INITIAL PRESENTATION
Chief Complaint “Right droopy eyelid”
History of Present Illness
A 74-year-old male with history of metastatic prostate cancer presented with 5 days of progressive difficulty opening his right eye. The patient was noted to have ptosis of the right upper lid by his radiation oncologist while at an appointment for palliative radiation to metastatic prostate cancer in his right hip. A computed tomography (CT) of the head demonstrated possible metastatic disease in the right superior orbital fissure. Over the following days, the patient became unable to move his right eye or open his right eyelid. His vision remained intact when the eyelid was manually lifted. Neuro-ophthalmology was consulted for further evaluation upon admission.
Past Ocular History
Past Medical History
Medications
Allergies
Family History
Social History
Review of Systems
OCULAR EXAMINATION
| OD | OS | |
|---|---|---|
| Lids/lashes | Complete paralytic ptosis of right upper lid | Normal |
| Conjunctiva/sclera | Temporal chemosis | Clear and quite |
| Cornea | Clear | Clear |
| Anterior Chamber | Deep and quiet | Deep and quiet |
| Iris | Normal architecture | Normal architecture |
| Lens | 2+ nuclear sclerosis | 2+ nuclear sclerosis |
CLINICAL COURSE
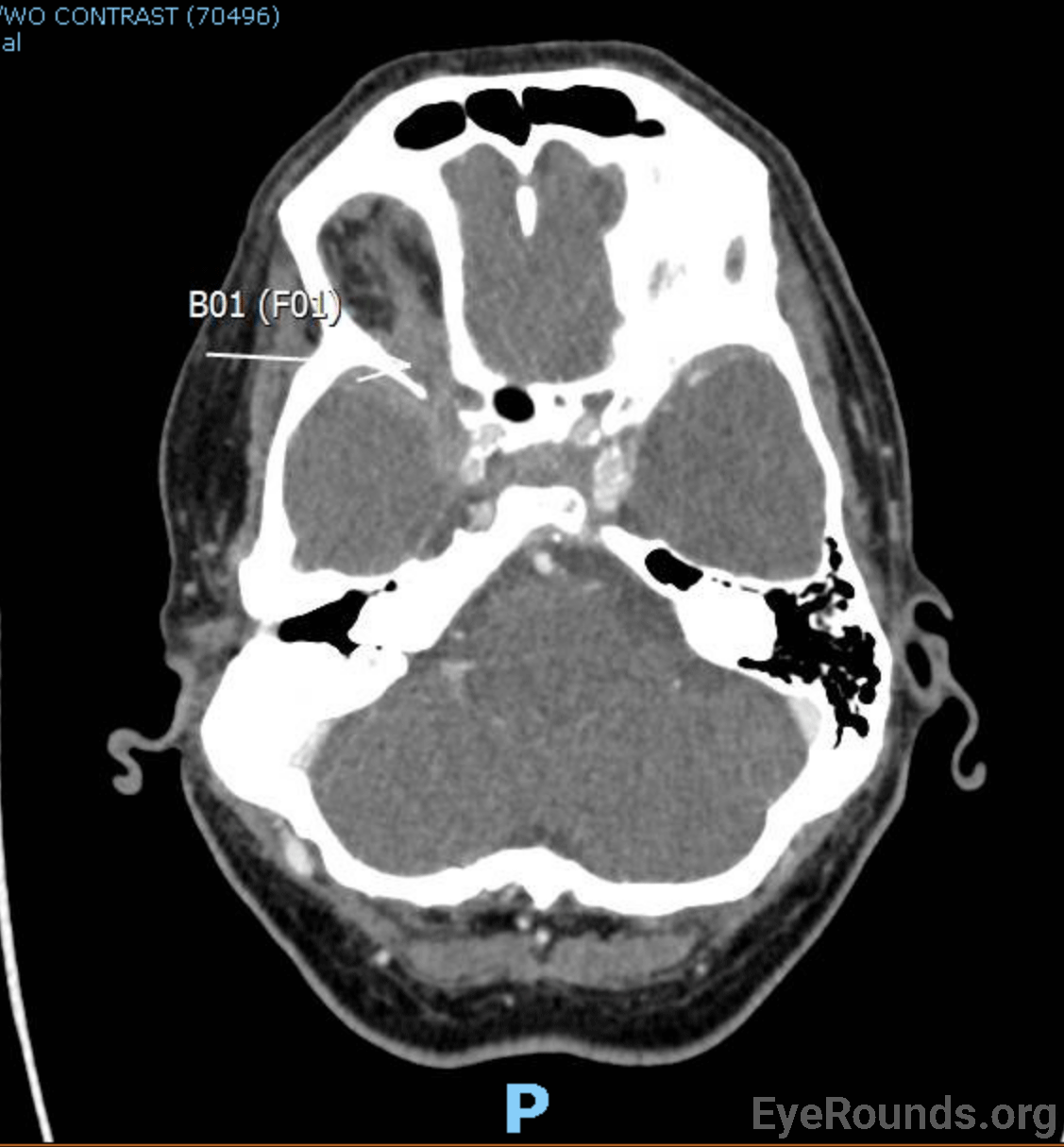
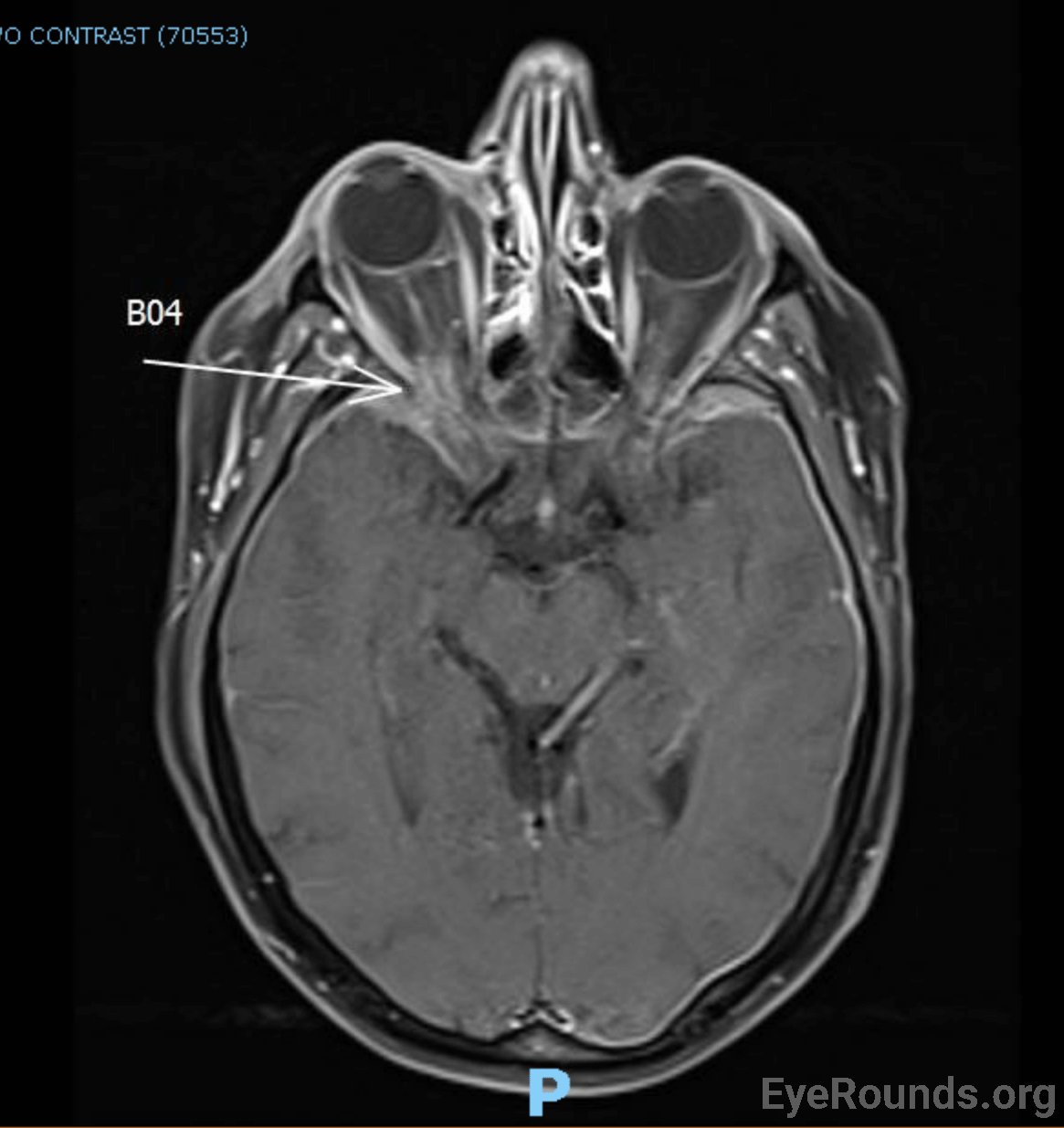
