Chief complaint: Decreased vision
History of Present Illness: The patient is a 64-year-old female with a history of macular degeneration who presented to clinic for follow-up. Her vision has slowly declined over the past decade. She continues to drive, but limits this to driving to and from work, which is in close proximity to her home.
Past Ocular History: age-related macular degeneration
Past Medical History: hypertension, hypothyroidism
Medications: losartan, levothyroxine, vitamins
Allergies: paroxetine, lisinopril, indomethacin
Family History: non-contributory
Social History: She is a former smoker (quit at the age of 30 years). She drinks alcohol occasionally.
Review of systems: negative except for HPI
Visual Acuity: (Best corrected)
Pupils: 4 mm → 2 mm both eyes (OU)
Extraocular movements: Full OU
Confrontation visual fields: Central scotoma OU
Intra-ocular pressure:
External: Normal OU
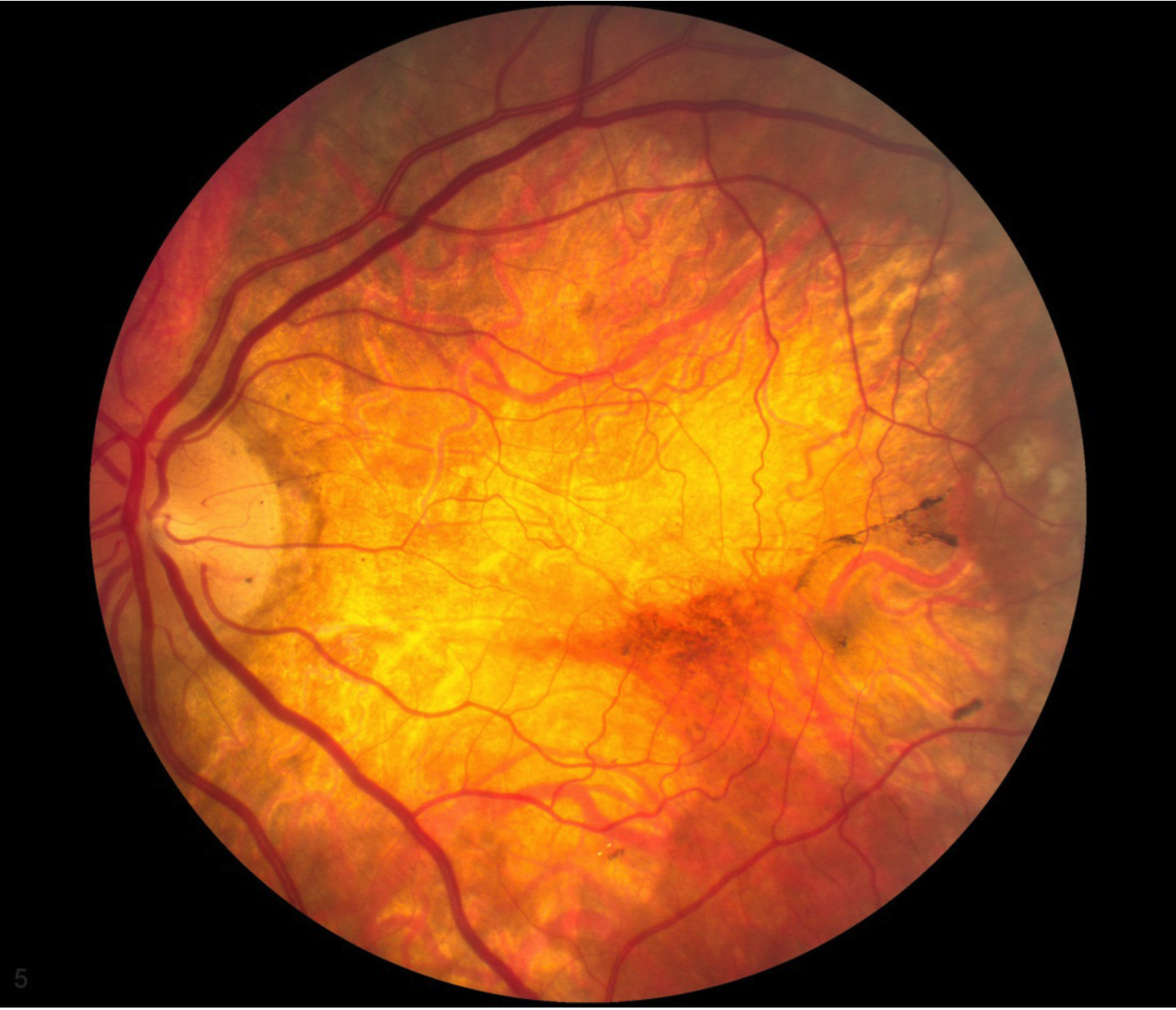
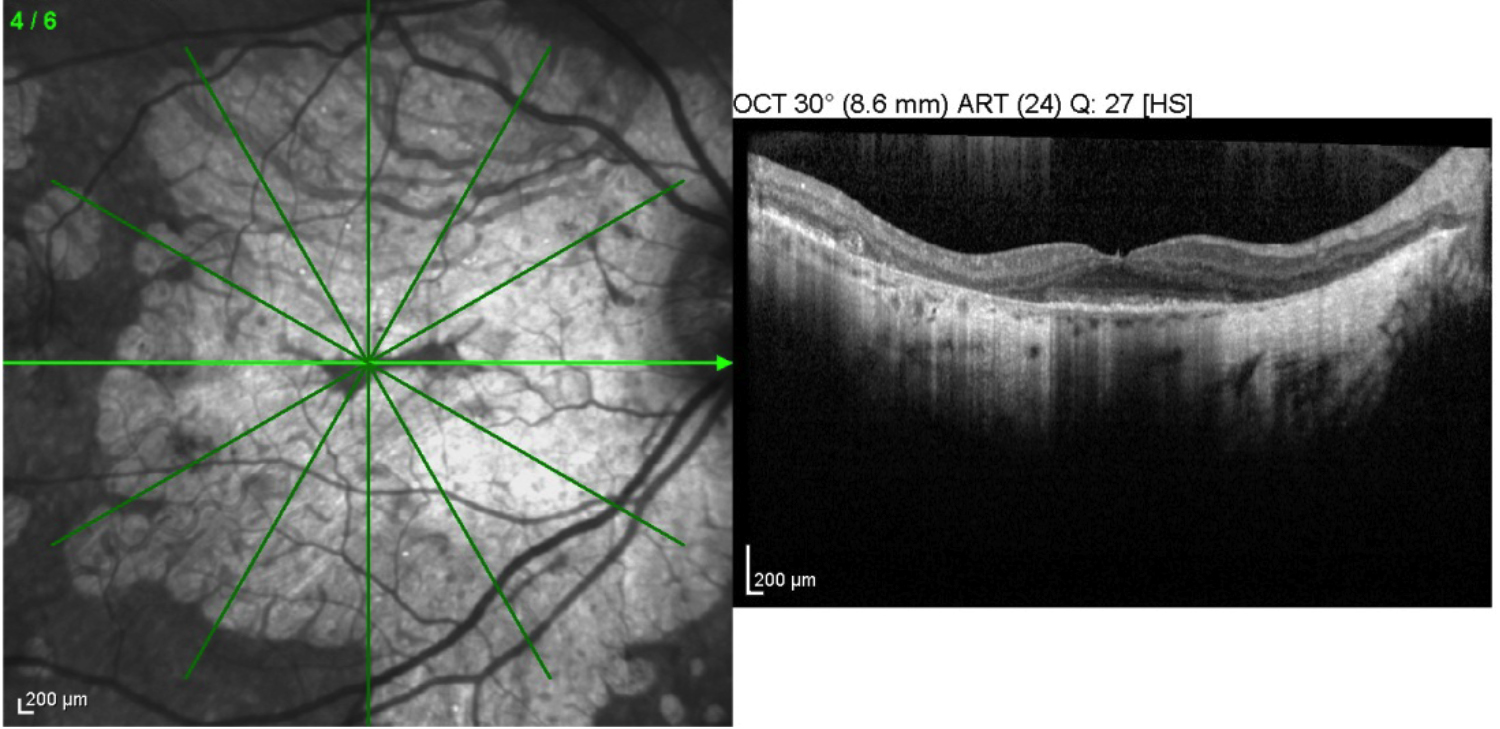
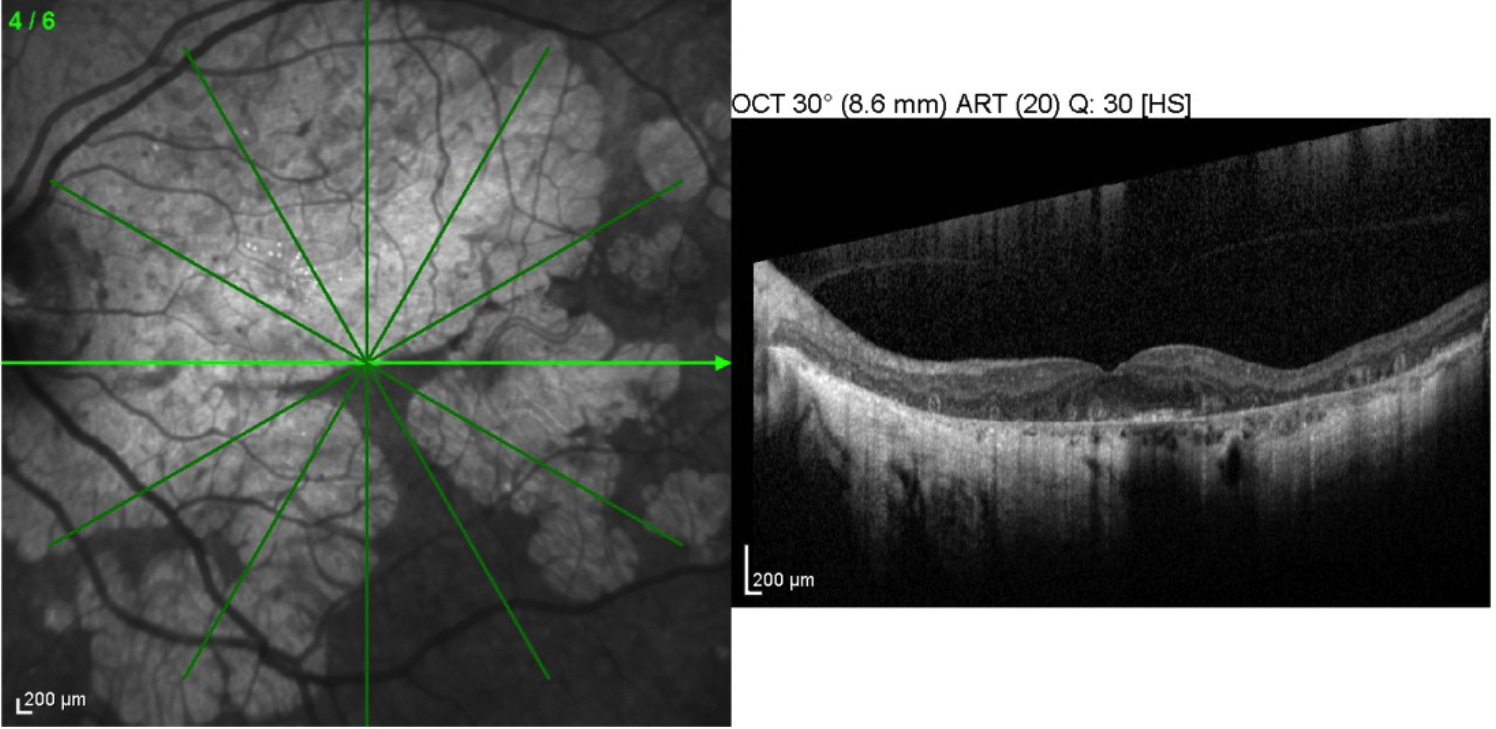
The optic nerves have a cup-to-disc ratio of 0.2. The media are clear OU and the vessels are of normal caliber for her age. Both eyes have extensive geographic atrophy in the macula with peripapillary involvement, and extensive peripheral drusen with retinal pigment epithelial changes and atrophy. There is a small island of preserved retina near the fovea OU. This island is in a slightly different position with respect to the foveal center in each eye (Figure 1).
|
|
 |
 |
 |
Peninsular geographic atrophy from dry age-related macular degeneration with bilateral central visual field loss that still meets the requirements for driving in Iowa.
