
Chief Complaint: 5-year-old white female presenting with dog bite to left side of face.
History of Present Illness: 5 hours prior to this evaluation, patient was playing with the black Labrador retriever of a family friend. Family witnessed the dog making a single lunge at the girl’s face, and an incomplete bite resulted with only the top jaw making contact. The dog did not attack further, and the incomplete bite to the left face was the only injury sustained.
POH/PMH/SH: No past ocular history. No past medical history. No past surgical history. No medications nor allergies. Well-adjusted kindergarten child lives at home with parents. Childhood immunizations up to date.
The patient was taken to the operating suite for examination under anesthesia (EUA) and laceration repair, likely to include canalicular repair (see Photos).
Continuation of the examination in the operating suite revealed that the remainder of the anterior segment examination and DFE were normal.
At this point, it is worthwhile to discuss both when to suspect canalicular laceration or avulsion and how to evaluate the wound. In any case where injury extends close to the lid margin medial to the puncta of the eyelids it is reasonable to assume that the canaliculus has been injured (Nerad, The Requisites, Oculoplastic Surgery 2001). The canaliculus is relatively superficial and can be readily injured even with cuts only a few millimeters deep. Dog bites commonly result in avulsion of the canalicular system because these are the weakest areas of the lids.
Evaluation should first be attempted directly within the laceration or avulsion injury to search for the proximal and distal cut ends of the canaliculus itself, which can be recognized as a gray or pink ring within the reddish orbicularis oculi muscle. Canalicular probing from the punctum toward the laceration may reveal the exposed probe within the wound as it exits the canaliculus. If the proximal end of the damaged canaliculus is not found on direct examination nor discovered by following the path of the probe used to explore the torn distal end, a pigtail probe may be used to intubate the intact side of the lacrimal system. The probe will pass through the intact canaliculus, curve through the common canaliculus, and enter the distal end of the torn canaliculus to exit within the wound.
In a small percentage of patients, there is no common canaliculus and both the upper and lower canaliculus enter the lacrimal sac independently. In these patients, the surgeon will be unable to use the pigtail probe technique, and a Crawford stenting procedure will be required.
If at any time the patient is unable to tolerate this examination but suspicion for canalicular involvement remains high, further exploration should be postponed. In these cases, the patient will require exam under anesthesia (EUA) anyway and further examination may then be done in the operating suite during the time of laceration and possible canalicular repair.
Such was the case with the young patient presented in this case. The following pictures were taken after EUA and during surgical repair to document the stepwise repair of a single canalicular laceration using the pigtail probe technique. Repair with Crawford stents is also a common technique and is done as the primary approach by many surgeons. The steps for Crawford stent repair and the less common Jone’s tube repair may be found in most oculoplastic surgery texts.
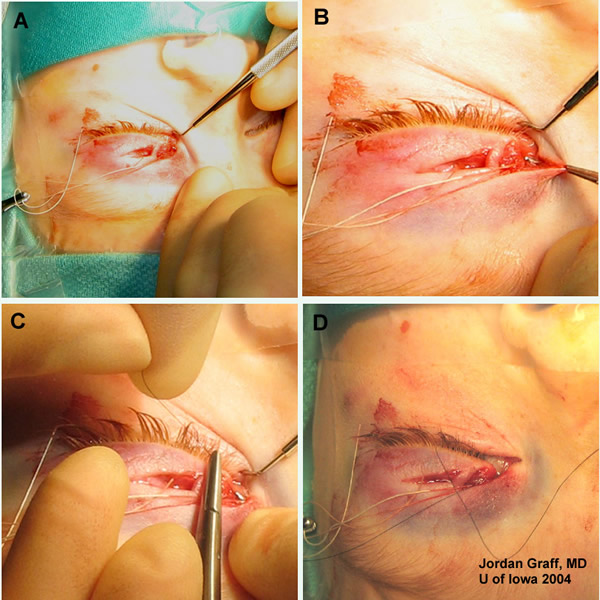 |
Note that in this particular patient, the laceration lies in the distal half of the canaliculus, closer to the punctum. The two direct lacerations lie across the upper lid. It is worthwhile to point out that this is a less common type of canalicular damage with most dog bites. More commonly, dog bites result in an avulsion injury which tears the canaliculus at or near the lacrimal sac. This is often in the lower lid. When a dog bites the face, the animal will often fix its lower teeth under the mandible of the patient, with the upper teeth grasping on the upper face, including around the lower eyelid. The closing of the jaw results in a tearing force on the tissues of the lower lid and midface. An avulsion injury often results in addition to whatever puncture or laceration wounds may have been caused by the teeth themselves.