CT scan on admission (Figure 1[A]) showed concern for a possible metastatic lesion involving the right superior orbital fissure. Due to concerns of a prior ear prosthesis placed following a stapedectomy over three decades ago with unknown MRI compatibility, MRI was delayed, and the patient was started on empiric dexamethasone of 4 mg twice daily. MRI was eventually performed which revealed a metastatic lesion involving the superior orbital fissure, thus confirming the diagnosis of superior orbital fissure syndrome on the right. There were also concerns for right cavernous sinus thrombosis, which was subsequently confirmed on MRV. The patient was not a surgical candidate and was treated with radiation therapy to the superior orbital fissure lesion. He was started on Apixaban 5 mg twice daily for treatment of the cavernous sinus thrombosis. The patient was noted to be hyponatremic during hospitalization and workup was consistent with syndrome of inappropriate antidiuretic hormone section (SIADH) which was responsive to fluid restriction. Dexamethasone was decreased to 2 mg twice daily at time of discharge, and he was noted to have minimal improvement in his ophthalmoplegia and ptosis 1 month after discharge.
DIAGNOSIS: Superior orbital fissure syndrome of the right eye secondary to metastatic prostate cancer
DIFFERENTIAL DIAGNOSIS:
DISCUSSION
Etiology/Epidemiology
