
Chief Complaint: 38-year-old male with blurry distance vision
History of Present Illness: The patient noticed blurry distance vision and problems seeing at night for years, more noticeably in his left eye than in his right. When driving at night, he noticed a significant amount of glare from oncoming headlights. On a previous examination 15 years ago, he was informed he had cataracts.
Past Ocular History: The patient wore glasses and had no other ocular history, including no history of amblyopia.
Medical History: No chronic medical conditions, including no diabetes or history of steroid use.
Medications: None
Allergies: No known drug allergies
Family History: Father and brother had posterior polar cataracts.
Social History: The patient smoked but did not drink alcohol.
Review of Systems: A full review of systems was negative.
Ocular motility: Full, both eyes (OU), no nystagmus
Intraocular pressure (IOP): 14 mmHg OD, 17 mmHg OS
Pupils: Reactive to light in each eye from 4mm in the dark to 2 mm in the light. No relative afferent pupillary defect (RAPD).
Confrontation visual fields: Full, OD and OS.
 |
 |
 |
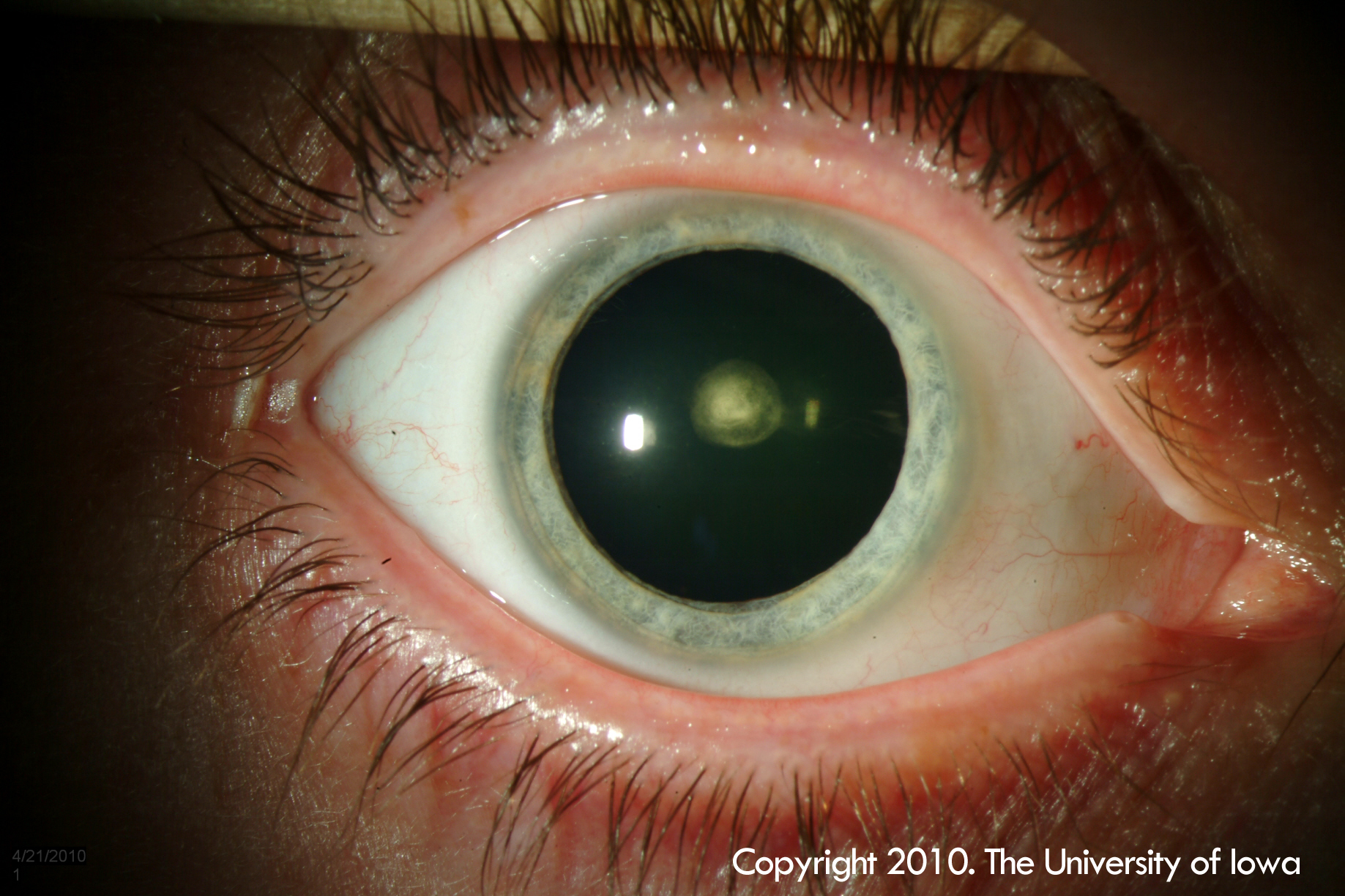
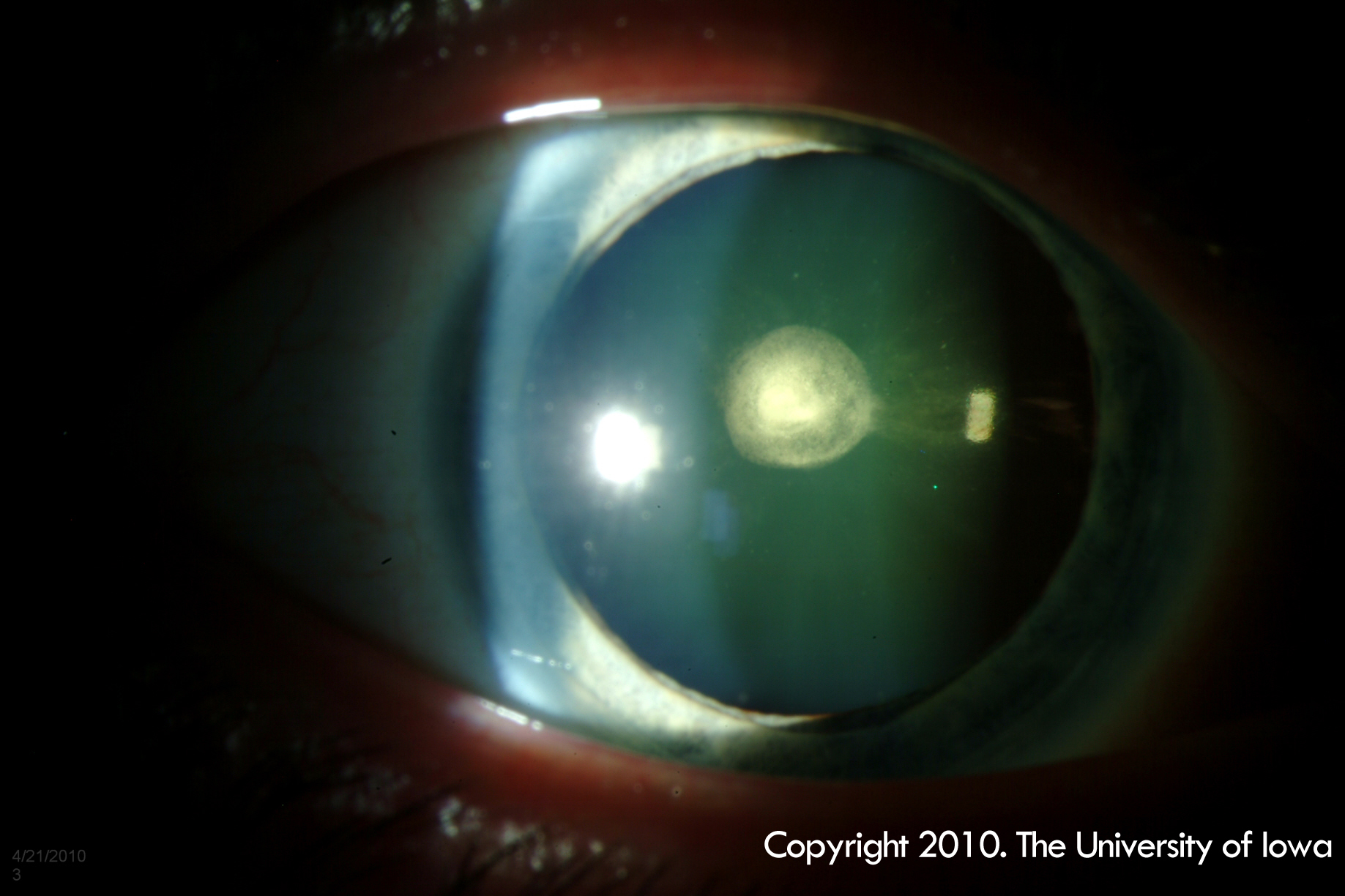
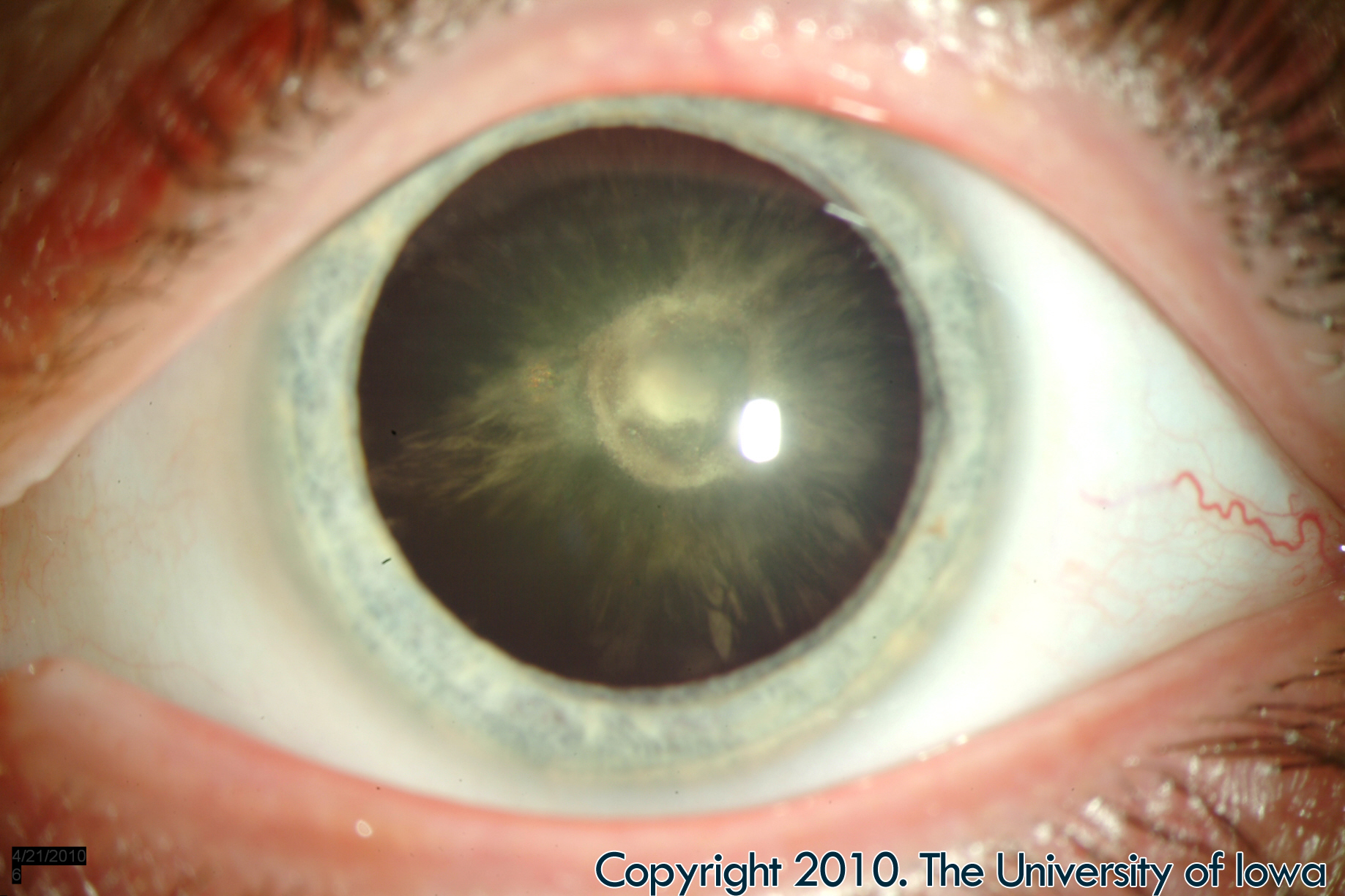
