A 62-year-old woman with a history of glaucoma and bilateral superior trabeculectomies presented with bilateral brow ptosis and right upper eyelid ptosis (Figure 1). The patient underwent bilateral brow ptosis repair by internal browpexy and right upper eyelid ptosis repair by external levator advancement (ELA). After unilateral upper eyelid ptosis repair, the patient developed contralateral ptosis (Figure 2) [2]. The reflexive descent of the contralateral upper eyelid after the unilateral raising of the ptotic eyelid is common and explained by Hering's Law. Surgical repair leads to decreased innervation to the bilateral levator palpebrae muscles, which are equally innervated [1]. The patient subsequently underwent a left upper eyelid ptosis repair by ELA.

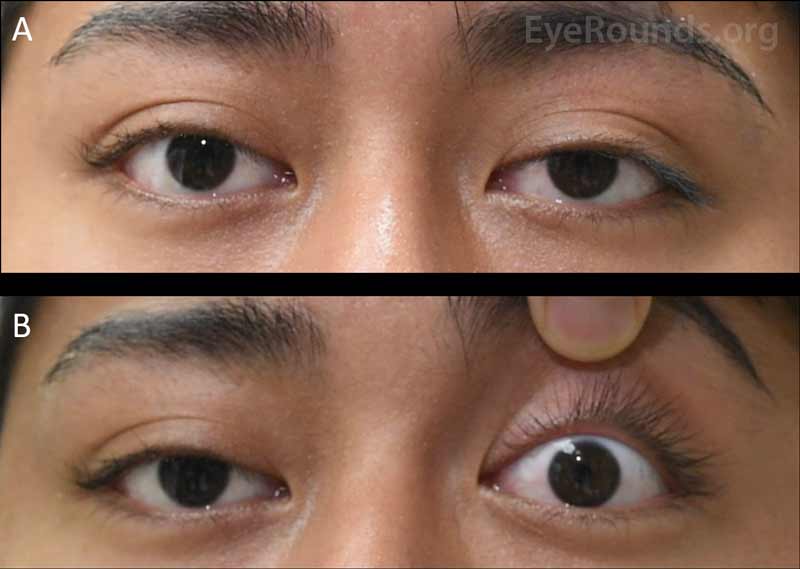
Hering's response describes the phenomenon in which manual elevation of one eyelid causes descent of the contralateral eyelid (video). This can be attributed to the yoked innervation of the levator palpebrae superioris muscles such that a singular signal controls both eyelids [1]. In the case of unilateral ptosis, while increased innervation to levator muscles compensates for decreased visual field on the affected side, the unaffected lid is simultaneously raised (panel A). When the ptotic lid is lifted – whether manually, pharmacologically, or surgically – this compensatory innervation is decreased and the unaffected lid falls (panel B). Therefore, unilateral ptosis repair may cause secondary ptosis of the contralateral eyelid and significant asymmetry; bilateral ptosis repair (either simultaneous or delayed) may be necessary for optimal results.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.


Address
University of IowaLegal
Related Links