Superior orbital fissure syndrome (SOFS), also known as Rochon-Duvigneaud Syndrome, is a type of orbital apex disorder. SOFS is a rare syndrome whose manifestations are based on compression of structures within the superior orbital fissure. As such, most of the information known about SOFS comes from sporadic case reports. While trauma is the most common underlying cause for SOFS, the entity as a whole is uncommon. A large retrospective study by Chen et al. revealed that 0.3% of patients with skull or facial fractures secondary to trauma develop this condition (1). Other studies have demonstrated similar incidences of approximately 0.8% following traumatic facial injury (2).
While trauma is the leading reported cause of SOFS, any condition that compromises the structures within the superior orbital fissure can precipitate it. Neoplasms, such as metastatic lesions, can cause a compressive mass effect within the superior orbital fissure (3). In women, breast cancer is the most common cause of metastatic orbital involvement which can precipitate SOFS (4). Infections such as meningitis, syphilis, and herpes zoster can also lead to inflammation and compression of key structures within the fissure (5-8). Vascular processes, such as aneurysms and pseudoaneurysms, have also been identified causes (9). Due to the often unpredictable nature of these aforementioned etiologies, the only reliable risk factor for the development of SOFS is an anatomically narrow superior orbital fissure (10). If the optic nerve is involved in patients with suspected superior orbital fissure syndrome, the diagnosis changes and becomes known as orbital apex syndrome (11).
