
Chief Complaint: Incidental pigmented lesion identified on dilated exam
History of Present Illness: A 58-year-old female was referred by her optometrist for the evaluation of a pigmented lesion in her right eye (OD) found incidentally on dilated exam. The last dilated exam was performed 3 years prior and was reportedly normal at that time. The patient denied change in vision, flashes, floaters, and pain.
Past Ocular History: Myopia and presbyopia
Past Medical History: Hypertension, no known primary malignancies
Best corrected visual acuity: 20/20 OD, 20/20 -2 left eye (OS)
Applanation tonometry: 15 mmHg OD, 15 mmHg OS
Confrontation visual fields: Total superotemporal deficiency OD, full OS
Motility/Alignment: Full, orthophoric
Slit lamp exam: no sentinel vessels, anterior chamber deep and quiet, normal iris without rubeosis, 1+ nuclear sclerotic cataract in both eyes (OU); 1+ pigmented anterior vitreous cell OD, no vitreous cell OS.
Figure 1: (click image for higher resolution)
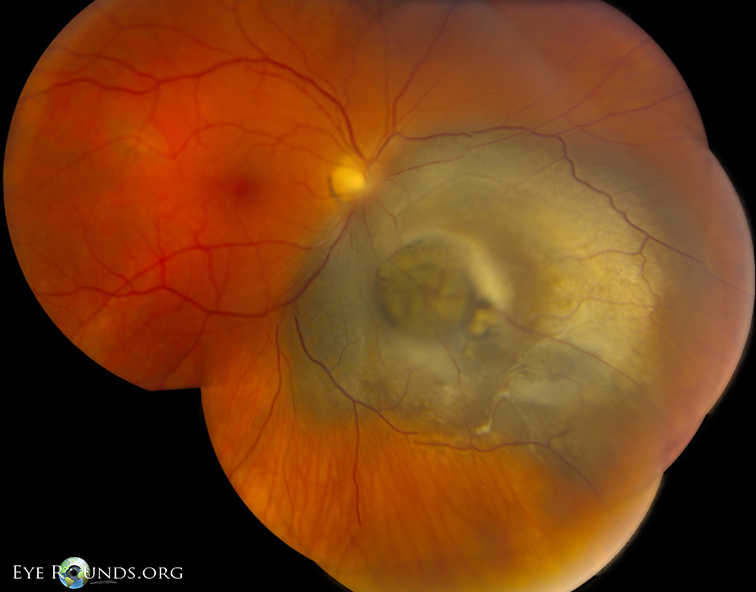
Elevated, peripapillary, moderately pigmented collar button shaped choroidal mass with mild overlying RPE metaplasia inferonasal to the optic disc. The mass measures 14 x 11 x 6 mm and overhangs the disc.
There is an exudative retinal detachment of the inferior 20% of retina when the patient sits upright.
Figure 2: (click image for higher resolution)
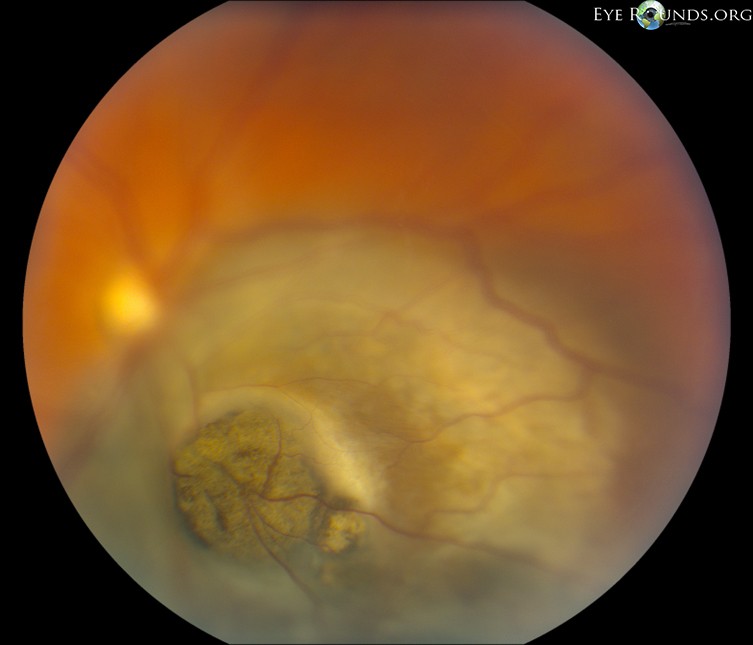
Close-up of lesion showing disruption of Bruch's membrane and nodular tumor eruption in a "collar button" shape.
