
posted September 26, 2016
Download pdf"Bump in the middle corner of the left eye"
A 51-year-old male noticed a "raised bump" on the nasal portion of his eye a month prior to presentation. He associated the lesion with the onset of a red eye and episodic foreign body sensation. Additionally, he noticed that his left eyelid had been slightly "more droopy" over the past two months. He denied pain and had not experienced any photophobia, diplopia or decreased visual acuity.
External
| OD | OS (Figure 1a-b) |
| MRD1: 4mm | MRD1: 2mm |
| MRD2: 6mm | MRD2: 6mm |
| Levator Function: 14mm | Levator Function: 14mm |
| Exophthalmometry (base 94): 11mm | Exophthalmometry (base 94): 10mm |

Figure 1a: External photo showing left lid ptosis and left caruncular lesion.

Figure 1b: External photo of left eye showing raised, pink caruncular lesion
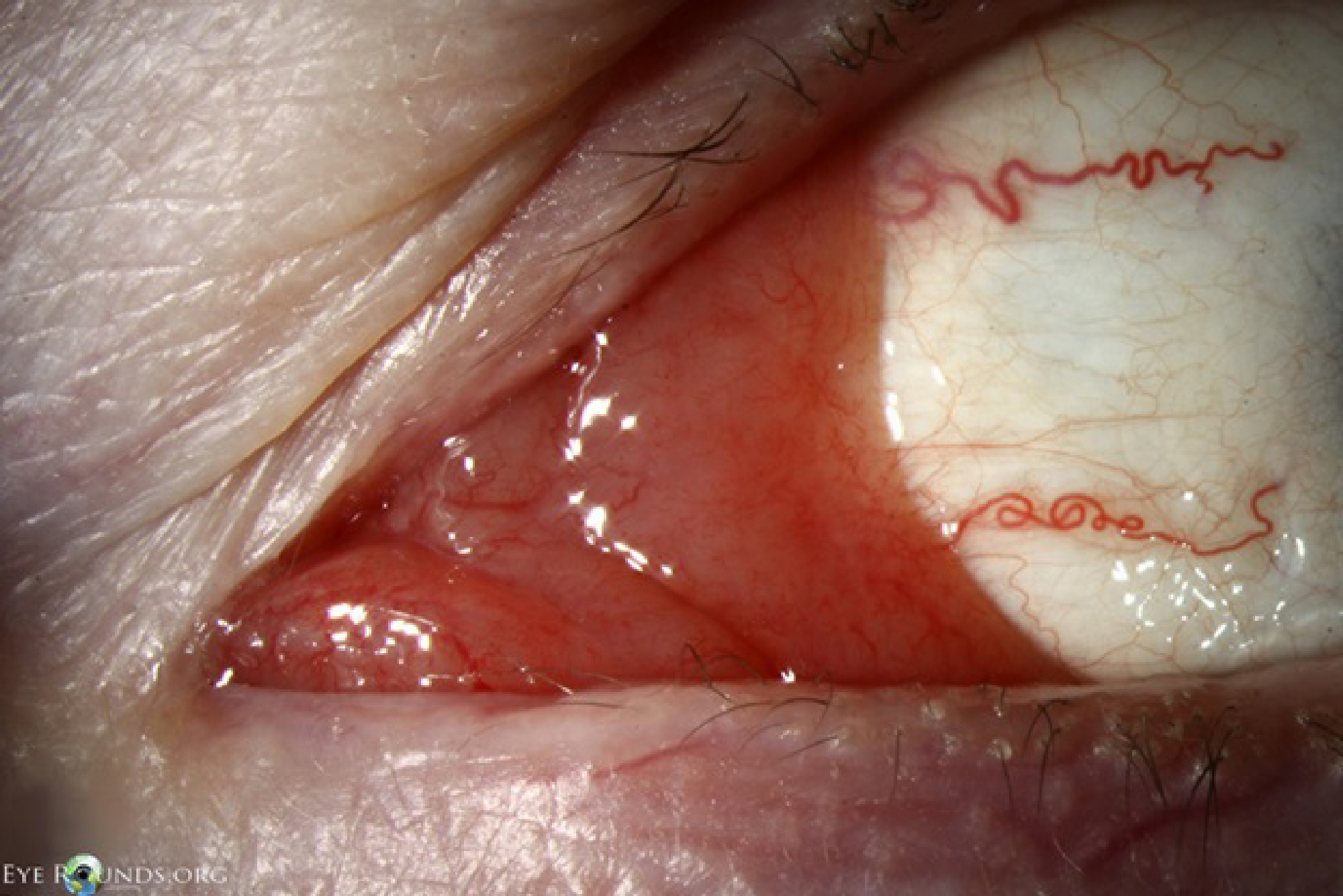
Figure 2: Slit lamp photo showing salmon colored patch with telangiectatic vessels in caruncle of left eye.
