Chief Complaint: 89-year-old female with a history of gradual redness and proptosis OD over 3 weeks.
History of Present Illness: Redness and proptosis OD worsened on 10 days of IV vancomycin & ceftriaxone.
PMH/FH/POH: mitral valve regurgitation, advanced Alzheimer's disease, heart disease, glaucoma, schizophrenia, diabetes, and myopia.
Patient has had trabeculectomies OD and OS.
| OD | OD |
|
|
| Face photo denoting marked proptosis OD with purulent discharge and periorbital erythema. | Photograph of right eye: fibrin in anterior chamber with consolidated hypopyon, marked conjunctival injection and chemosis, and purulent discharge. |
|
|
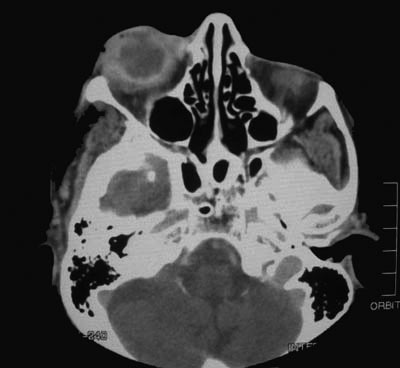
| CT scan: marked proptosis OD with thickened sclera OD | A different view demonstrating thickened sclera OD wth adjacent areas of possible abscess and/or inflammation. |
|
|
| Area of globe perforation from pan-endophthalmitis. | The optic nerve separated from the globe during enucleation. There is a rim of necrotic tissue at the lamina cribrosa. |
Pan-endophthalmitis and Orbital Cellulitis
This patient presented with periorbital swelling, erythema, proptosis, loss of vision, and ophthalmoplegia of the right eye. She developed an endophthalmitis, likely due to trabeculectomy blebitis, which evolved into a pan-endophthalmitis because of her declined mental function and delay to seek medical attention. The pan-endophthalmitis resulted in globe perforation and spread of the infection resulting in an orbital cellulitis. On CT scan, there was marked scleral thickening and inflammation around the globe. The original scans were worrisome for a possible orbital abscess, which requires emergent surgical exploration and intervention. During surgery, we encountered purulent discharge and inspection of the globe revealed an area of perforation due to necrosis and infection. At this point, the decision was made to perform an enucleation of the right eye.
The presence of a trabeculectomy bleb increases the incidence of infection and endophthalmitis. It is estimated that the incidence of endophthalmitis following trabeculectomy surgery occurs at a rate of less than 1:1000 for early and 1:500 for late endophthalmitis, but can be as high as 1:100 cases. Risk factors for infection following trabeculectomy surgery include: an inferior or nasally located bleb; presence of a high bleb or blepharitis; development of a late-onset bleb leak; use of antifibrotic agents; chronic antibiotic use; and performance of a trabeculectomy alone versus a combined procedure. The use of antifibrotic agents, e.g. mitomycin-C and 5-fluorouracil, have been implicated in increasing the incidence of post-trabeculectomy endophthalmitis due to thin, cystic blebs; however, some studies have not observed a statistically significant increase in the rates of infections with antifibrotic agents during trabeculectomy surgery.
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
|
Doan A, Carter KD: Pan-endophthalmitis and Orbital Cellulitis: 89-year-old female with a history of gradual redness and proptosis OD over 3 weeks. February 21, 2005; Available from: http://www.EyeRounds.org/cases/case16.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links