Figure 3: (click image for higher resolution)
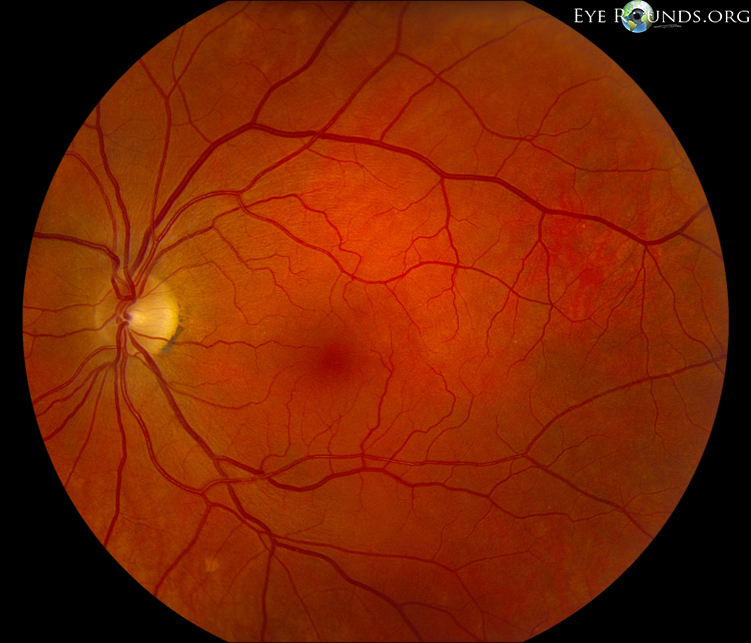
There are a few small hard drusen in the macula. The fundus is otherwise unremarkable.
Figure 4: (click image for higher resolution)

B-scan ultrasonography revealed an irregular, peaked choroidal mass 6 mm in height x 13 mm at its base. It had low to medium reflectivity and 2+ internal vascularity. An exudative retinal detachment is appreciated inferior to the mass.
Figure 5: (click image for higher resolution)

A-scan ultrasonography demonstrated low to medium internal reflectivity.
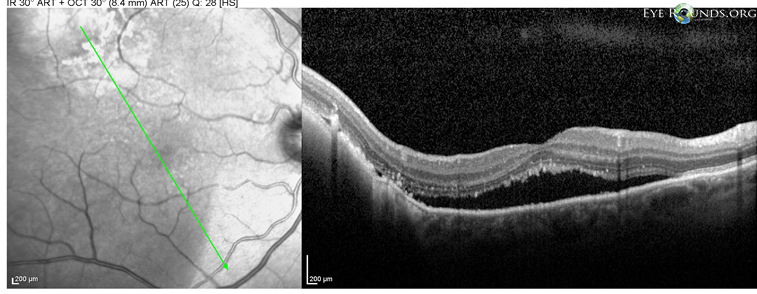
Figure 6: (click image for higher resolution)
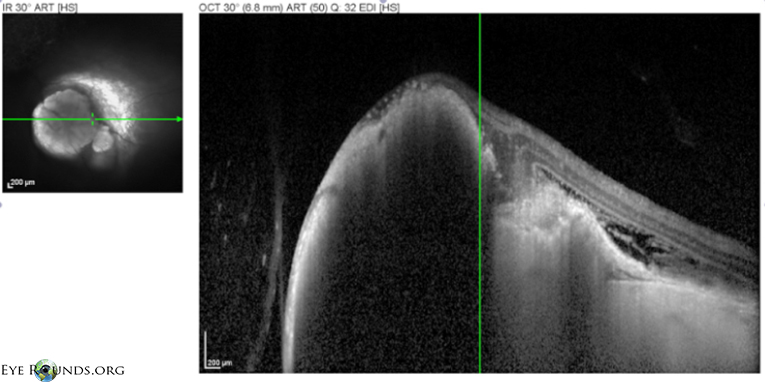
OCT showed a choroidal mass with disruption the RPE and Bruch's membrane and associated subretinal fluid.
