
Chief Complaint: Right upper eyelid mass
History of Present Illness: A 6 month old male was referred by his pediatrician to the Oculoplastics Clinic for evaluation of a right upper eyelid mass. His mother states that she noticed some fullness in this area when the patient was three months old and states that it has become progressively larger and more noticeable. As this area grew in size, she noticed drooping of the right upper eyelid as well. The area had not been red or irritated and did not seem to bother the patient. He had otherwise been in good health.
Medical History: The patient was born at 38 weeks by Cesarean section for fetal distress. He had normal development and reached all milestones. He had no other medical problems.
Medications: None
Allergies: No known drug allergies.
Family History: Non-contributory.
Social History: Lives with mother and father who were present for the exam.
Visual acuity: Central steady and maintained OD, Central steady and maintained OS.
Cycloplegic refraction: +2.00 OD, +2.00 OS
Globes soft to palpation OU.
Pupils: 6 mm OU in dark, 4 mm OU in light. No RAPD.
Motility: Full OU.
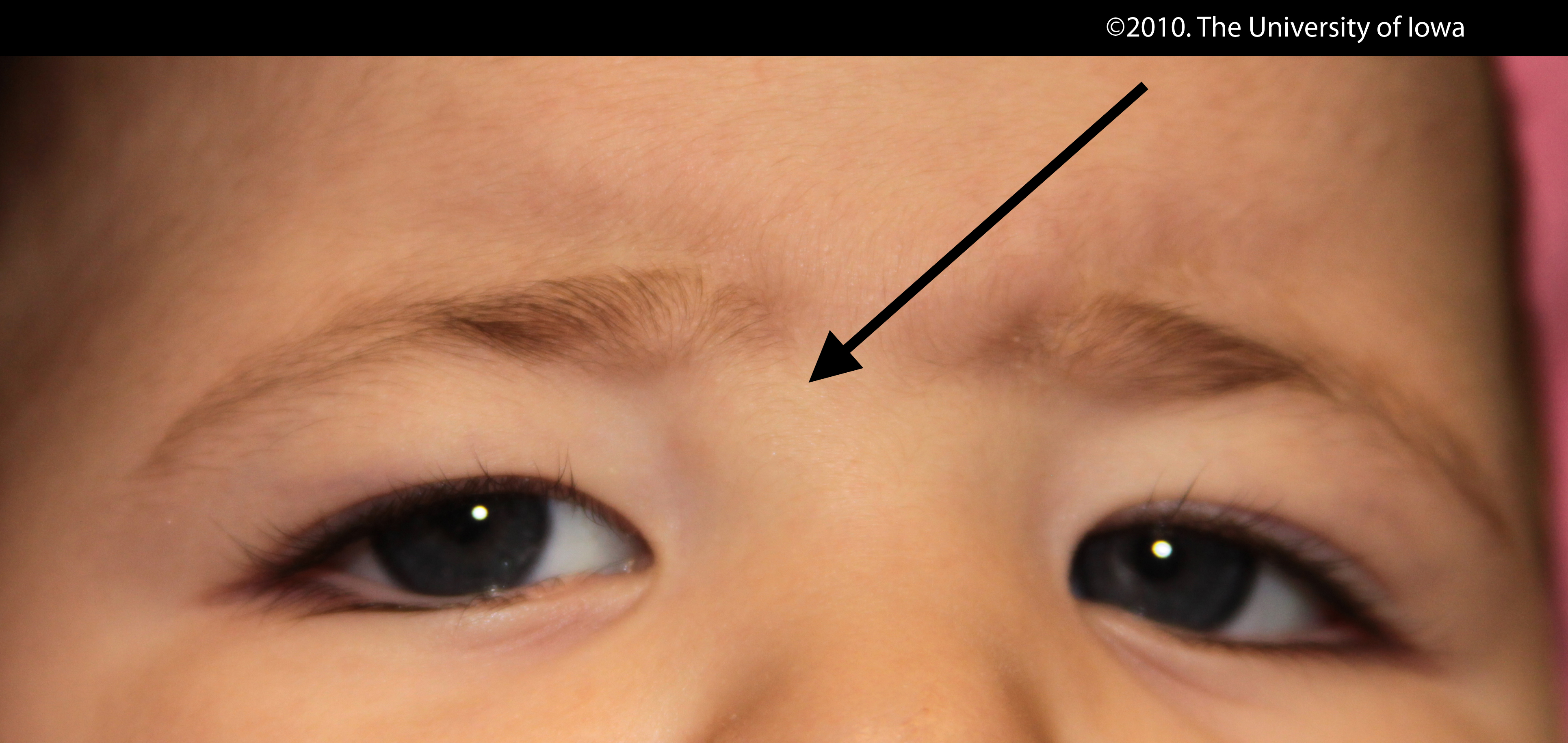
External exam: 2 cm x 2 cm soft mobile mass at the superior aspect of right lateral orbital rim. No edema or erythema. Not tender to palpation. No globe displacement. (See Figures 1 and 2.)