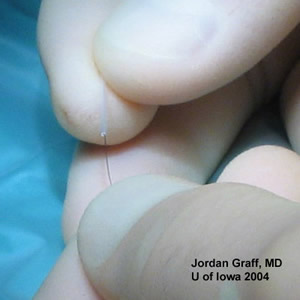 |
2A) A 25 mm segment of silicone tubing is passed over the nylon suture. |
 |
2B) Grasping the silicone stent with smooth forceps, the suture and overlying silicone stent are then carefully drawn through the canaliculus. |
 |
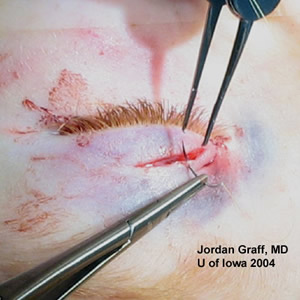
2C) Nylon suture guided the stenting of the avulsed canaliculus. |
This repair took place within 10 hours of the time of injury. It is a general consensus among the major texts that repair be done at least within the first 24 hours. Prompt repair will minimize the degree of scarring and fibrosis which could make canalicular intubation difficult.
 |
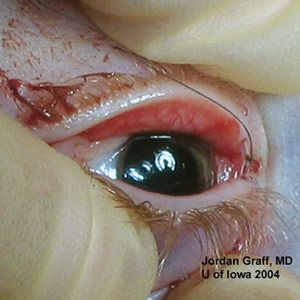
3A) The pigtail probe is passed into the punctum of the injured side. The probe exits through the lacerated canaliculus within the wound. |
 |
3B) The distal end of the same 6-0 Nylon is now threaded through the eye of the pigtail probe and the probe is withdrawn. The silicone stent is further advanced through the superior punctum completing a circular path through both canaliculi. Deep sutures are also tied at this point. |
 |
3C) With the medial canthal tendon repaired and deep tissues approximated, the 6-0 Nylon is tied off and cut short. This allows the knot to be retracted within the silicone stent. The stent is then rotated out of the palpebral fissure and within the canalicular system. |
 |
3D) Skin edges are then approximated with 7-0 Vicryl or 5-0 fast absorbing gut sutures. |
There has been discussion in the literature regarding the need for primary canalicular repair if the opposing lid retains an intact drainage system as proven by Jones dye test. However, Linberg and Moore showed that a full 50% of healthy patients will have intermittent epiphora, increased tear film or discomfort if only one of their canaliculi is occluded. Because it is impossible to know which patients may have those symptoms if the damaged canaliculus is not repaired, primary reconstruction of all canalicular lacerations is generally recommended. Additionally, it is significantly easier to repair the drainage system during the primary surgery than to re-operate at a later date after canalicular scarring has occurred.
The surgeon should be reminded that when facial lacerations are the result of a dog bite, decisions regarding rabies vaccination require information about the animal. Regulations vary from state to state within the United States. Usually, the animal is detained in the custody of local animal control for 10 days, and its rabies vaccination status is determined. If the animal cannot be found, shows clinical signs of rabies, or tests positive for rabies, a 6-shot series of post-exposure prophylaxis is recommended. The first shot is given as soon as possible and the next 5 shots over a 28-day period (see your local Animal Control office website for additional details). Obtain contact information for the Animal Control office and a case # for the animal in question so that you may use for future reference.
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
Post-Surgical Care
|
Graff JM, Allen R. Canalicular Laceration - Dog Bite: 5-year-old white female presenting with dog bite to left side of face. EyeRounds.org. February 21, 2005; Available from: http://www.EyeRounds.org/cases/case26.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
