
Chief Complaint: Blurry vision in the right eye (OD) following cataract surgery
History of Present Illness: A 59-year-old male patient presented with poor vision at far but good vision at near one month following uncomplicated cataract surgery OD.
Medical History:
Past Ocular History: Uncomplicated cataract surgery OD for posterior subcapsular cataract with target at plano. History of BB gun injury to OS as a child requiring repair of corneal laceration and iris defect. He also states that he had a retinal detachment repair at the time.
Medications:
Allergies: No known drug allergies.
The patient was noted to have a visually significant cataract in the right eye and had cataract surgery OD a few weeks ago. His cataract surgery OD was uncomplicated. The IOL was placed in the bag with a target of plano. He presented for his one month post-operative visit stating that he was having a hard time seeing far away and on refraction was clearly left myopic.
The anterior segment exam and dilated funduscopic exam of the right eye was normal. The posterior chamber lens was centered and clear, there was no evidence of capsular block or sulcus placement of the IOL which could have led to a myopic shift. He had no evidence of cystoid macular edema which could lead to a hyperopic shift. This led to a review of the lens calculations which uncovered a series of system and communication errors.
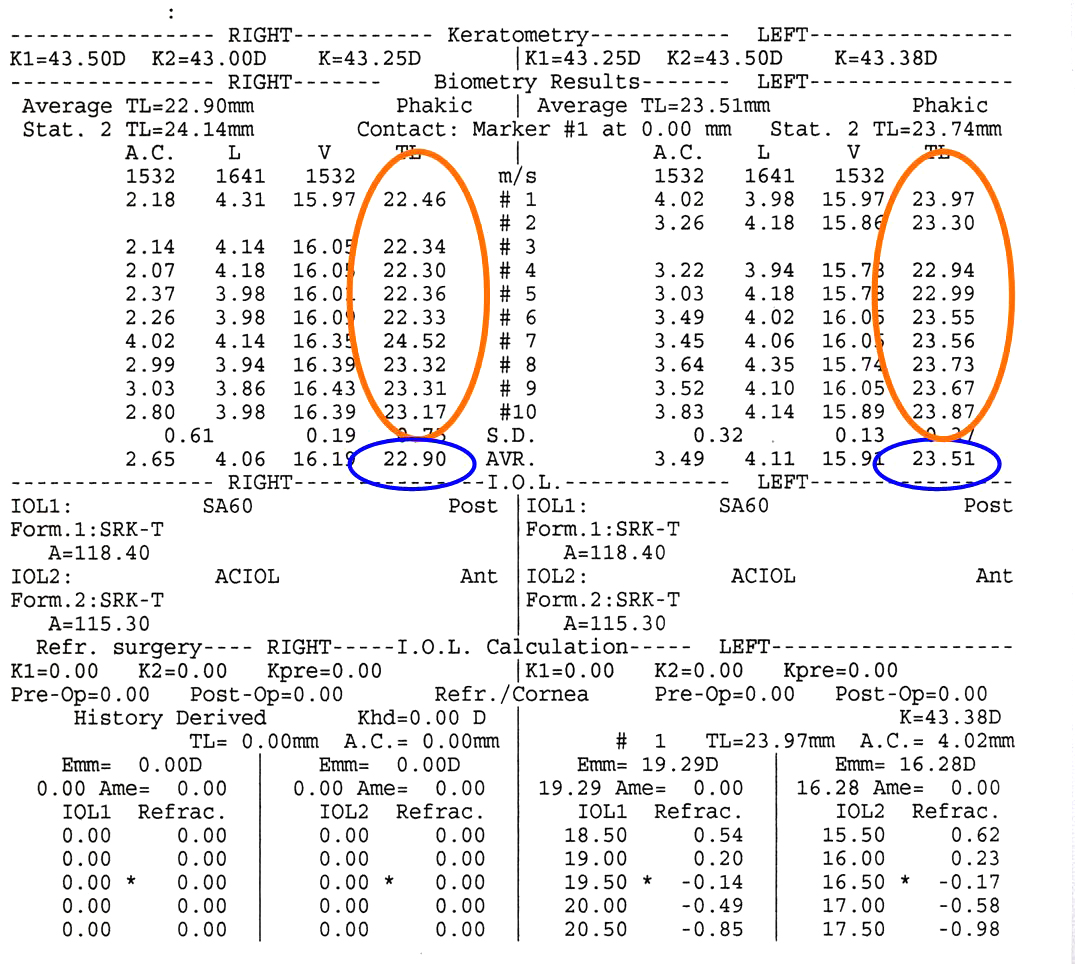 |
The axial eye length measurements used for the lens calculations were taken from an immersion A-scan that was done preoperatively. The axial eye lengths are usually calculated by our IOL master, but this machine was not fully operational at the time of the patient's initial exam. Note that the measurements of the right eye are very irregular and range from 22.30 to 24.52. The measurements for the left eye are similarly irregular. These variable values were averaged to generate the axial eye length of 22.90 mm OD and 23.51 mm OS. There is a 0.61 mm difference between the axial eye lengths (AEL). The technician did not relay the poor quality of the immersion scan to the physicians which led to the first communication issue.
