Chief Complaint: "My vision is much worse since my delivery."
One week after an otherwise uncomplicated cesarian section, a G2P2 24-year-old woman with type 1 diabetes was evaluated by the University of Iowa Retina Service for decreased vision and multiple new floaters in both eyes. She identified the onset of dramatically decreased vision in both eyes that began at the time of the delivery of her most recent child.
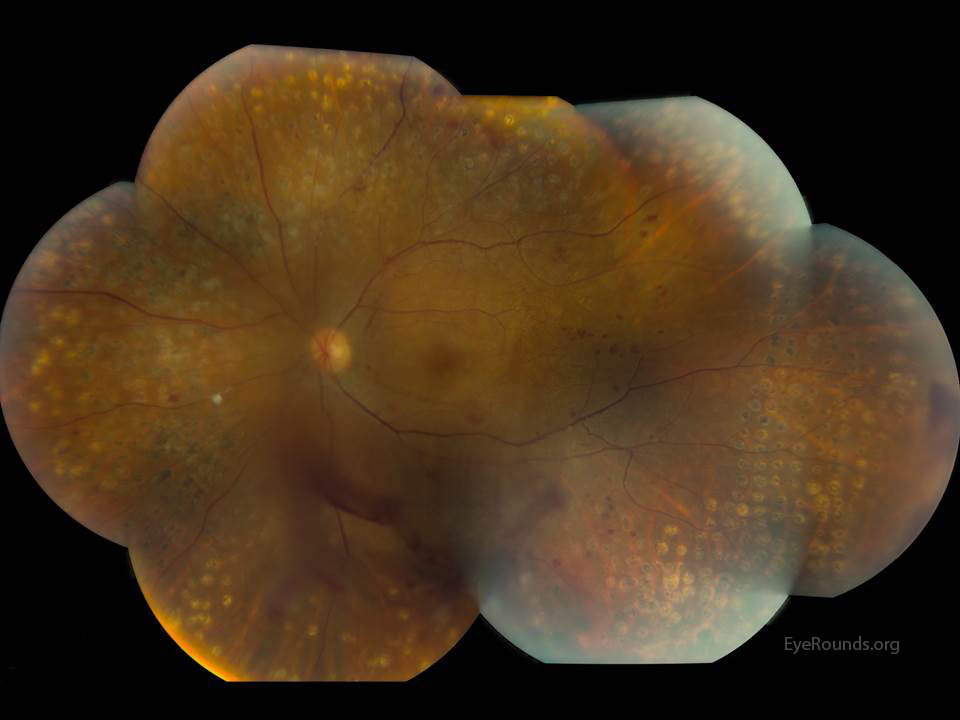
During the patient's first pregnancy three years prior, her previously diagnosed severe non-proliferative diabetic retinopathy progressed to proliferative diabetic retinopathy with new-onset vitreous hemorrhage and she developed clinically significant diabetic macular edema in the left eye. To avoid fetal exposure to anti-vascular endothelial growth factor (anti-VEGF), anti-VEGF injections were withheld at that time, and the patient was instead treated with panretinal photocoagulation. Given her high risk for ocular complications, the patient had been closely monitored by the Retina Service throughout the first trimester of this second pregnancy; however, she was lost to follow-up thereafter.
