

Bilateral Internuclear Ophthalmoplegia and Thalamic Esotropia: The Result of Metastatic Disease
Internuclear ophthalmoplegia (INO) is due to a lesion of the medial longitudinal fasciculus (MLF) between the 3rd and 6th cranial nerve nuclei, resulting in impaired adduction of the ipsilateral eye and abducting nystagmus with contralateral gaze. Because the right and left MLF are in close proximity, bilateral INO can occur. There are numerous causes of INO, including neoplasm, but the most common cause of bilateral INO is demyelinating disease. Neoplasia, when it does manifest as INO, rarely occurs in isolation (1).
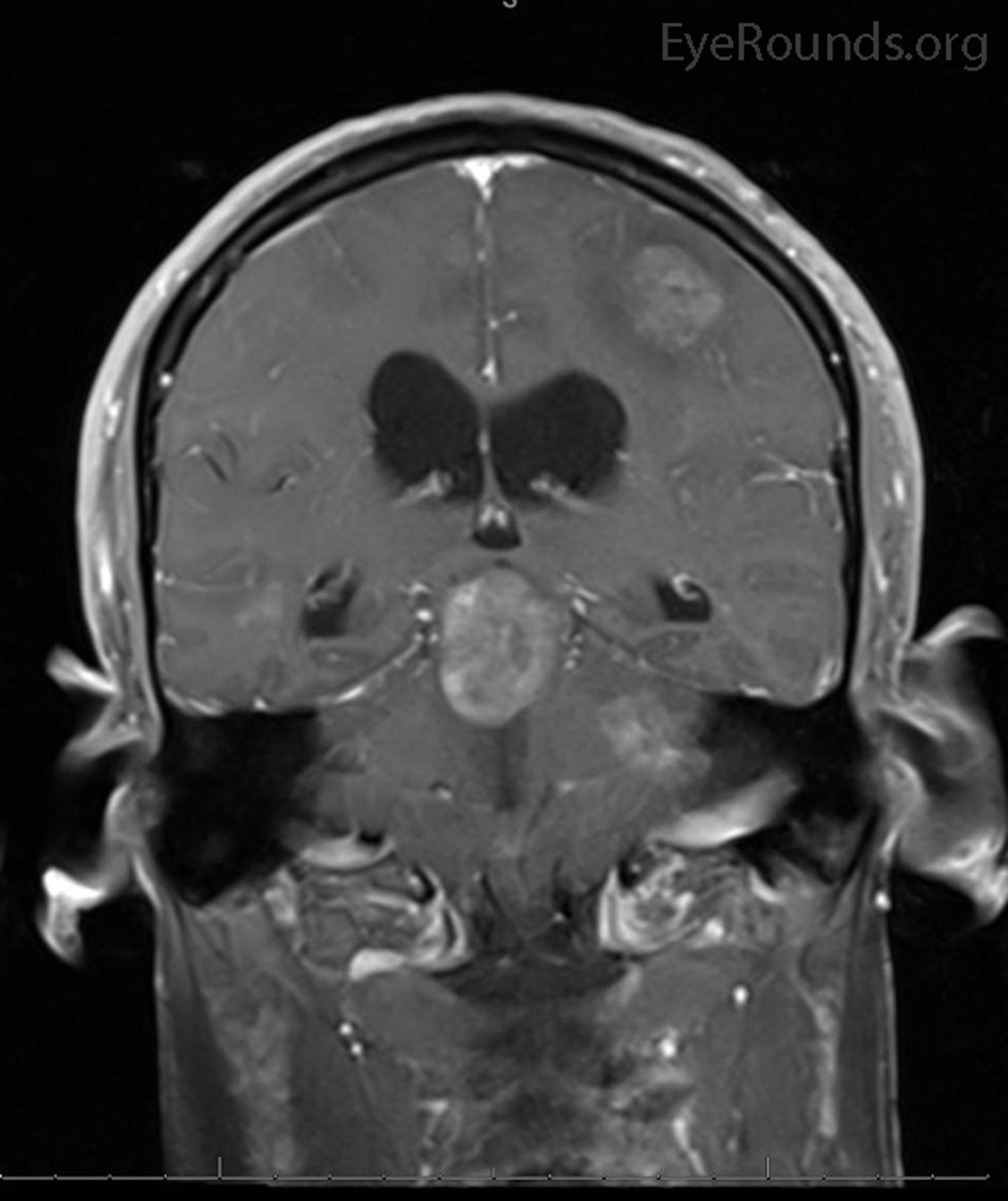
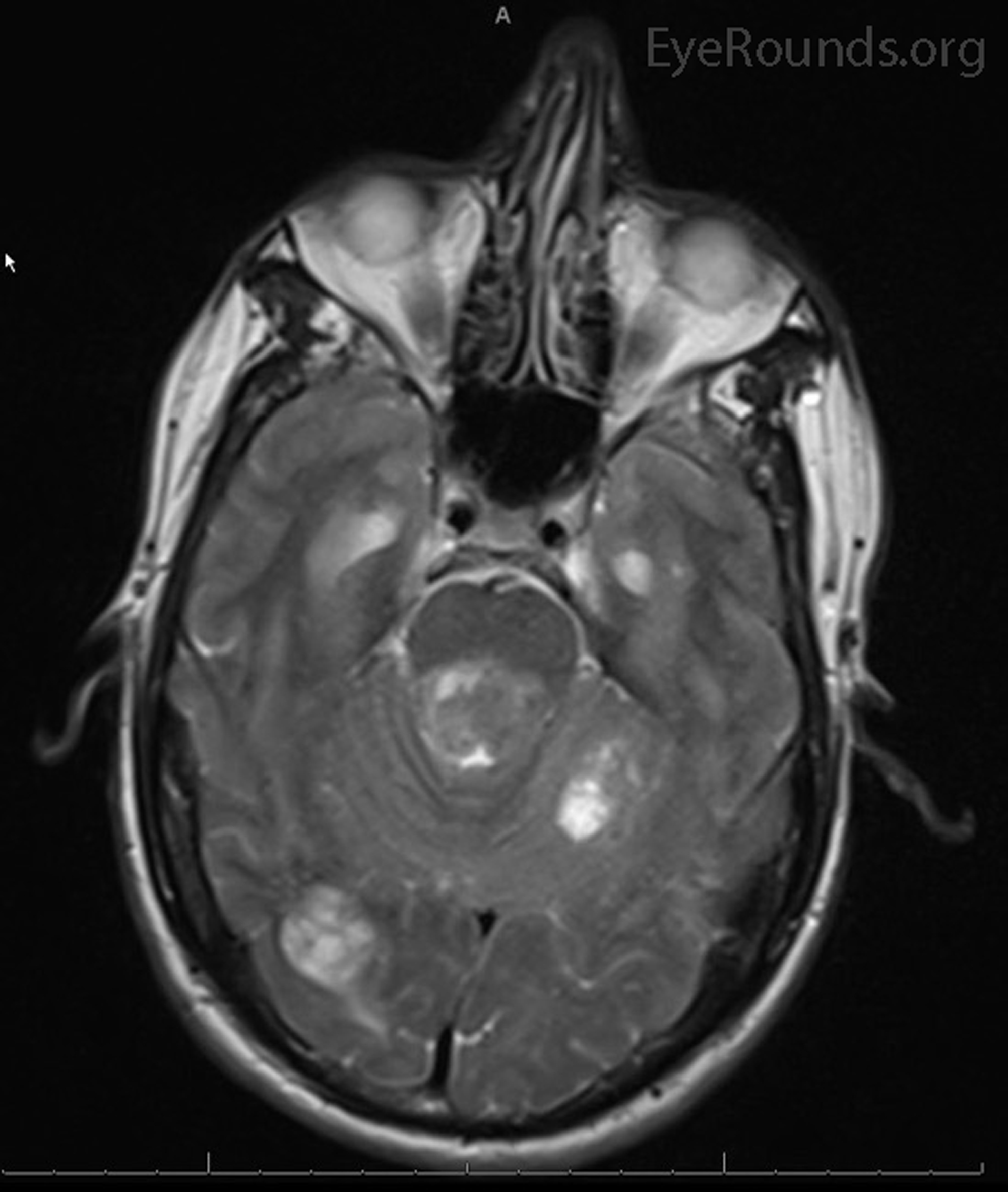
Our patient had metastatic squamous cell lung carcinoma (Figure 1) with lesions involving the brainstem and bilateral MLF, resulting in a bilateral INO. He also had metastases adjacent to the thalamus and evidence of a thalamic esotropia (noted with down gaze), a rare entity typically seen with thalamic hemorrhage (2). Though the exact cause of thalamic esotropia is unknown, disinhibition of descending convergence pathways is a proposed mechanism (3). Some patients with a thalamic esotropia also have abduction deficits, making thalamic esotropia a potential cause of pseudoabducens palsy.
 |
 |
Video: Up gaze is normal. Esotropia is present with down gaze. With right gaze, there is abducting nystagmus of the right eye and limited adduction of the left eye with a slow adducting saccade. With left gaze, there is abducting nystagmus of the left eye and limited adduction of the right eye with a slow adducting saccade.
If video fails to load, use this link: https://vimeo.com/171007997
References:
- Rismanchi N, Crawford JR. Bilateral internuclear ophthalmoplegia associated with pediatric brain tumor progression: a case series and review of the literature. J Neurooncol (2013) 115:487-91.
- Gomez CR, Gomez SM, Selhorst JB. Acute thalamic esotropia. Neurology. (1988) 38(11):1759-62.
- Han IB, Ahn JY, Kim HS. Acute esotropia secondary to thalamic hemorrhage. Kor J Cerebrovascular Surgery (2005) 7:245-48.