Anatomy
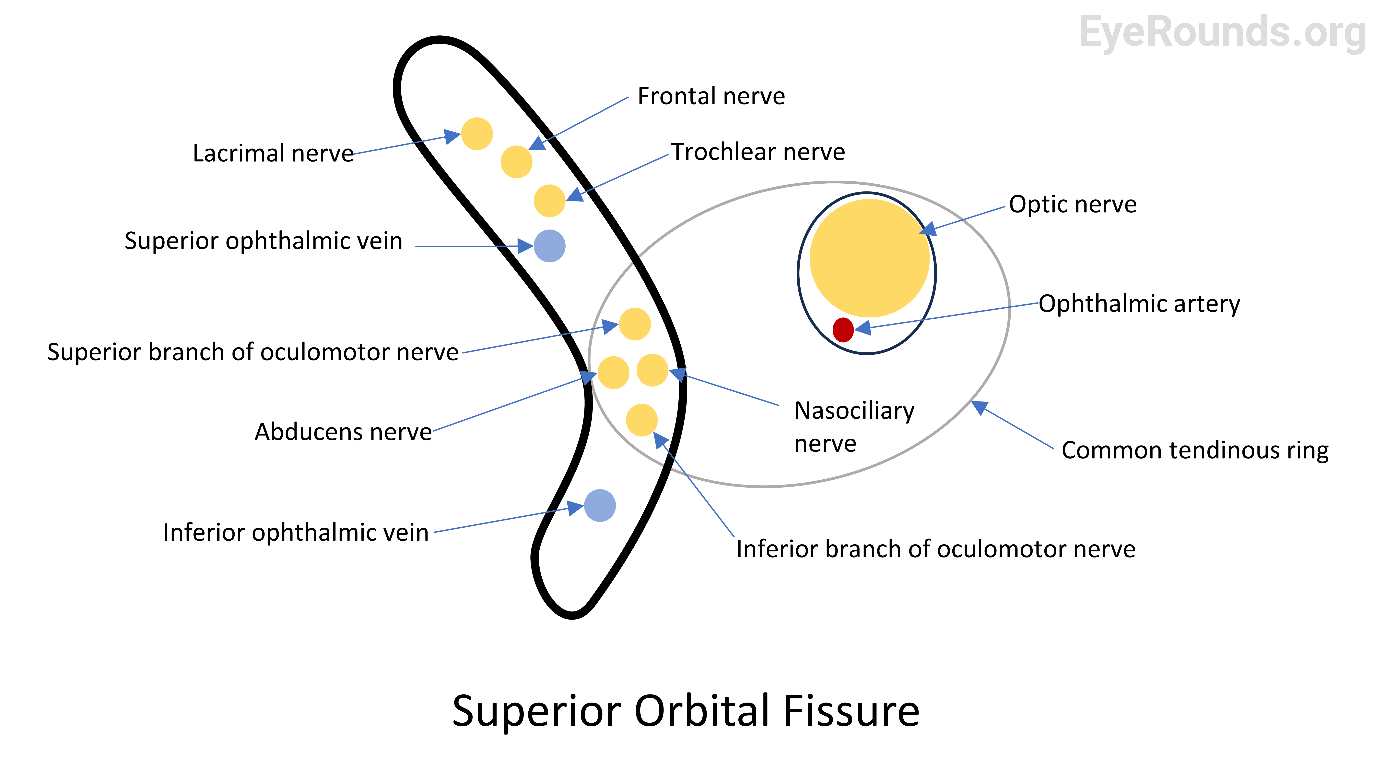
The superior orbital fissure lies between the greater and lesser wings of the sphenoid bone. Multiple structures run through this area, and they can be categorized into three distinct regions based on their location relative to the common tendinous ring (also known as the annulus of Zinn) (Figure 2). The superolateral region outside the annulus of Zinn contains the trochlear, frontal, and lacrimal nerves (a branch of CN V1) along with the superior ophthalmic vein (12). The central region within the annulus of Zinn transmits the superior and inferior divisions of the oculomotor nerve, the nasociliary nerve (another branch of CN V1), and the abducens nerve (12). Inferiorly, outside the annulus of Zinn, one finds the inferior ophthalmic vein (12). Disruption of these structures, whether through shear injury, compression, inflammation, infection, infiltration, or ischemia, results in the signs and symptoms of SOFS. Medial to the superior orbital fissure and within the annulus of Zinn lies the optic canal. Within the optic canal, both the optic nerve and the ophthalmic artery traverse into the orbit (11).