| 1A: Posterior polar cataract of the right eye (click on image for higher resolution) | 1B: Slit lamp photo of the posterior polar cataract in the right eye (click on image for higher resolution) | 1C: Red reflex showing posterior polar cataract of the right eye (click on image for higher resolution) |
 |
 |
 |
| 2A: Posterior polar cataract of the left eye (click on image for higher resolution) | 2B: Slit lamp photo of the posterior polar cataract of the left eye. Note the posterior subcapsular change and anterior subcapsular/cortical spokes (click on image for higher resolution) | 2C: Red reflex of the left eye demonstrating the posterior polar cataract (click on image for higher resolution) |
The patient’s symptoms and anterior segment findings were consistent with posterior polar cataracts. His vision could be improved with refraction to 20/20-2 OD and 20/30-2 OS. Options for management were discussed with the patient including trying a new pair of glasses to improve distance vision or pursuing cataract surgery, which would likely improve distance vision as well as improve symptoms of decreased night vision and glare. Because the cataract was significantly affecting his activities of daily living, the patient opted to pursue cataract surgery for the left eye. The patient was informed that cataract surgery for posterior polar cataracts is associated with increased risk of capsular rupture and vitreous loss that can lead to worse visual outcomes.
Because of the increased complexity of the case, the surgical plan involved obtaining anesthesia with a retrobulbar block, avoiding hydrodissection, sculpting out a bowl in the anterior cortical and nuclear material prior to performing gentle viscodissection, avoiding rotation of the nucleus, and using the anterior vitrector to remove nuclear and cortical material with very low aspiration and slow cut rate settings. In this video you will note that after the cortical material was removed, the surgeon opted not to polish the remaining posterior subcapsular fibers to avoid rupturing the posterior capsule (See Video 1). This remaining material was treated with a Nd:YAG (neodymium yttrium aluminum garnet) laser capsulotomy post-operatively.
Posterior-Polar-Cataract from EyeRounds on Vimeo. |
| Another surgical video demonstrates a similar technique but uses irrigation and aspiration to remove the cortical material rather than anterior vitrectomy. This video is from http://www.facebook.com/video/video.php?v=454807036140 |
Neither case resulted in posterior capsular rupture.
Pathophysiology: Posterior polar cataract is a congenital condition that can be sporadic or familial. Sporadic posterior polar cataracts are typically unilateral and associated with remnants of the tunica vasculosa lentis, an embryologic hyaloid structure that fails to regress. Familial posterior polar cataracts are typically bilateral and follow an autosomal dominant pattern of inheritance (Basic and Clinical Science Course, Section 11). More recently, mutations resulting in a 17-base-pair duplication in the PITX 3 gene have been associated with posterior polar cataract. This gene codes for a transcription factor that participates in anterior segment and lens development (Berry et al. 2004, Addison et al. 2004). The exact mechanism of how the mutation causes cataract is unknown, but the result is dysplastic, abnormal lens fibers that, as they migrate posteriorly from the equator, form an opacity in the region of the central posterior capsule. The opacity is usually a round discoid plaque, clearly demarcated from the rest of the lens and often associated with vacuoles in the lens surrounding the plaque (Eshaghian and Streeten 1980). Satellite opacities, which may represent fluid entering the lens, can also develop with time around the original plaque. The abnormal lens fibers can become adherent to the central posterior capsule, and the capsule around the plaque is often weakened. Thus, posterior capsular rupture is a feared complication when removing this type of cataract (Osher et al.1990). These cataracts often present in the first few months of life, and if visually significant at an early age, can lead to amblyopia. Most posterior polar cataracts are stationary but can progress in severity over time.