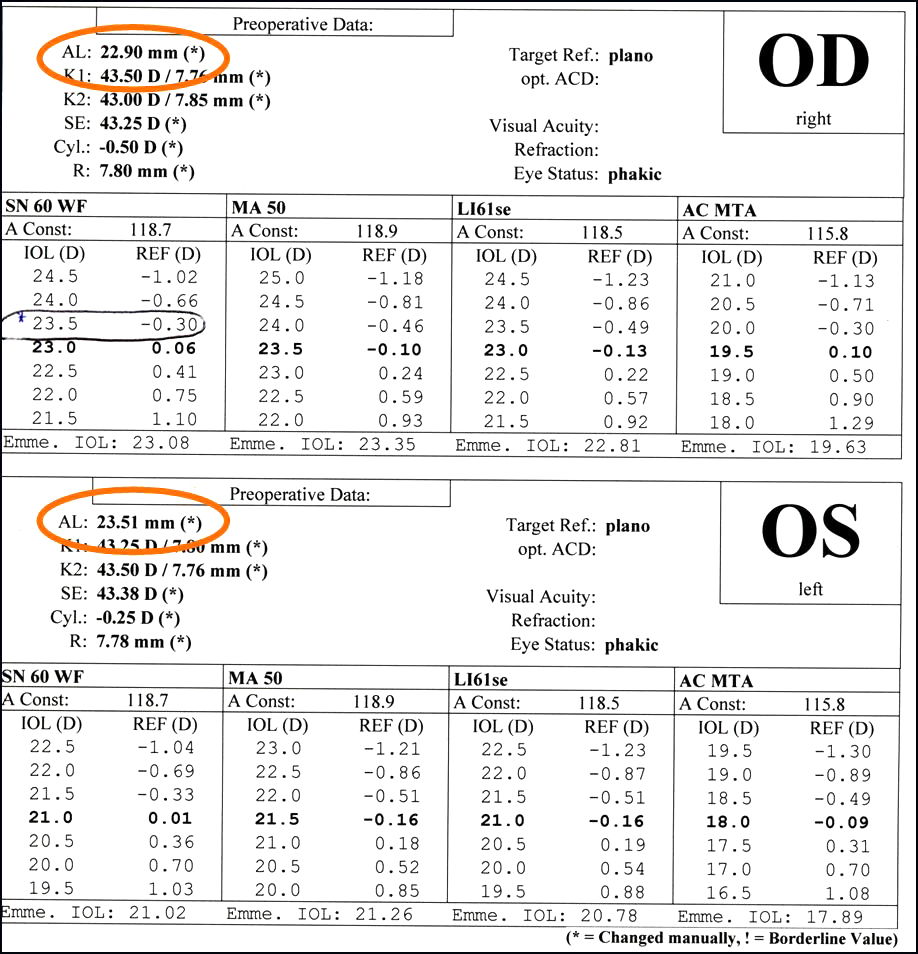 |
When the immersion ultrasound-generated axial eye lengths were entered into the IOL master IOL calculator program the lens choice for a slightly myopic target (23.5 D) was selected (figure 2). The attending asked about the discrepancy in AEL but thought that the trauma to the left eye had required a scleral buckle which could explain the AEL difference (communication issue). The attending did not investigate further or look at the immersion scans. As a result, an IOL was placed despite having poor quality immersion scans and a significant difference between AEL between both eyes. When the patient was discovered to have the large myopic surprise the IOL master was run again and the problem was discovered.
 |
The post operative IOL master shows a good quality scan (pseudophakic mode) and good agreement in AEL between eyes. The post operative IOL master is consistent with the myopic shift found from placing the 23.5 D lens chosen for the right eye.