| Figure 1. This external photograph demonstrates a subcutaneous mass at the lateral aspect of the right upper eyelid, under the tail of the brow. Note that the overlying skin is not erythematous, edematous or discolored. | Figure 2: A closer view of the lateral orbital lesion that appears to rest at the superior aspect of the right lateral orbital rim. |
 |
 |
Anterior segment exam: Conjunctiva/Sclera normal OU, Corneas clear OU, Anterior chamber deep and quiet OU, Irides normal OU, Lenses clear OU.
Dilated funduscopic exam: Macula, vasculature and periphery normal OU.
The location and presentation of this lesion were most consistent with a dermoid cyst, and excision of the lesion was recommended. This was discussed with the patient's mother who consented to excision of the lesion.
The patient underwent an uncomplicated anterior orbitotomy through a superior eyelid crease incision and excision of the lesion.
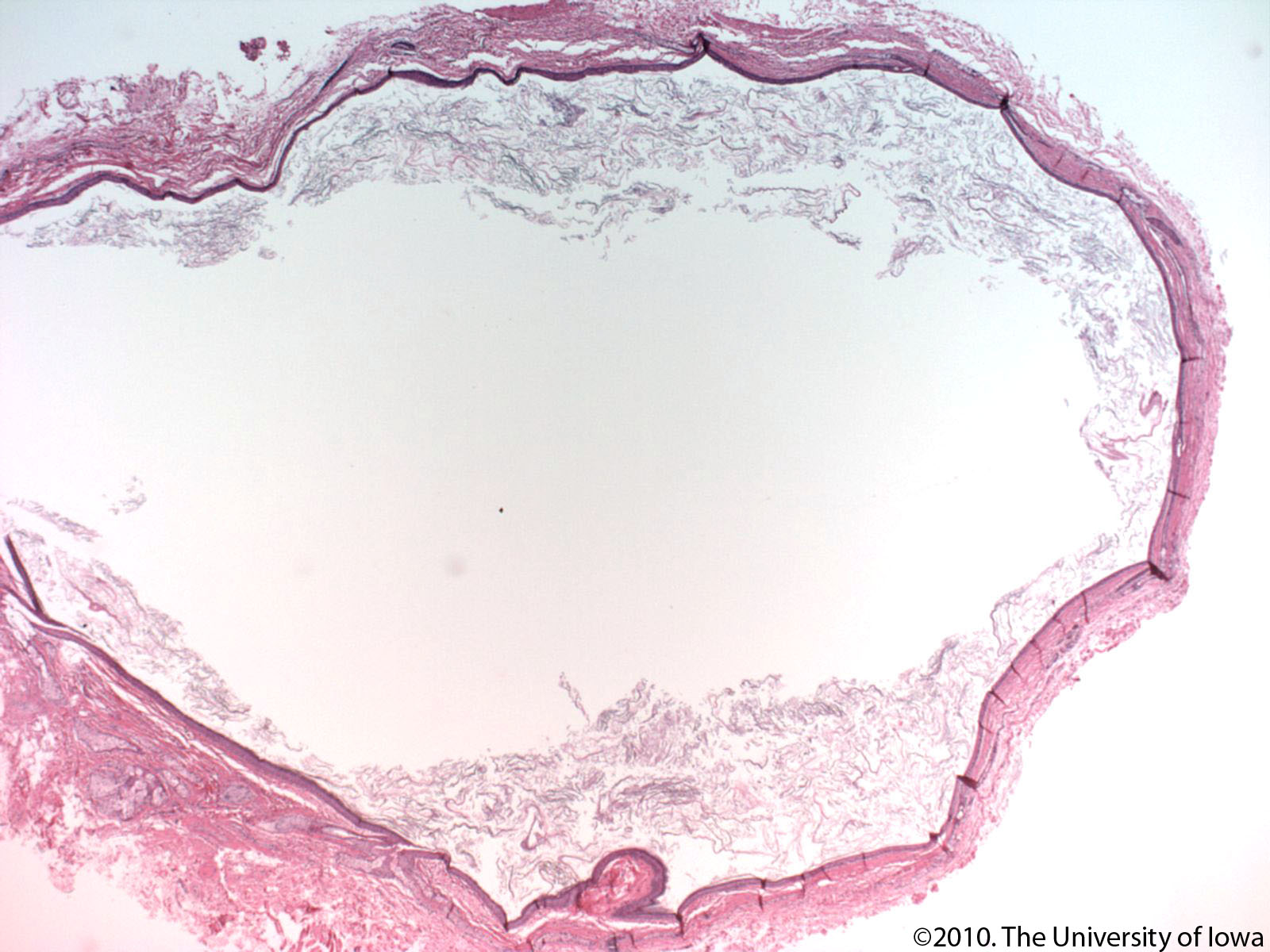
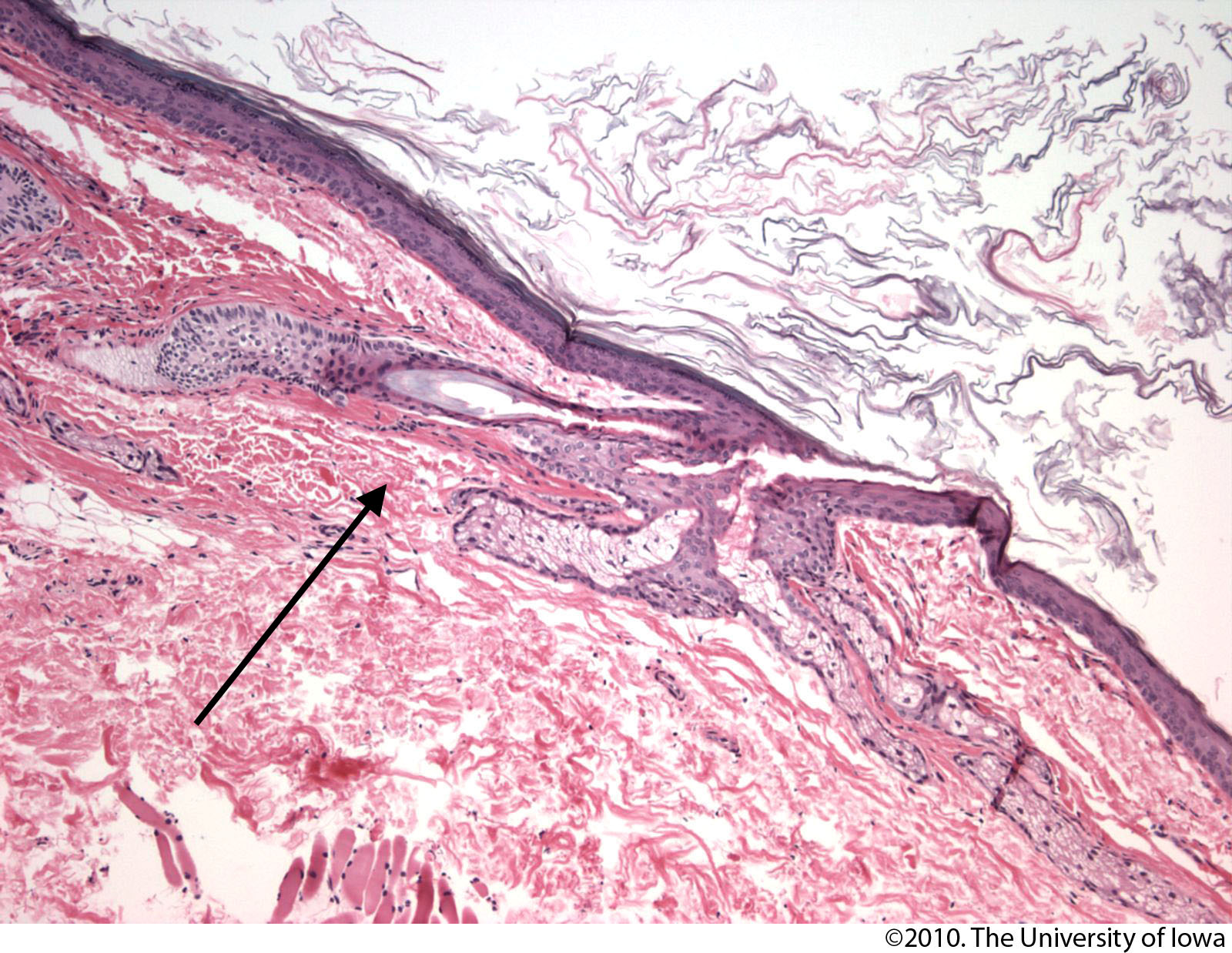
Pathology exam demonstrated a cystic structure lined with stratified squamous keratinizing epithelium and with skin adnexal structures in the cyst wall, consistent with a dermoid cyst. (See Figures 3 and 4).