Left eye caruncular lesion was biopsied the same day in clinic. Specimens sent for anatomic pathology and immunohistochemistry for flow cytometry evaluation.
Extranodal marginal zone B-cell lymphoma of the conjunctiva
After diagnosis of extranodal marginal zone B cell conjunctival lymphoma, the patient was referred to an oncologist for evaluation of systemic involvement, including basic hematologic screening tests; magnetic resonance imaging (MRI) of the orbits; and computerized tomography (CT) of the chest, abdomen and pelvis. After it was confirmed that there was no systemic disease involvement, the patient was treated with external beam radiation therapy (EBRT) (total dose of 24 Gy in 15 fractions) to the left eye without complication. Three months post-treatment, follow up laboratory evaluation and orbital CT demonstrated no recurrence. A new lesion was noted in the inferior fornix of the right eye at his 6 month post-treatment follow up appointment. The patient was asymptomatic and unaware of the growth of the forniceal lesion. Biopsy revealed a right conjunctival marginal zone B-cell lymphoma and imaging demonstrated localized disease. He received similar local radiation therapy (24Gy in 15 fractions) to the right eye and was disease free four months following completion of radiation to the right eye (Figure 3).

Figure 3: External photos showing resolution of ptosis four months following radiation treatment to the right eye lesion and eleven months after completing radiation to the left eye lesion.
Approximately 2-8% of extranodal lymphomas occur within the adnexa of the eye [1]. Of these, approximately 25% occur within the conjunctiva [2]. Estimated incidence of conjunctival lymphoma is 2-4/1,000,000 [1]. Conjunctival lymphoma is most commonly a primary neoplasm, although 10 to 30 percent are secondary tumors in patients with disseminated lymphoma [3]. The most classic location for conjunctival lymphoma is the inferior fornix, although involvement in the superior fornix or elsewhere is not uncommon (Figure 4).

Figure 4: Slit lamp photo showing the salmon-pink appearance classically associated with conjunctival lymphoma.
Four pathological subtypes constitute the large majority of reported cases of conjunctival lymphoma, all of which are classified as non-Hodgkin's B-cell lymphomas [1]. Extranodal marginal zone lymphoma (68-81% of reported cases) is the most common subtype, followed by follicular lymphoma (8-16%). Both are histologically considered low-grade malignancies. Less common subtypes include mantle cell lymphoma (3-7%) and diffuse large B-cell lymphoma (3-4%) which are considered high-grade malignancies [1-2]. Conjunctival lymphoma is most common in the 5th to 7th decades, with a slight female predominance [1,3]. It is the third most common malignancy involving the conjunctiva, behind squamous cell carcinoma and melanoma [4].
Conjunctival lymphoma can appear clinically identical to reactive lymphoid hyperplasia. Both conditions are examples of lymphoproliferative neoplasms and must be carefully distinguished. Reactive lymphoid hyperplasia results from antigen stimulation of the conjunctival lymphoid system and is more common in younger patients. Lymphoma also arises from the conjunctival lymphoid system, although the link with chronic antigen stimulation is controversial in the literature [3,5-9] Risk factors for lymphoma development include chronic exposure to bioactive solvents and reagents, chronic autoimmune conditions, and increasing age [10].
The most common symptoms include foreign body sensation, ptosis and epiphora. The most common sign is a painless enlarging mass, which classically takes on a salmon-pink, flesh-colored appearance when deep to the conjunctiva [1]. The average delay between clinical onset and diagnosis is 6-8 months secondary to lack of significant symptoms [1,3]. Constitutional B-symptoms, including fever, night sweats, malaise and unintended weight loss are all rare in the low-grade subtypes (4-8%) [1].
Diagnosing conjunctival lymphoma after biopsy is complex as it depends on morphologic and cytometric analysis. Clinically, two samples are needed, one fixed for morphologic examination and one fresh specimen for flow cytometry. Histological heterogeneity can create diagnostic and prognostic challenges and thus flow cytometry has become critical for diagnosis. This technique gives not just clarity differentiating lymphoma from reactive lymphoid hyperplasia, but it can also define the specific subtype of lymphoma. For example, marginal zone B-cell lymphomas are positive for CD20, BCL2, PAX5, and CD79A but typically do not express CD5, CD10 or CD23 [4].
After the diagnosis of conjunctival lymphoma is made, systemic involvement of the lymphoma must be ruled-out [9]. This is particularly important because patients can have asymptomatic regional lymph node involvement and/or systemic involvement at the time of diagnosis [9]. Evaluation for systemic involvement includes orbital CT and/or MRI, basic hematologic screening tests (complete blood count, white blood cell differential, serum immunoprotein electrophoresis), CT chest/abdomen/ pelvis, and bone marrow biopsy. The most common stage at initial diagnosis was stage IE using Ann Arbor staging and stage T1 using the AJCC TNM staging system (Table 1a-b). Both of these stages indicate only local involvement.