Based on the clinical appearance and echographic findings, the patient was diagnosed with a medium-sized peripapillary choroidal melanoma with secondary exudative retinal detachment inferiorly OD. The patient underwent metastatic workup for tumor staging. The outside complete blood count (CBC), basic metabolic panel (BMP), liver function tests (LFTs), chest x-ray, and abdominal ultrasound were negative for evidence of metastasis. The patient was counseled on management options including brachytherapy, charged particle radiation, enucleation, observation, and alternative therapies. The likely development of profound vision loss due to radiation optic neuropathy following radiation treatment was also discussed. The patient elected to have an enucleation with prosthesis.
Enucleation was performed by oculoplastic surgeons at the University of Iowa. Pathologic evaluation of the globe confirmed the mass was a mixed cell choroidal melanoma with >10% epithelioid cells and <90% spindle cells. The mass was positive for invasion of Bruch's membrane, perineural invasion of choroidal nerve twigs, and minimal tumor infiltrating lymphocytes. No vascular, ciliary body, or extraocular invasion was noted and the optic nerve margins were free of tumor. It was classified as American Joint Committee on Cancer (AJCC) stage pT3a and grade pG2.
The patient tolerated surgery well and later received an ocular prosthesis. Due to the clear margins and lack of evidence indicating distant metastasis, no further treatment for choroidal melanoma was necessary. The patient was counseled to undergo yearly eye exams with annual tumor surveillance, consisting of a physical exam, liver function studies, and imaging of the liver with ultrasonography or MRI with contrast.
Figure 7: (click image for higher resolution)

Gross specimen of the globe after enucleation showing posterior choroidal mass with adjacent retinal detachment.
Figure 8: (click image for higher resolution)
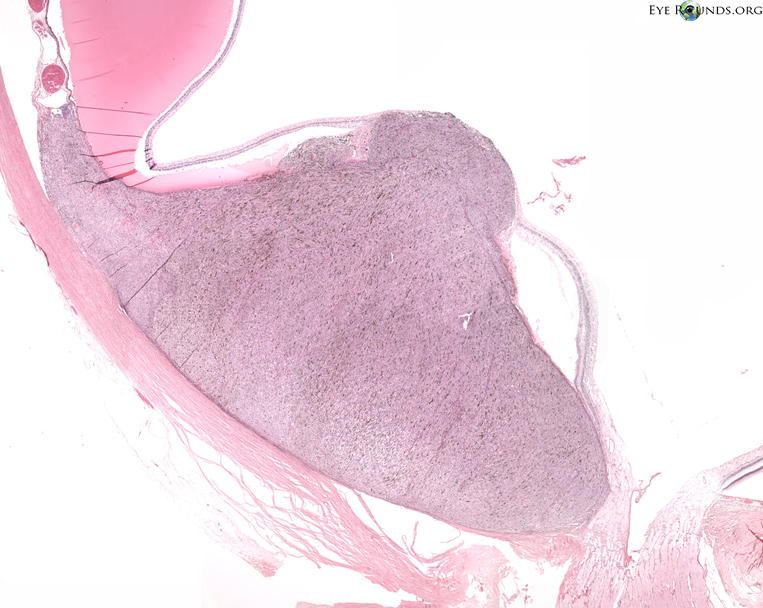
Histolopathology demonstrating the choroidal melanoma which disrupts Bruch's membrane forming a "collar button" appearance. An exudative retinal detachment is present adjacent to the tumor anteriorly. Hematoxylin and eosin, original magnification 10x
Uveal melanoma is the most common primary intraocular malignancy in adults. It arises from the neuroectodermal melanocytes within the uveal tract, most commonly involving the choroid (85%) (1). Choroidal melanoma presentation peaks at the age of 60 years with a higher incidence in Caucasians. Tumors can be asymptomatic and detected incidentally on fundus exam or symptomatic with decreased visual acuity, blurring, metamorphopsia, flashes, floaters or visual field loss (2).
It is important to be able to distinguish between melanoma and pseudomelanomas, like choroidal nevus, choroidal metastasis, melanocytoma, or hyperplasia of the retinal pigmented epithelium (RPE). Physical appearance of the lesion on fundus exam can help differentiate the lesion. Nevi are usually flat, <6 mm in diameter, and may have overlying drusen. Choroidal metastases are typically amelanotic, lobulated, and associated with more subretinal fluid than melanomas of a similar size. Melanocytomas are black, often extend onto the optic nerve and invade the nerve fiber layer, giving a feathered appearance. Congenital hyperplasia of the RPE (CHRPE) is typically a sharply demarcated pigmented lesion with scalloped margins (3).