| Figure 3: This is a 10X Hematoxylin and Eosin stained image of a dermoid cyst from a similar case. Note the keratin filled lumen and the epithelial lining. | Figure 4: This 50X view of the cyst wall demonstrates a hair follicle (arrow), one of the adnexal structures that are commonly found in walls of dermoid cysts. Note the kertinized stratified squamous epithelium lining the cyst. |
 |
 |
Diagnosis: Dermoid Cyst
Lateral anterior dermoid
Medial anterior dermoid
Cyst with spontaneous rupture
Deep dermoid with mass effect
Incidence: Accounting for 3-9% of orbital tumors in children, dermoid cysts are one of the most common non-inflammatory space-occupying orbital lesions in the pediatric population. Dermoid cysts are generally thought to be congenital lesions of childhood with the vast majority presenting in the first few years of life. However, deep lesions can go undiagnosed for years and may present for the first time in late adulthood (Shields 1997).
Pathophysiology: Dermoid cysts are congenital choristomas that result from the sequestration of embryonic epithelium between orbital bones, usually along suture lines. These ectodermal tissues are "pinched off" in characteristic locations in the orbit and grow until they become clinically apparent (Sherman 1984). Histologically, the cysts are classified as either epidermoid or dermoid cysts. Both cysts are lined with keratinizing epithelium, but the dermoid cyst wall also contains such adnexal structures as hair follicles, sebaceous glands and sweat glands (Lane 1987). The cyst cavity typically contains some combination of sebaceous fluid, keratin, calcium and cholesterol crystals (Ahuja 2006). There is often evidence of chronic granulomatous inflammation in the cystic structures as well.
Clinical Features: Dermoid cysts may be categorized based on location and are often classified as either anterior lesions or deep lesions. Each type of lesion has distinguishing clinical features.
Anterior lesions typically present in the first few years of life as smooth, well-circumscribed, subcutaneous, painless masses. The most common location for the anterior dermoid cyst is at the superolateral aspect of the orbit at the frontozygomatic suture, as seen in the case described here. Medial lesions occur less frequently and often arise from tissue sequestered in the frontoethmoidal or frontolacrimal sutures (See figure 5). If there is no orbital extension, the posterior aspect of the mass may be palpable. Because of their anterior location, these lesions do not usually cause globe displacement, but they can cause visually significant ptosis if they grow to a large enough size.
 |
Deep lesions are more insidious, and often develop at the sphenozygomatic or sphenoethmoidal suture (Henderson 2007). Their presence is usually declared by mass effect on surrounding structures: Patients with deep lesions may present in late adolescence or adulthood with painless, progressive proptosis, motility deficits or diplopia. Extension into intracranial fossae is possible if the frontal or sphenoid bones are involved. Temporal fossa involvement is rare but reported; this may result in intermittent proptosis associated with chewing, as positional changes of the temporalis muscle during chewing transmit pressure to the lesion and, hence, to the orbit (Emerick 1997).
Dermoids may also straddle the orbital bones (most commonly the lateral orbital wall) such that they have both an anterior lobe and a deeper orbital lobe. These so-called "dumbbell" dermoids must be imaged to assess the extent of the orbital component before excision (Figure 6).
 |
Dermoid cysts can spontaneously leak their cystic substances into surrounding soft tissues, causing a localized inflammatory response that can masquerade as primary inflammation or infection. While this is rarely the first presenting sign for an anterior dermoid, it may be the first presenting sign of a deep dermoid.