Table 1a. TNM-based orbital lymphoma staging system [11].
| (A) TNM-based AJCC staging system* for ocular adnexal lymphomas | |
| Primary tumor (T) | |
| TX | Lymphoma extent not specified |
| T0 | No evidence of lymphoma |
| T1 | Lymphoma involving the conjunctiva alone without orbital involvement |
|
Bulbar conjunctiva only |
T1b |
Palpebral conjunctiva ± fornix ± caruncle |
|
Bulbar and nonbulbar conjunctival involvement |
| T2 | Lymphoma with orbital involvement ± any conjunctival involvement |
|
Anterior orbital involvement but no Iscrimal grand involvement (± conjunctival disease) |
|
Anterior orbital involvement with lacrima gland involvement (± conjunctival disease) |
|
Posterior orbital involvement (± conjunctival involvement ± any extraocular muscle involvement) |
|
Nasolacrimal drainage system involvement (± conjunctival involvement but not including nasopharynx) |
| T3 | Lymphoma with preseptal eyelid involvement ± orbital involvement ± |
| T4 | Orbital adnexal lymphoma extending beyond orbit to adjacent structures, such as bone and brain |
|
Involvement of nasopharynx |
|
Osseous involvement (including periosteum) |
|
Involvement of maxillofacial, ethmoidal, ± frontal sinuses |
|
Intracranial spread |
| Lymph node involvement (N) | |
| NX | Involvement of lymph nodes not assessed |
| N0 | No evidence of lymph node involvement |
| N1 | Involvement of ipsilateral regional lymph nodes |
| N2 | Involvement of contralateral or bilateral regional lymph nodes |
| N3 | Involvement of peripheral lymph nodes not draining ocular adnexal region |
| N4 | Involvement of central lymph nodes |
| Distal metastasis (M) | |
| MX | Dissemination of lymphoma not assessed |
| M0 | No evidence of involvement of other extranodal sites |
| M1 | Lymphomatous involvement in other organs recorded either at first diagnosis or subsequently |
|
Noncontiguous involvement of tissues or organ external to the ocular adnexa (e.g. parotid gland, submandibular gland, lung, liver, spleen, kidney, breast) |
|
Lymphomatous involvement of the bone marrow |
|
Both M1 and M1b involvement |
Table 1b. Ann Arbor staging classification specific to lymphoma [11].
| (B) Ann Arbor staging classification for Hodgkin and non-Hodgkin lymphomas | |
| Stage I | Involvement of a single lymph node region or extralymphatic region/organ (IE) |
| Stage II | Involvement of 2 or more lymph node regions or lymphatic structures on teh same side of the diaphragm alone or extralymphatic regions on the same side of the diaphragm (IIE) |
| Stage III | Involvement of lymph node regions on both sides of the diaphragm with localized extralymphatic (IIIE) or splenic (IIIS) involvement or both (IIIES) |
| Stage IV | Involvement of one or more organs or tissues outside the lymphatic system, with or without involvement of nearby lymph nodes |
A: Without B symptoms |
|
Localized disease is most commonly treated with external beam radiation therapy (ERBT) with or without chemotherapy [1,10]. ERBT dose normally ranges between 15-45 Gy [1]. The complete remission rate of localized lymphoma is over 90 percent [3-4]. Radiation therapy can also prevent systemic spread in some cases if the lesion is isolated [10]. Other options include excision only, excision and topical chemotherapy, and intralesional chemotherapy [9]. Agents used include interferon alfa-2b and rituximab [3]. For disseminated disease, a single agent or combination chemotherapy is commonly used [3].
Disease recurrence has been shown to be significant, as one recent study showed 38% of patients with extranodal marginal zone conjunctival lymphoma had recurrence with a median recurrence of 24 months [1]. It is therefore recommended to continue surveillance indefinitely with follow up every 3 months for the first year, followed by every six months to a year thereafter [3].
Tumor histology is the most significant prognostic factor, as survival is much longer for low grade malignancies like marginal zone and follicular lymphoma compared to high grade malignancies like mantle cell lymphoma [1]. The location of lymphoma within the orbit also carries prognostic value, as conjunctival lymphoma carries the lowest risk of systemic lymphoma while lymphoma of the eyelids carries the highest risk [10]. Bilateral involvement has a significant impact on survival, with one study finding the 10-year progression free survival to be 72% for those with unilateral disease compared to 48% in bilateral disease [12].
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
Greenwald MF, Meirick TM, McConnell LK, Shriver EM. Conjunctival Lymphoma. EyeRounds.org. September 26, 2016; Available from: https://eyerounds.org/cases/243-conjunctival-lymphoma.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
