worst. Melanomas of the mixed cell type have an intermediate prognosis and totally necrotic melanomas assume the same prognosis as mixed cell melanomas (Shields 1992). More recently, intrinsic tumor microvascular patterns have been studied and shown to have prognostic significance. Tumors with more complex microvascular patterns such as networks of closed vascular loops, are associated with an increased incidence of subsequent metastasis (Folberg 1997).
Historically, enucleation has been the gold standard in the treatment of intraocular tumors. In 1882, Fuchs wrote that all intraocular melanomas were treated by enucleation and the only untreated cases were in the older literature. Today, enucleation remains appropriate for many large choroidal melanomas particularly when useful vision is lost. The past hypothesis that surgical manipulation might lead to potential release of malignant cells into the bloodstream and orbital soft tissues during the procedure is no longer accepted today.
Some investigators have advocated preenucleation radiation of the eye as a way to improve survival. However, according to the Collaborative Ocular Melanoma Study (COMS), external beam radiation treatment (EBRT) did not positively or negatively affect the survival of patients with large choroidal melanomas (> 16.0 mm basal diameter or > 10.0 mm apical height) who were randomized to enucleation alone versus EBRT followed by enucleation This study established the appropriateness of primary enucleation alone in managing large choroidal melanomas that are not amenable to globe-conserving therapy (COMS 1998).
Today, the application of a radioactive plaque to the sclera overlying an intraocular tumor is probably the most common method of treating medium-sized uveal melanomas (6.0-16.0 mm basal diameter or 2.5-10.0 mm apical height). It allows the delivery of a high dose of radiation to the tumor and a relatively low dose to the surrounding structures. Radioactive plaques are sutured temporarily to the sclera underlying the melanoma and left in place for 3-7 days. Though many radioactive isotopes may be used, radioactive iodine (I-125) seeds are frequently the isotope of choice in plaques today. After brachytherapy the tumor gradually flattens over 2-3 years, usually leaving behind a residual pigmented mass surrounded by choroidal atrophy. Regrowth is diagnosed in only 4-5% of the treated tumors. As long as there is no tumor regrowth, further treatment is not needed. Late radiation-related complications (especially optic neuropathy and radiation retinopathy) are visually limiting in as many as 50% of patients.
The theoretical advantage of enucleation over globe-sparing treatments is a reduced risk of metastatic spread. However, the COMS group (where medium-sized tumors were treated with either I-125 brachytherapy or enucleation) found that the mortality rates following brachytherapy did not differ from the mortality rates following enucleation for up to 12 years after treatment (COMS 2001).
The choice of therapy depends on several factors. The most important are the size and location of the tumor, the patient's age, general health, occupation and motivation and the available skills and equipment. The results from the Collaborative Ocular Melanoma Study provide a framework for patient discussions.
In the future, it is expected that the treatment of primary uveal melanoma will be mainly directed toward eliminating subclinical metastasis (Shields 2008). Ideally, management would involve early detection of small uveal melanoma with prompt treatment combined with systemic therapy (Shields 2002). As effective systemic therapies, in the form of chemotherapy, immunotherapy, and/or gene therapies are identified, the management of uveal melanoma will be improved.
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENTA complete review of the details of ocular melanoma therapy will not be attempted here. Some basic options and principles of therapy include:
Collaborative Ocular Melanoma Study (COMS) findings can be found at: www.jhu.edu/wctb/coms |
We thank Nasreen Syed, MD, of the University of Iowa, F.C. Blodi Ocular Pathology Laboratory for providing the pathology and histopathology photographs in this paper.
Albert, DM, Jakobiec FA. Principles and Practice of Ophthalmology: Clinical Practice. Philadelphia: W.B. Saunders, 1994.
Callender GR. Malignant melanotic tumors of the eye: a study of histologic types in 111 cases. Trans Am Acad Ophthalmol Otolaryngol 1931;36:131-142.
Chapter 17: Melanocytic Tumors, In: Shetlar DJ, et al. Section 4. Ophthalmic Pathology and Intraocular Tumors, 2007-2008 Basic and Clinical Science Course. San Francisco: American Academy of Ophthalmology, 2007; p.259-275.
Chapter 9: The Uveal Tract, In: Spalton DJ, et al. Atlas of Clinical Ophthalmology, Third edition. New York: Elsevier Limited, 2005; p.267-285.
The Collaborative Ocular Melanoma Study Group. The collaborative ocular melanoma study (COMS) randomized trial of pre-enucleation radiation of large choroidal melonomas. COMS report no.10. Americal Journal of Ophthalmology 1998;126:779-796.
The Collaborative Ocular Melanoma Study Group. The COMS randomized trial of iodine 125 brachytherapy for choroidal melanoma. Arch Ophthalmol 2001;119:969-982.
Folberg R, Mehaffey M, Gardner LM, et al: The microcirculation of choroidal and ciliary body melanomas. Eye 1997;11:227-38
Garcia-Valenzuela, Enrique. Choroidal Melanoma. eMedicine.com. http://emedicine.medscape.com/article/1190564-overview, 2008 [cited July 18, 2010].
Shields JA, Shields CL. Posterior uveal melanoma. Clinical and pathologic features. In: Shields JA, Shields CL, eds. Intraocular tumors. A text and atlas. Philadelphia: WB Saunders, 1992; p.117-136.
Shields JA, Shields CL. Posterior uveal melanoma. In: Shields JA, Shields CL, eds. Intraocular tumors. An atlas and textbook. Second edition. Philadelphia: WB Saunders, 2008; p.85-177.
Shields JA. Management of posterior uveal melanoma. Past, present, future. Editorial. Retina 2002;22:139-142.
Pham LTL, Graff JM, Boldt HC. Posterior Uveal (Ciliary Body and Choroidal) Melanoma. EyeRounds.org. July 27, 2010; Available from: http://www.EyeRounds.org/cases/117-Posterior-Uveal-Melanoma.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links