Workup and Imaging: Classic dermoid cysts located at the frontozygomatic suture whose posterior aspect can be palpated may be diagnosed clinically without imaging. Medial lesions require imaging to rule out an encephalocele or mucocele prior to surgical excision. Deep orbital lesions also require imaging for diagnostic purposes and to help with surgical planning.
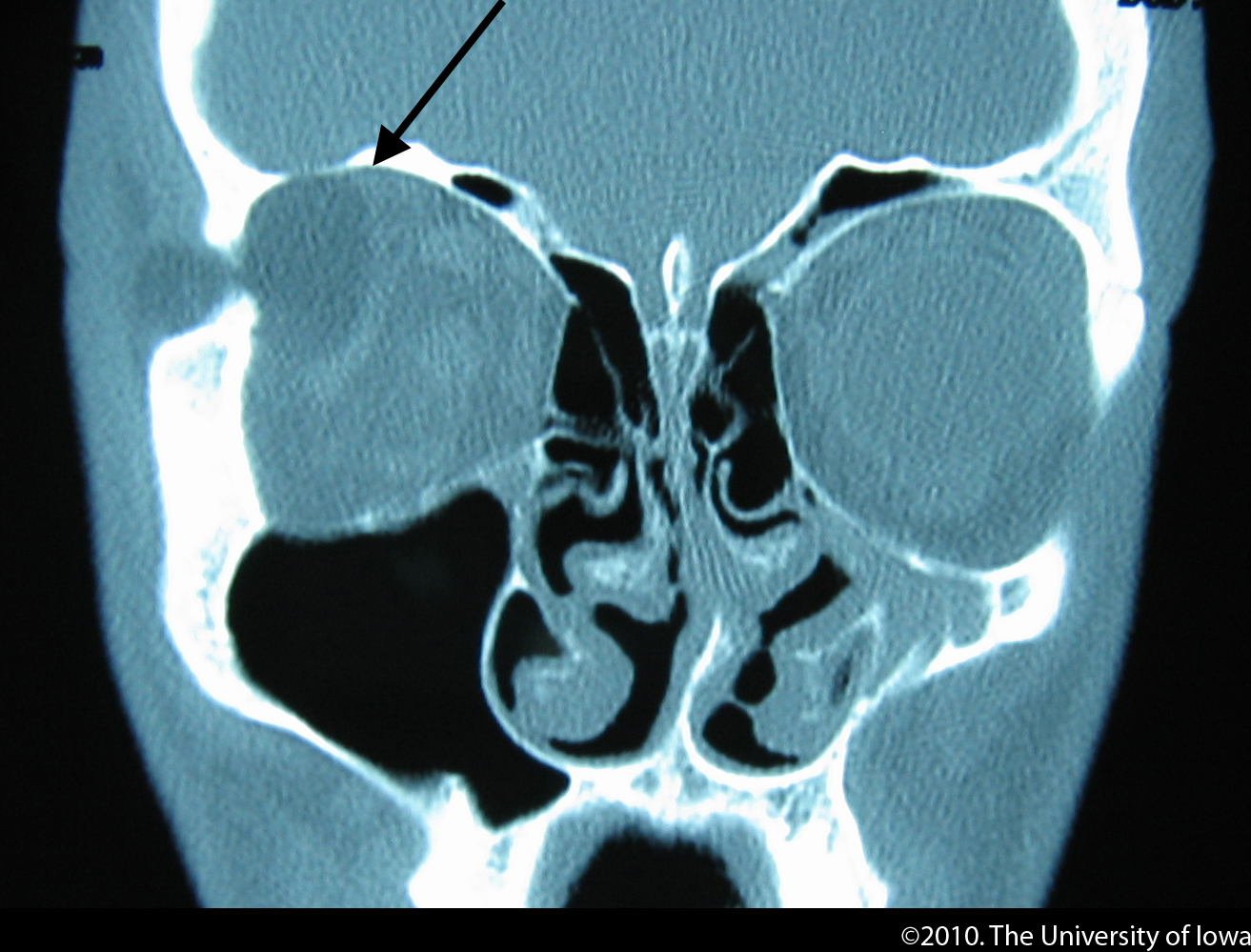
CT is a commonly used modality for imaging orbital dermoid cysts. On CT, a dermoid typically has a hyper-dense wall and a hypo-dense cavity which remains non-enhancing with contrast (Figure 7). The central cavity may appear heterogeneous as a result of keratin and other cystic debris (Shields 2004). An estimated 85% of dermoids are associated with such bony changes as smooth pressure erosion near the affected suture, clefts, and full-thickness bony channels (Emerick 1997). CT imaging is especially useful delineating these bony changes. However, caution should be used whenever using CT imaging in children, due to the relatively high dose of radiation that can predispose to tumors.
