

Neurotoxin Tarsorrhaphy
Contributors: Kelly H. Yom, BA; Dabin Choi, BS; Aaron M. Ricca, MD; Pavane L. Gorrepati, BA; Audrey C. Ko, MD
Photographer: Audrey C. Ko, MD
Posted June 19, 2018
A 69-year-old man with history of facial malignancy presented with mechanical and cicatricial left lower eyelid retraction and ectropion after surgical resection and radiation (Figure 1). Examination revealed exposure keratopathy and a non-healing corneal epithelial defect. There can be delayed wound healing and chronic fibrosis in patients who have had radiation [1]. Thus, this patient was not a good candidate for surgical or temporary suture tarsorrhaphy.
A neurotoxin tarsorrhaphy was performed since it is a safe and effective method to protect the cornea [2]. Moreover, this procedure can be done in the clinic setting and allows further examination of the eye, as it does not permanently fuse the eyelids. Following neurotoxin injection in the left upper eyelid, complete ptosis was successfully achieved (Figure 2), and the patient reported overall improvement in his symptoms. The corneal epithelial defect subsequently resolved.

Figure 1. External photograph demonstrating the left upper eyelid position, exposure keratopathy, and diffuse injection of the left eye prior to receiving neurotoxin.
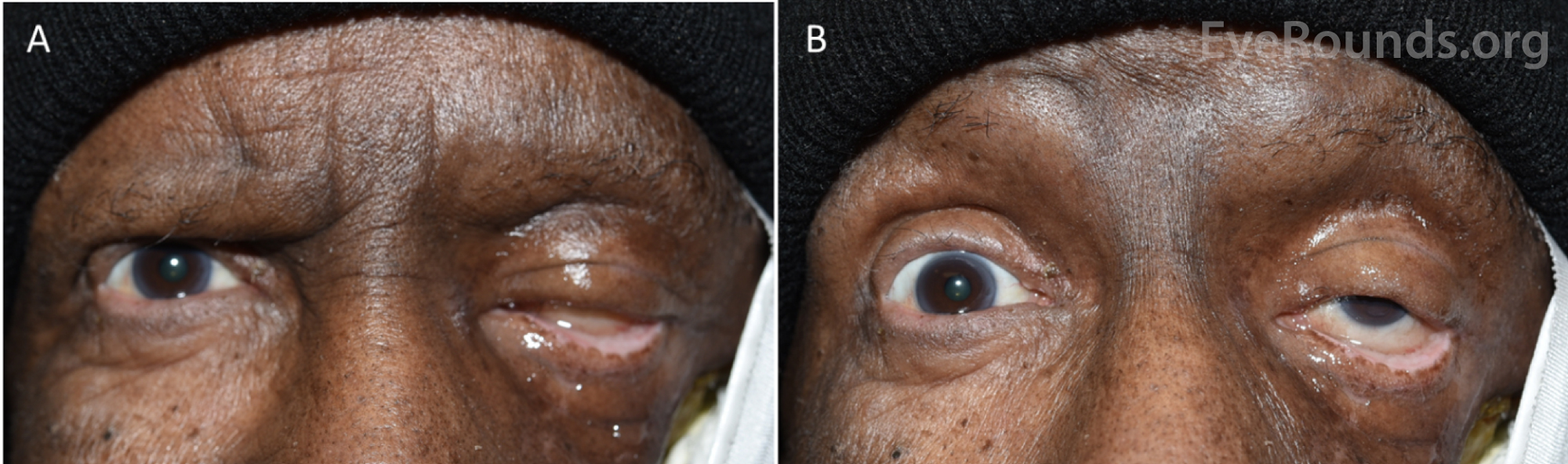
Figure 2. External photographs demonstrating complete ptosis of the left upper lid two weeks following injection of neurotoxin (A). Upon actively opening the eyelid, partial ptosis of the left upper eyelid is achieved (B). The eyelid is easily lifted for application of ocular medications and for ocular examination. Also note that after the neurotoxin tarsorrhaphy, there was interval resolution of the left ocular injection.
References
- Jacobson LK, Johnson MB, Dedhia RD, Niknam-Bienia S, Wong AK. Impaired wound healing after radiation therapy: A systematic review of pathogenesis and treatment. JPRAS Open. 2017;13:92-105. doi:10.1016/j.jpra.2017.04.001.
- Khairy H. Botulinum toxin A-induced ptosis: A safe and effective alternative to surgical tarsorrhaphy for corneal protection. Journal of the Egyptian Ophthalmological Society. 2014;107(1):20-22. doi:10.4103/2090-0686.134937.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.