Signs/Symptoms
The clinical presentation for patients with SOFS can be directly correlated to the structures that are compromised. Patients may demonstrate upper lid ptosis if the superior division of CN III is impacted, causing partial to complete paralysis of the levator palpebrae superioris muscle. Partial or complete ophthalmoplegia is also a common finding and can develop with damage to CN III, IV, and/or VI. Similarly, proptosis may occur due to decreased extraocular muscle tone or mass effect. Anhidrosis can develop if sympathetic innervation to the eye is damaged as it runs along CN V1. Anesthesia of the superior eyelid and lower forehead with loss of the corneal reflex leading to a neurotrophic cornea may also occur through the same process. Finally, the pupil may appear dilated without the ability to constrict to light due to loss of parasympathetic input to the eye. (10)
Work-up
When clinical suspicion of SOFS is high, imaging can be used to confirm possible lesion localization and aid in diagnosis. The imaging modality of choice is based on the likely underlying cause of SOFS and hospital availability, with CT being more readily available than MRI. In cases of trauma, CT is the imaging test of choice (13). The most common findings on CT for trauma patients include fractures to the zygomatic and orbital bones (1). CT is also beneficial for measuring the size of the superior orbital fissure. For other causes of SOFS, such as neoplastic, infectious, and inflammatory, MRI with and without contrast with fat suppressed images of the orbits is the modality of choice due to its superior visualization of soft tissue and nerve structures (13). For cases where MRI is used, imaging findings will vary based on the underlying etiology. Neoplastic lesions may reveal underlying metastasis or meningiomas, and infectious processes may show orbital cellulitis or subperiosteal abscesses (13). In cases of suspected vascular abnormalities, both MR angiography and CT angiography are appropriate and would likely identify the underlying process (13). If an infectious cause is suspected, laboratory evaluation with complete blood counts with differentials, basic metabolic panels, and blood cultures are standard. More targeted evaluation, such as a lumbar puncture for meningitis, will depend on the clinical presentation of the patient and the suspected infection. The superior orbital fissure is challenging to access surgically, so biopsy of adjacent tissues in the sinus, orbit, retromaxillary space, inferior orbital nerve, or remote areas such as primary or other metastatic tumors or lymph nodes are options.
Treatment/Management/Guidelines
Trauma is the most well-studied cause of superior orbital fissure syndrome. One study in 2010 reviewed 29 cases and found that patients treated with steroids recovered in 70% of cases compared to 42.1% in those treated with conservative measures alone (10). In both instances, the majority of patients also received surgery (84.7%), most commonly decompression through fracture fixation or hematoma evacuation, without significant aggravation of neurological symptoms post-repair (10). Due to this, the proposed treatment of traumatic SOFS is combination megadose steroids (e.g., 30 mg/kg methylprednisolone followed by 5.4 mg/kg per hour for 48 hours) and surgical intervention (10). More recent literature also supports this approach (14,15).
While steroids have been linked to improved outcomes in patients presenting with traumatic SOFS, this must be balanced against the risks of steroids in patients with traumatic brain injury (TBI). The CRASH study showed that the use of megadose steroids in patients presenting with TBI and Glasgow coma scale (GCS) >15 is associated with an increased risk of death and disability (16). While early studies have shown a benefit with steroids in traumatic SOFS, due to the concern for an increase in mortality, the use of steroids in patients with severe trauma is controversial and typically not employed.
Treatments for other types of SOFS are less well-studied. Depending on the cause, neoplastic cases may be treated with chemotherapy, radiation, or debulking surgery (4,17,18). Steroid therapy may also benefit these patients if significant edema is visualized on imaging surrounding these lesions. In cases of infection, treatment with appropriate antibacterial, antivirals, or antifungals, occasionally coupled with steroids, is typically used along with adjacent sinus debridement and washout (5,19,20). Vascular causes, such as pseudoaneurysms, are usually managed through an endovascular approach (21). In summary, the treatment of SOFS is targeted at the underlying cause (surgery, antimicrobials, radiation/chemotherapy) and is commonly combined with high-dose steroids to decrease any coexisting inflammation. Due to the rarity of these etiologies, there is limited data on the return of neurologic function. Patient follow-up is highly variable and depends on the underlying cause and treatment undertaken.
EPIDEMIOLOGY OR ETIOLOGY
|
WORK-UP
|
SIGNS AND SYMPTOMS
|
TREATMENT/MANAGEMENT
|
Related Link(s):
References
Heinzman Z, Ahmed B, and Linton E. Superior Orbital Fissure Syndrome. EyeRounds.org. Jan. 26, 2024. Available from https://eyerounds.org/cases/355-Superior-Orbital-Fissure-Syndrome.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links