|
|
|
|
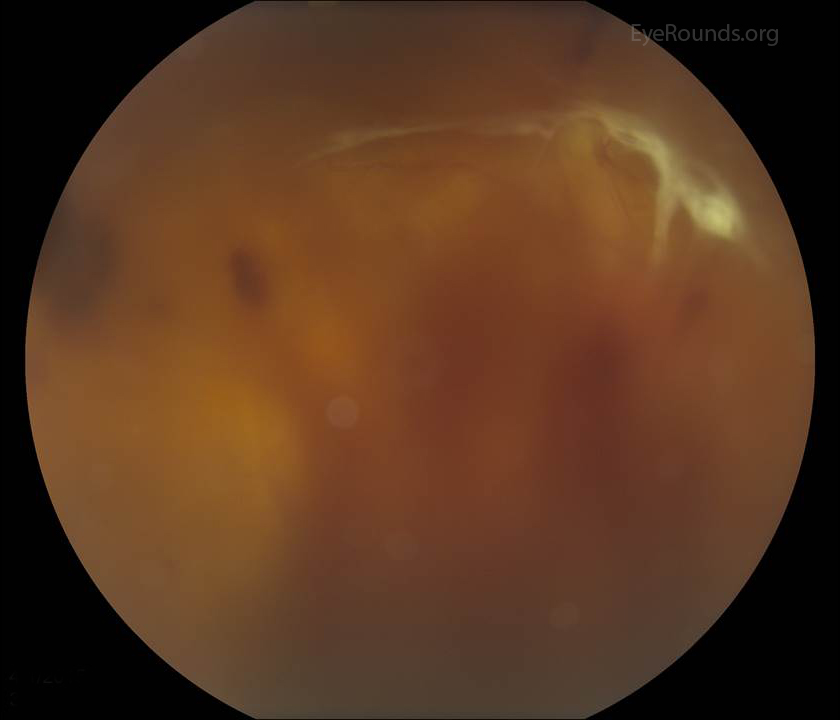
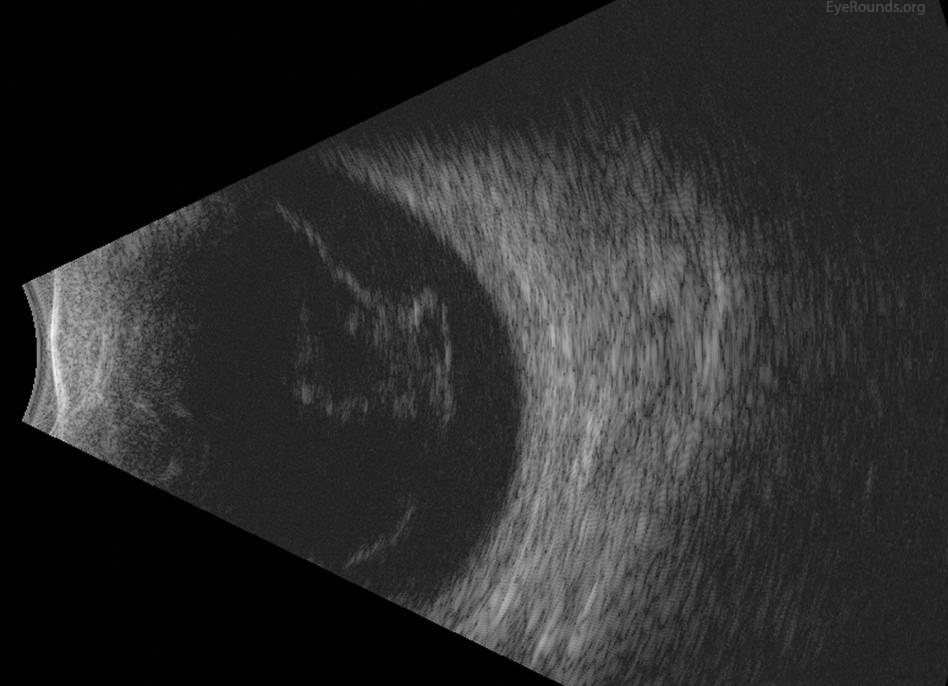
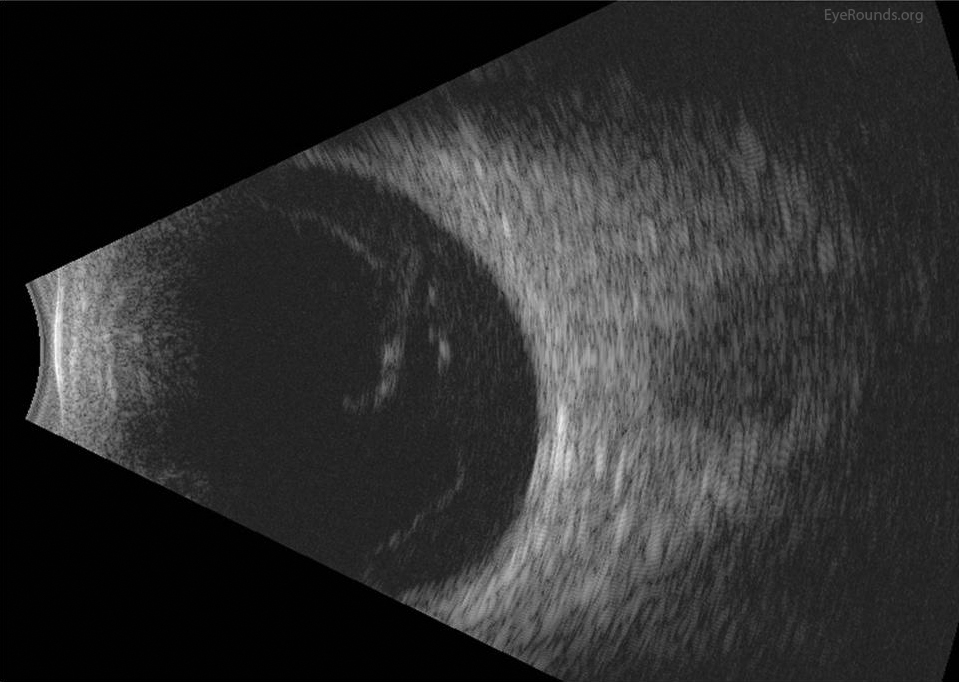 OD: Dense, dispersed vitreous hemorrhage. Dense subvitreal hemorrhage. Extensive posterior vitreous detachment with tractional insertions superiorly and around optic disc. No retinal detachment detected. |
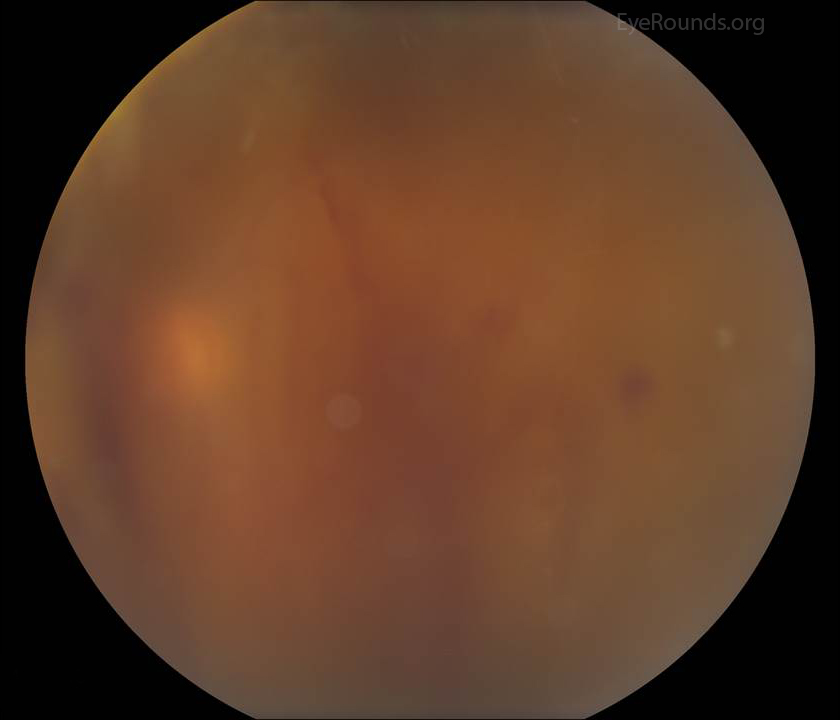
 OS: Moderately dense, dispersed vitreous hemorrhage. Total, mobile posterior vitreous detachment. No traction or retinal detachment detected. |
New onset bilateral vitreous hemorrhages in the setting of progression of proliferative diabetic retinopathy in pregnancy
The patient's exam and imaging was consistent with vitreous hemorrhages in both eyes related to progression of proliferative diabetic retinopathy. Given that this resulted in poor vision bilaterally and thus placed the patient's safety at risk and made it difficult for her to function, surgical intervention was recommended. The case was discussed with the patient's obstetrician, who allowed her to proceed with surgery. She was scheduled for a pars plana vitrectomy in her right (worse) eye shortly thereafter.
Ocular effects of pregnancy range from physiologic, self-limited changes to pathologic changes requiring surgical intervention. Pregnancy alone does not cause any detrimental long-term effects on the retina (1). Diabetic retinopathy is the most common preexisting ocular condition that may be worsened by pregnancy. The period of accelerated progression of diabetic retinopathy may persist throughout the months following delivery. Risk factors for the progression of diabetic retinopathy during pregnancy include longer duration of diabetes, poor glycemic control, greater severity of retinopathy at conception, the presence of hypertension or preeclampsia, and pregnancy itself (2). Presence of angiopathy in the kidneys may also correlate with the severity of retinopathy.