There are several clinical elements that suggest choroidal melanoma on exam:
A useful mnemonic can be used to help remember these features,
"To Find Small Ocular Melanoma" (TFSOM) (4). This corresponds to:
Figure 9 : (click image for higher resolution)
A:

B:
A different patient presenting with visual symptoms and a pigmented choroidal mass highly suspicious for choroidal melanoma. (A) Biconvex shape with orange pigment overlying the mass and subretinal fluid inferonasal to the lesion. (B) OCT shows subretinal fluid adjacent to the lesion.
Echography is the most useful ancillary test for supporting the clinical diagnosis of choroidal melanoma. The A-scan assesses internal reflectivity, vascularity, and elevation. Melanomas characteristically display low internal reflectivity and a solid tumor pattern. Tumors that have erupted through Bruch's membrane show high amplitude internal reflectivity corresponding to the outer cap followed by low amplitude internal reflectivity corresponding to the basal region. The B-scan demonstrates the size, position, and thickness of the lesion, and can detect extrascleral extension. Most choroidal melanomas present with an exudative retinal detachment that can be imaged on B-scan (5).
Management is dependent on the tumor size, location, and effect on the patient's vision. Conservative therapy that aims to salvage the globe is first-line. There is a wide variety of treatment options for choroidal melanoma, including (6):
The vast majority of patients (98%) with choroidal melanoma have no detectable metastatic disease, but a metastatic workup should be completed for every suspected diagnosis including a complete physical exam, CBC, LFTs, chest x-ray, and imaging of abdominal organs (usually ultrasonography for routine monitoring) (7). Metastatic disease is spread hematogenously with preferential spread to the liver, and occasional involvement of the lungs, bone, skin, or brain. Despite advancements in melanoma detection and treatment, prognosis has remained relatively stable. Five year all-cause survival from diagnosis is 90% for small melanomas, 70% for medium, and 50% for large. Disseminated melanoma at the time of diagnosis is usually fatal within one year (8).
Melanomas are classified based on histopathology as per the Modified Callender Classification, with a strong correlation between microscopic features and prognosis. Lesions can contain spindles cells, epitheloid cells, or both. Spindle cell melanomas have the best prognosis, epithelioid cell melanomas have the least favorable prognosis, and mixed-cell melanomas have an intermediate prognosis (9). Tumors made entirely of spindle A cells are nevi.
Figure 10: (click image for higher resolution)
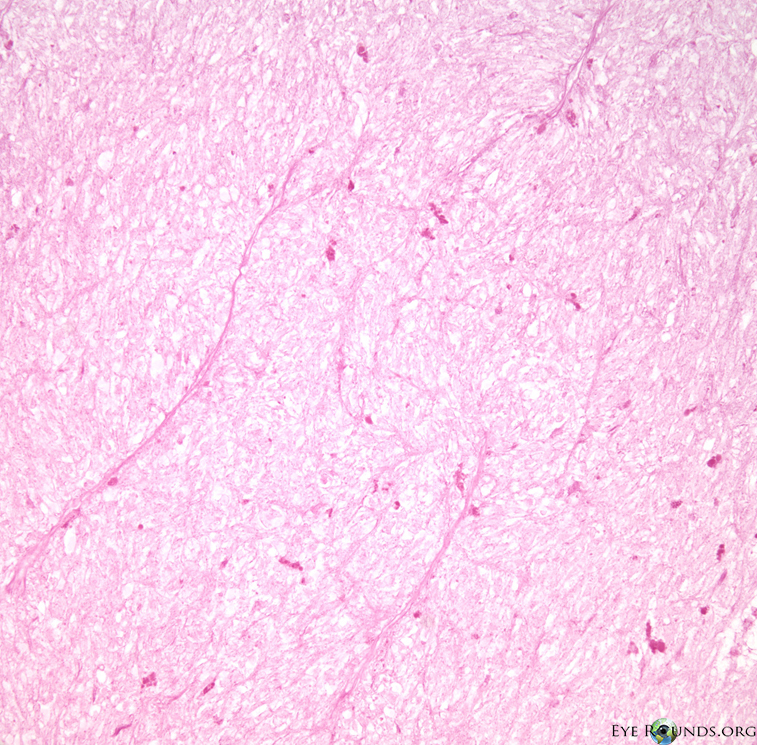
Spindle A cells
Melanin bleach, original magnification 300x
Elongated cells with slender nuclei and indistinct nucleoli.