MRI is another oft-used imaging modality for dermoid cysts, and has the added advantage of not exposing the patient to radiation. This is especially important in the pediatric population. The lesions are generally hypointense on T1-weighted imaging with respect to fat and are best visualized using fat-suppression techniques. The lesions tend to be hyperintense on T2-weighted imaging. Similar to the CT imaging characteristics, these lesions typically do not enhance with contrast (Shields 2004).
Figure 7: This coronal CT image without contrast demonstrates a lateral dermoid cyst with the characteristic hyperdense cyst wall and hypodense cyst cavity. |
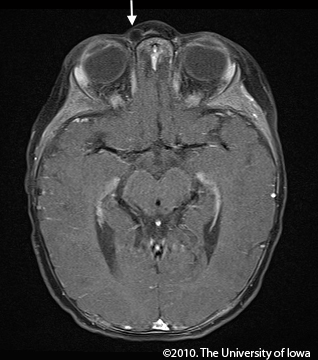
Figure 8: This axial T1-weighted MRI image demonstrates a right medial dermoid with a hyperintense cyst wall and hypointense cyst cavity. This study helps to rule out a mucocele or encephalocoele in the setting of a medial lesion. |
|---|---|
 |
 |
The treatment of orbital dermoid cysts is surgical. Excision is recommended in most cases to prevent the possibility of spontaneous rupture or cutaneous fistula formation. The primary goal of excision is to remove the dermoid with the cyst wall intact without causing an iatrogenic rupture. Leakage of the cystic contents into the orbit can result in significant inflammation and recurrence, while lesions removed in their entirety rarely recur.
The surgical approach depends upon the location of the lesion. Lateral or medial dermoids located anteriorly can often be approached via an anterior orbitotomy through a superior eyelid crease incision (Kersten 1988). This is preferable to making an incision directly over the lesion because a superior eyelid crease scar can be hidden in a skin fold. The use of a cryo probe can help in the delivery of the cyst intact in these cases. Deeper lesions are approached based upon their location in the orbit and relationship to adjacent structures. Intracranial extension requires a multi-disciplinary surgical approach for complete excision.
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
|
Ahuja R et al. Orbital Dermoids in Children. Semin Ophthalmol. 2006;21:207-211.
Emerick G et al. Chewing-Induced Visual Impairment from a Dumbbell Dermoid Cyst. Ophthal Plast Reconstr Surg. 1997;13(1):57-61.
Henderson J and Garrity J. "Cysts and Celes" in Henderson's Orbital Tumors. Mayo Foundation for Medical Education and Research, 2007; pp. 33-39.
Kersten, RC. The eyelid crease approach to superficial lateral dermoid cysts. J Pediatr Ophthalmol Strabismus. 1988;25(1):48-51
Lane, C et al. Orbital Dermoid Cyst. Eye. 1987;9:504-511.
Sherman R et al. Orbital dermoids: clinical presentation and management. Br J Ophthalmol. 1984;68 642-652.
Shields J and Shields C. Orbital Cysts of Childhood Classification, Clinical Features and Management. Surv Ophthalmol. 2004;49(3):281-299.
Shields J et al. Orbital Dermoid Cysts: Clinicopathologic Correlations, Classification, and Management, the 1997 Josephine E. Schueler Lecture. Ophthal Plast Reconstr Surg. 1997;13(4): 265-276.
Gandhi N, Syed NA, Alen R. Dermoid Cyst. EyeRounds.org. posted July 26, 2010; Available from: http://www.EyeRounds.org/cases/115-dermoid-cyst.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