| Visual Acuity (in at least one eye) | Restrictions, if any |
|---|---|
20/40 |
No restrictions |
20/41-20/70 |
No driving when headlights are required
|
20/71-20/199 |
Discretionary issuance
|
= 20/200 |
License denied |
Bioptic Telescopes |
Not allowed to achieve the visual acuity standards noted above |
Visual Field |
|
>140 degrees binocular or monocular |
No restrictions |
< 140 degrees but >110 degrees |
Vehicle must have left and right outside mirrors. |
<110 degrees binocular or |
Discretionary issuance
|
<75 degrees binocular or monocular |
Discretionary issuance
|
<20 degrees binocular or monocular |
License denied |
Driving is a daily activity that the majority of us take for granted. Ophthalmologists not only have a role in treating eye diseases and preserving vision, but also in looking out for the well-being of the patient. Part of this is determining a patient's ability to drive, because if they are incapable of driving safely, they not only put themselves at risk, but also others on the road. Visual acuity, contrast sensitivity, visual fields, and visual processing are the most recognized factors in driving performance.[2]
Driving laws are made by state legislatures and therefore are different in every state. All states have visual acuity requirements of varying degrees, and the majority of states have a minimum visual field requirement. The specific driving requirements for a state can be obtained from the state's DMV/DOT website. The vision requirements for driving in Iowa are listed in Table 1, and the vision requirements for many of the neighboring states can be found at (http://www.medicine.uiowa.edu/eye/DrivingwithVisualImpairment/).[1] Unlike some states, Iowa allows an individual to undergo a detailed on-road driving evaluation to demonstrate the competence to drive even if they do not meet the standard visual requirements (see Table 1). This is because a patient with compromised vision but good mental capacity is often a better driver than a patient with 20/20 vision but poor judgment. Interestingly, most studies show minimal or no association between decreased visual acuity and motor vehicle collisions.[3,4] This may be partially because visually impaired drivers tend to drive less and in more familiar surroundings.[5]
An impaired visual field has been demonstrated to be a risk factor for motor vehicle accidents and violation rates.[6] In Iowa, greater than 140 degrees of continuous horizontal binocular or monocular field is required to drive without restrictions. This is determined using the V4e target, which is the brightest and largest stimulus employed in routine Goldmann perimetry. Deficits in the isopters of smaller and dimmer stimuli do compromise a patient's ability to see and drive, but they are not legally limiting. In patients with large deficits in these dimmer isopters, restrictions should be seriously considered despite the legal ability to drive.
The Useful Field of View test (UFOV) was developed to test fitness to drive beyond standard visual field testing measures. UFOV measures higher order visual processing skills such as visual processing speed and selected and divided visual attention skills.[7] Multiple studies have demonstrated that the UFOV test correlates with driving performance.[3,8,9] The UFOV test can help determine if a patient can use their compromised field of vision in a functional manner, which is important in helping guide decisions in driving restrictions. In addition, the UFOV test can identify patients who have a relatively full visual field on traditional visual field testing but a limited functional field due to the inability to attend to simultaneous targets. Unfortunately, the UFOV is currently considered too costly and time consuming to be used for widespread screening.[10]
In some states, it is mandatory for physicians to report patients whose vision loss makes them at high risk for motor vehicle accidents. Even if the physician is not legally required to report patients, one still has a moral and ethical obligation to counsel these patients of their inability to drive to protect the patient and public. This can be a difficult discussion when a patient has 20/20 vision and has been driving without difficulty, but does not meet the criteria to drive due to constricted visual fields. These patients may believe they are seeing their eye doctor for a routine eye examination, only to learn they are no longer visually qualified to drive. The loss of the ability to drive is never taken lightly because driving cessation is associated with a number of adverse consequences, including depression, social isolation, and decreased quality of life.[2,5,11]
Approaching patients in a sensitive manner is critical when telling them they no longer meet the visual requirements to drive. It is best to explain that you are on their side and here to protect them. Some of these patients have been driving safely for many years, and feel this has demonstrated their competence to drive. Using a case in point to demonstrate the personal risks involved may help the patient to understand and accept the restriction. For example, there is no way to prevent the child on a bike that may cross the road without looking or the inexperienced driver from hitting the patient's car. No matter how unavoidable the situation, it could become a legal liability if others discover that the patient is driving with compromised vision, despite not being at fault for the accident.
Some patients are technically legal to drive, but have significantly compromised fields. This is the case for our patient. Often asking such a patient if they feel safe to drive will allow the physician to breach the topic. At times, patients will feel relief when told they should not drive, because they themselves do not feel safe when they are on the road. In other patients, a UFOV test or an on-road driving evaluation can be helpful in determining the capacity to continue to drive safely.
Our patient has Goldmann visual fields that demonstrate that she is legally able to drive in the state of Iowa without restrictions because only the largest isopter, V4e, is taken into account when determining the driving visual field. Her bilateral scotomata of the V4e are in different positions in each eye, which makes her bilateral visual field continuous and full with respect to the V4e. However, she does have fairly large I4e scotomata in both eyes, which do overlap. Thus, some small objects in less than ideal lighting could easily go unnoticed. We reviewed our findings with the patient and recommended limiting her driving. We plan to see her back in clinic where she will undergo a Useful Field of View test in order to better determine her ability to drive safely.
Chen JJ, Wilkinson ME, Stone EM. Driving in the visually impaired: regulation and discussion. EyeRounds.org. Posted January 2, 2013. Available from http://www.EyeRounds.org/cases/161-driving.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links