Treatment: When posterior polar cataracts become visually significant (either in infancy if the cataracts are large enough to be amblyogenic, or in adulthood when they cause glare), they can be surgically removed. However, the high risk of posterior capsular rupture makes surgical removal often very difficult. There have been reported rates of posterior capsular rupture in 26-36% of cases depending on the series studied (Osher et al. 1990, Vasavada and Singh 1999). More recent studies demonstrate lower rates of posterior capsular rupture (Hayashi 2003). To avoid posterior capsular rupture the following techniques have been described in the literature.
| this video from: http://www.facebook.com/video/video.php?v=472413536140 |
In summary, there are various surgical techniques that can be utilized to minimize the risk of posterior capsular tear in posterior polar cataract extraction. Avoid hydrodissection, perform hydrodelineation, use slow motion phacoemulsification settings, consider viscodissection of the epinuclear material, and do not polish the remaining posterior polar remnant. Laser posterior capsulotomy can safely be performed post-operatively.
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
|
Addison PK, Berry V, Ionides AC, et al. Posterior polar cataract is the predominant consequence of a recurrent mutation in the PITX3 gene. Br J Ophthalmol 2005;89(2):138-141
Berry V, Yang Z, Addison PK, et al. Recurrent 17 bp duplication in PITX3 is primarily associated with posterior polar cataract. J Med Genet 41(8):e109
Chapter 4. Embryology: Rosenfeld,SI et al. Section 11. Lens and Cataract. 2007-2008 Basic and Clinical Science Course. San Francisco: American Academy of Ophthalmology; 2007; p. 34-35.
Eshaghian J, Streeten BW. Human posterior subcapsular cataract; an ultrastructural study of the posteriorly migrating cells. Arch Ophthalmol 1980 98:134-143
Fine IH, Packer M, Hoffman RS. Management of posterior polar cataract. J Cataract Refract Surg 2003;29:16-19
Hayashi K, Hayashi H, Nakao F, Hayashi F. Outcomes of surgery for posterior polar cataract. J Cataract Refract Surg 2003; 29:45-49
Kelman CD. V Groove phaco technique: Fast, easy, safe: Interview with Dr. Kelman. Ophthalmology Times 1994;19(18):12
Lee MW, Lee YC. Phacoemulsification of posterior polar cataracts—a surgical challenge. Br J Ophthalmol 2003;87(11):1426-1427
Lim Z, Goh J. Modified epinucleus pre-chop for the dense posterior polar cataract. Ophthalmic Surg Lasers Imaging 2008;39(2):171-173
Osher RH, Yu BC, Koch DD. Posterior polar cataracts: a predisposition to intraoperative posterior capsular rupture. J Cataract Refract Surg 1990;16:157-162
Osher RH. Slow motion phacoemulsification approach (letter). J Cataract Refract Surg 1993;19:667
Vasavada A, Singh R. Phacoemulsification in eyes with posterior polar cataract. J Cataract Refract Surg 1999;25:238-245
Vasavada AR, Desai JP. Stop, chop, chop and stuff. J Cataract Refract Surg 1996;22:526-529
Vasavada AR, Raj SM. Inside-Out delineation. J Cataract Refract Surg 2004;30:1167-1169
Vasavada AR, Raj, SM. Posterior polar cataract and preexisting posterior capsular defect. Cataract & Refractive Surgery Today Europe 2008 March:73-77
Birkholz ES, Oetting TA, Kitzmann AS. Posterior Polar Cataract. EyeRounds.org. January 22, 2011. Available from https://eyerounds.org/cases/128-Posterior-Polar-Cataract.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