Post-operative Course: The error in lens calculation and choice was explained in detail to the patient. The options of monovision, trying glasses, lens exchange and refractive surgery were discussed with him. He opted to try refractive surgery to correct the residual myopia in the right eye. He has since undergone PRK OD to correct his myopia and astigmatism.
We approached this event using the Swiss cheese model of accident causation first described by James Reason in 2000.(1) In this model, the various components of human systems are represented by slices of Swiss cheese. The holes in the cheese represent deficiencies in each component. An error in the system occurs when these holes line up in a single point in time as a result of specific circumstances.
In this case, we determined that there were a few systems-based and communication issues holes that led to placement of the wrong IOL. First, our routine method for measuring axial eye length (the IOL master) was not operational on the day that our patient came for his initial workup, necessitating the use of an A-scan immersion technique for measurements (systems issue). The A-scan is a more complicated technique requiring a skilled technician to perform accurately (systems issue). The technician did not report the AEL difference or the poor quality of the scans to the physicians (communication issue). The resident reviewing the initial IOL calculations was a new second-year resident who was not yet accustomed to reviewing IOL measurements (systems issue). The attending who reviewed these calculations noted the AEL differences but assumed that the injury to the left eye included a scleral buckle repair which could explain the AEL difference (communication issue) and as a result the attending did not look deeper into the source of the AEL difference which may have uncovered the poor quality ultrasound (communication issue).
After caring for the patient, it is important for the institution to attend to the systems of care that could be safer and less likely to allow alignment of the Swiss cheese that led to placing the wrong IOL. We, of course, will try to have the IOL master available at all times. When axial eye length calculations need to be performed by A-scan, they are performed by our technicians who have significant experience in this technique and we have enhanced our training in this area. We also used the EyeRounds website and a conference to share this experience with other opthalmologists to help them fine tune their systems to assure perfect IOL measurements for their operative patients.
Breaking bad news to patients is one of the more difficult patient interactions a physician will encounter in his or her career. Prior reviews of literature demonstrate that often patients to whom such news is being delivered are dissatisfied with the information they receive or the way in which the information is presented.(2) Rabow and McPhee developed a practical and comprehensive model of delivering bad news to patients.(3) It includes the principles of communicating information to patients in a simple mnemonic, ABCDE.
We tried to adhere to these principles when we discussed this situation with our patient. Everyone who communicated with the patient after his surgery was aware of his clinical and operative history. When the error in lens choice was discovered, the situation was explained in detail to the patient and his fiancè by the primary surgeon. The lens measurements were reviewed with the patient in a way that was understandable to him, and the reason for the error was also explained. He and his fiancè understood and were able to ask questions about the surgical and non-surgical options to optimize the vision in the right eye. After a candid discussion about the risks and benefits of all of the options, we decided together that a refractive procedure for the right eye would be the safest and most effective option. Most importantly, we apologized to the patient for our error and for the fact that he would require an additional procedure.
Medical errors are an unfortunate but real aspect of any medical field. Assessing the error based on the various systems at play, and addressing each system flaw with a specific solution can help made medical systems more solid and less like slices of Swiss cheese. Open communication with patients about the nature of the error is of paramount importance; adhering to principles of honesty and compassion can help ensure an effective interaction.
Gandhi N, Oetting TA. Communication Issues Following a Post Operative Surprise: Blurry Vision Following Cataract Surgery. EyeRounds.org. January 15, 2010; Available from: http://www.EyeRounds.org/cases/105-Professionalism-post-op-surprise.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