A longitudinal fold may be present in the nuclei.
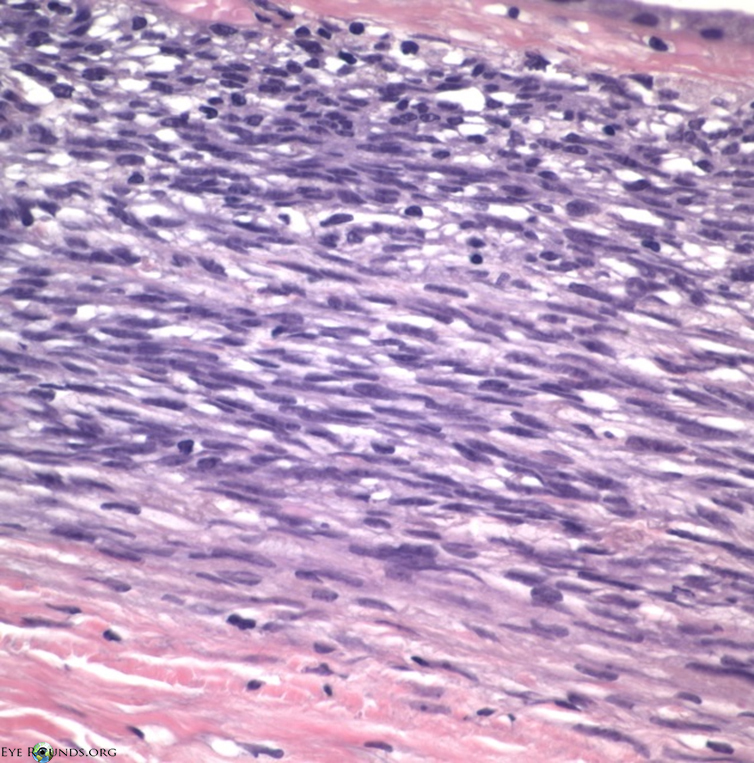
Spindle B cells
Hematoxylin and eosin, original magnification 300x
Ellipsoid cells with a more plump nucleus, coarser chromatin, and more prominent nucleoli compared to spindle A cells
There is a higher nuclear:cytoplasm ratio than spindle A cells.

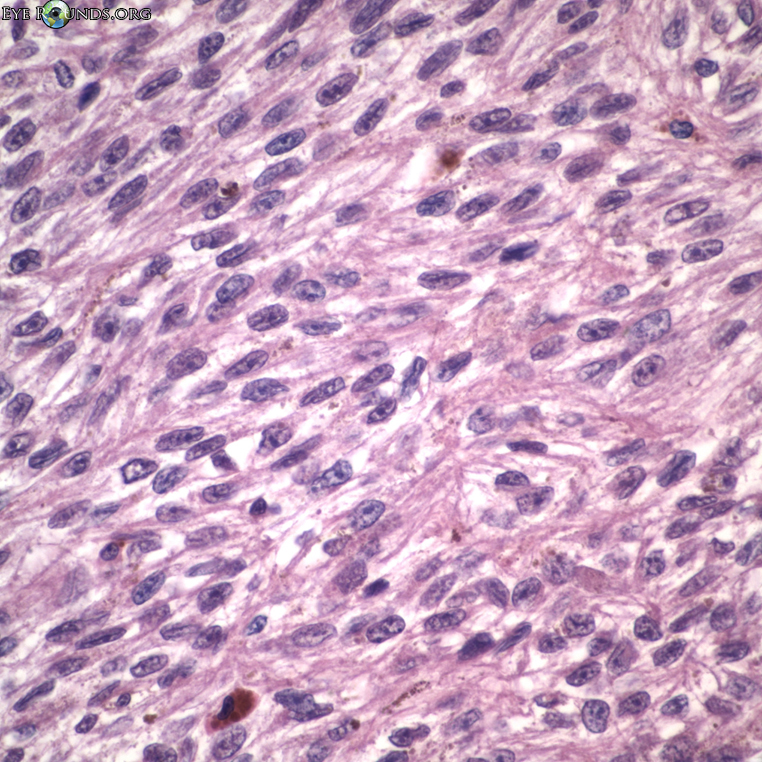
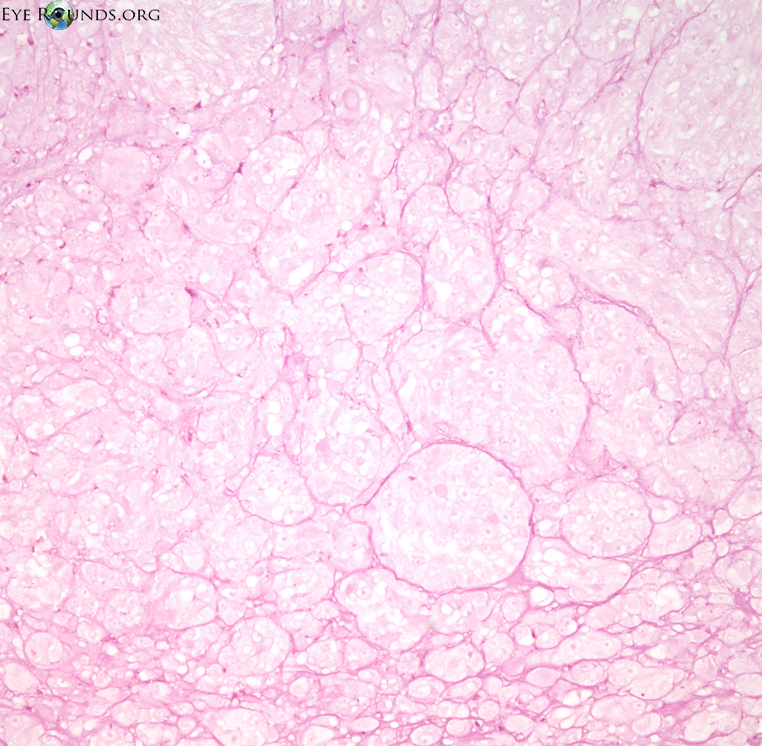
Epithelioid cells
Hematoxylin and eosin, original magnification 300x
Pleomorphic polyhedral cells with eosinophilic cytoplasm and a larger, rounder nucleus than spindle cells.
The nuclei have distinct, irregular nuclear membranes with large, eosinophilic nucleoli.
These cells are often discohesive, and some may be bizarre or multinucleated.
Epithelioid cells usually have greater mitotic activity than spindle-type cells.
Other histopathologic features can also be associated with poor prognosis and metastasis including (10,11):
Figure 11: (click image for higher resolution)
Histopathology demonstrating choroidal melanoma vascular patterns. Vascular patterns can range from silent (no vessels) to networks that consist of at least 3 back-to-back vascular loops. More complicated vascular patterns carry a poorer prognosis. (A-top image) Parallel-oriented straight vessels. (B-bottom image) Complex vascular pattern with a large fibrovascular network. Melanin bleach and Periodic Acid Schiff without hematoxylin, original magnification 100x
 A
A
 B
B
Choroidal melanoma has a typical pattern of spread as the tumor enlarges. It begins as a brown dome-shaped lesion that causes early exudative subretinal detachment. It can expand to disrupt Bruch's membrane and herniate into the posterior chamber, forming the classic "collar button" or "mushroom" configuration. Invasion of scleral vasculature allows orbital spread. Distant metastatic disease occurs hematogenously by penetration into the vortex veins. Optic nerve invasion rarely occurs, usually only with large peripapillary melanomas.
Epidemiology
|
Histology
|
Prognostic CriteriaClinical features associated with poorer prognosis:
Pathologic features (associated with poorer prognosis):
American Joint Committee on Cancer TNM Staging (www.mmmp.org) |
Treatment
|
>Mullaney S, Vislisel J, Maltry A, Boldt HC. Choroidal Malignant Melanoma: 58-year-old female with pigmented retinal lesion and exudative retinal detachment. EyeRounds.org. July 8, 2014; available from https://eyerounds.org/cases/190-choroidal-malignant-Melanoma.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