Because diabetes mellitus type I has an earlier onset (and thus a longer duration prior to pregnancy) than type II, women with diabetes mellitus type I are at a higher risk for progression during pregnancy than those with type II (1). Women who are diagnosed with gestational diabetes are not at any increased risk for the development of diabetic retinopathy during pregnancy (3). Women with diabetes who develop diabetic retinopathy during pregnancy (but had no documented evidence of diabetic retinopathy prior to pregnancy) have a high rate of spontaneous postpartum regression. Patients with severe proliferative or non-proliferative diabetic retinopathy prior to conception have a higher risk of progression of disease during pregnancy; however, some cases of severe proliferative disease progression may eventually show signs of regression in the postpartum period (4).
Although glycemic control is a modifiable risk factor, it should be noted that brisk tightening of glycemic control has been associated with a greater risk of diabetic retinopathy progression (2). Therefore, despite the possibility of progressive changes reversing in the postpartum period, it is advisable to stabilize ocular disease prior to pregnancy whenever possible.
Of note, increased severity of diabetic retinopathy has been correlated with poor fetal outcomes. The incidence of congenital malformations is higher in patients with proliferative changes (1).
The exact mechanism underlying the worsening of proliferative diabetic retinopathy during pregnancy is unknown; several contributing factors may be involved. Recent studies suggest that a decrease in both retinal venous diameter and retinal blood flow may develop during pregnancy in diabetic patients. It is hypothesized that these changes may further worsen retinal ischemia and hypoxia. Contrary to this theory, other studies have reported increased retinal blood flow in pregnancy, and conclude that this hyperperfused state exacerbates vessel stress and vulnerability in an already compromised retinal vessel environment, causing endothelial damage and thus, worsening diabetic retinopathy (5, 6, 7).
Another theory is related to the several hormonal changes that occur during pregnancy. Specific hormones affecting the eye include human placental lactogen, estrogen and progesterone. Elevated levels of these hormones cause vascular changes that may contribute to the progression of diabetic retinopathy. Human placental lactogen may have the largest impact on progression of disease as it is massively produced and has functions similar to growth hormone (1).
Diabetic women of childbearing age who are planning to become pregnant should receive a dilated fundus exam prior to conception with special attention focused upon detecting diabetic retinopathy. Mydriasis is best achieved using tropicamide or phenylephrine HCL, both of which are category C drugs (the potential benefit may justify use, despite the potential risk) (1). A first trimester eye exam should be performed, with follow-up care dependent on the degree of retinopathy observed (3). If no retinopathy to moderate non-proliferative retinopathy is present, the patient should be reexamined in 3-12 months. Severe non-proliferative retinopathy or any degree of proliferative retinopathy requires follow-up every one to three months until delivery (8). If there was disease present prior to pregnancy, regardless of the severity, a six-month post-partum follow-up appointment is recommended.
The standard of care for treatment of proliferative diabetic retinopathy is laser photocoagulation therapy (3). Pregnancy is not an indication to delay such treatment. If a pregnant woman develops severe non-proliferative changes, immediate laser photocoagulation is indicated to prevent proliferative changes (9).
Very little data is available on the effects of intravitreal anti-vascular endothelial growth factor (anti-VEGF) injections during pregnancy. Uncomplicated cases have been reported throughout all trimesters of pregnancy (10, 11). However, there are also a few case reports of early miscarriages in patients who received anti-VEGF injections during early pregnancy (11, 12). Physicians hypothesize that although anti-VEGF formulations, such as bevacizumab and ranibizumab, do not likely cross the placental barrier in large quantities, they may act on placental circulation by inhibiting VEGF-A. More studies are needed to reach a definitive conclusion on the safety of intravitreal anti-VEGF injections during pregnancy (10). If an anti-VEGF injection is recommended, the patient must be well-educated about the potential risks and the pregnancy must be closely monitored.
Surgical intervention may be indicated in some complicated cases, including tractional retinal detachment, non-clearing vitreous hemorrhage, and neovascular glaucoma (9). In these cases, collaboration between the ophthalmologist and the obstetrician is necessary.
Risk Factors
|
Signs
|
Symptoms
|
Treatment
|
Treloar M, Roybal CN, Niles PI, Russell, SR. Progression of Proliferative Diabetic Retinopathy During Pregnancy. EyeRounds.org. Posted September 1, 2015; Available from: https://eyerounds.org/cases/219-Gestational-Diabetic-Retinopathy.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links