
Chief Complaint: Enlarging conjunctival/corneal lesion, left eye
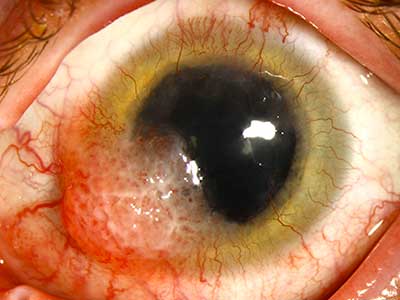
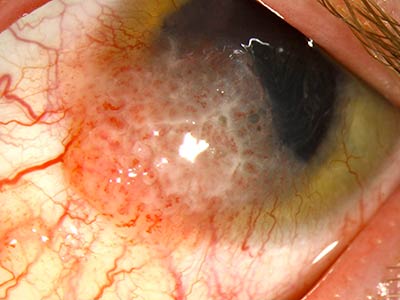
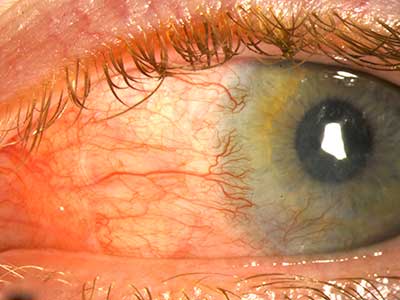
A healthy, 22-year-old Caucasian man presented to the University of Iowa Department of Ophthalmology with concerns of a new, enlarging conjunctival/corneal mass on his left eye. He first noticed the mass 2 to 3 months prior to presentation when he developed redness, irritation, and foreign body sensation. Shortly thereafter, he noticed a small, elevated lesion on his cornea. The lesion has continued to increase in size over these recent months.
The patient first presented to the cornea clinic at age 11 with symptoms of intermittent discomfort and epiphora with 360 degrees of vascular pannus noted on examination on his left cornea. At the time, the pannus was presumed to be secondary to chronic asymmetric meibomian gland dysfunction, but did not improve significantly with doxycycline, topical steroids, topical olopatadine (Patanol), and warm compresses.
In 2002, due to persistent symptoms, he was evaluated at an outside institution where several tests were done, including impression cytology of the cornea, which was negative. When he had resumed care at our institution in 2004, two superficial keratectomies were performed, which showed mild to moderate epithelial dysplasia, most likely reactive in nature rather than neoplastic. No organisms or inflammatory cells were noted on the biopsies, but due to continued concern of possible Acanthamoeba keratitis, the patient was also treated with topical cyclosporine, oral Vitamin C, oral Vitamin A, and chlorhexidine for a short period of time without any clinical improvement. The patient was presumed to have a diffuse epitheliopathy, of uncertain etiology, and possible stem cell deficiency. The patient was subsequently followed locally until the development of the presenting conjunctival/corneal lesion.
None; otherwise healthy
No current medications
Noncontributory
Non-smoker
Negative other than the ocular issues
Visual acuity, with correction:
Pupils: 6mm to 4 mm, brisk reflexes, no RAPD
Intraocular pressure: 18 mmHg both eyes (OU)
Extra-Ocular Motility: Full OU
Anterior Segment Exam:
 |
 |
Dilated fundus exam: Normal OU
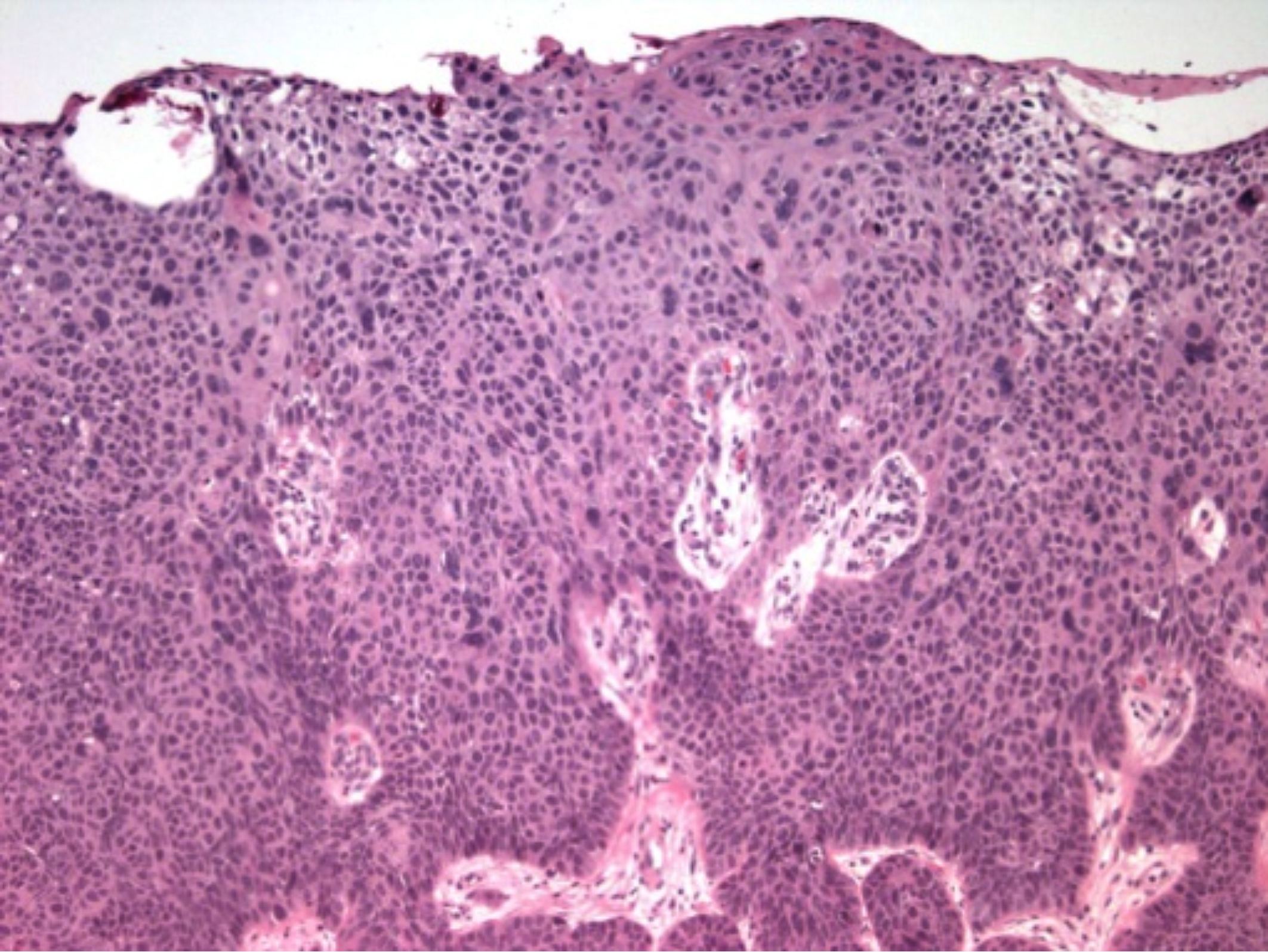
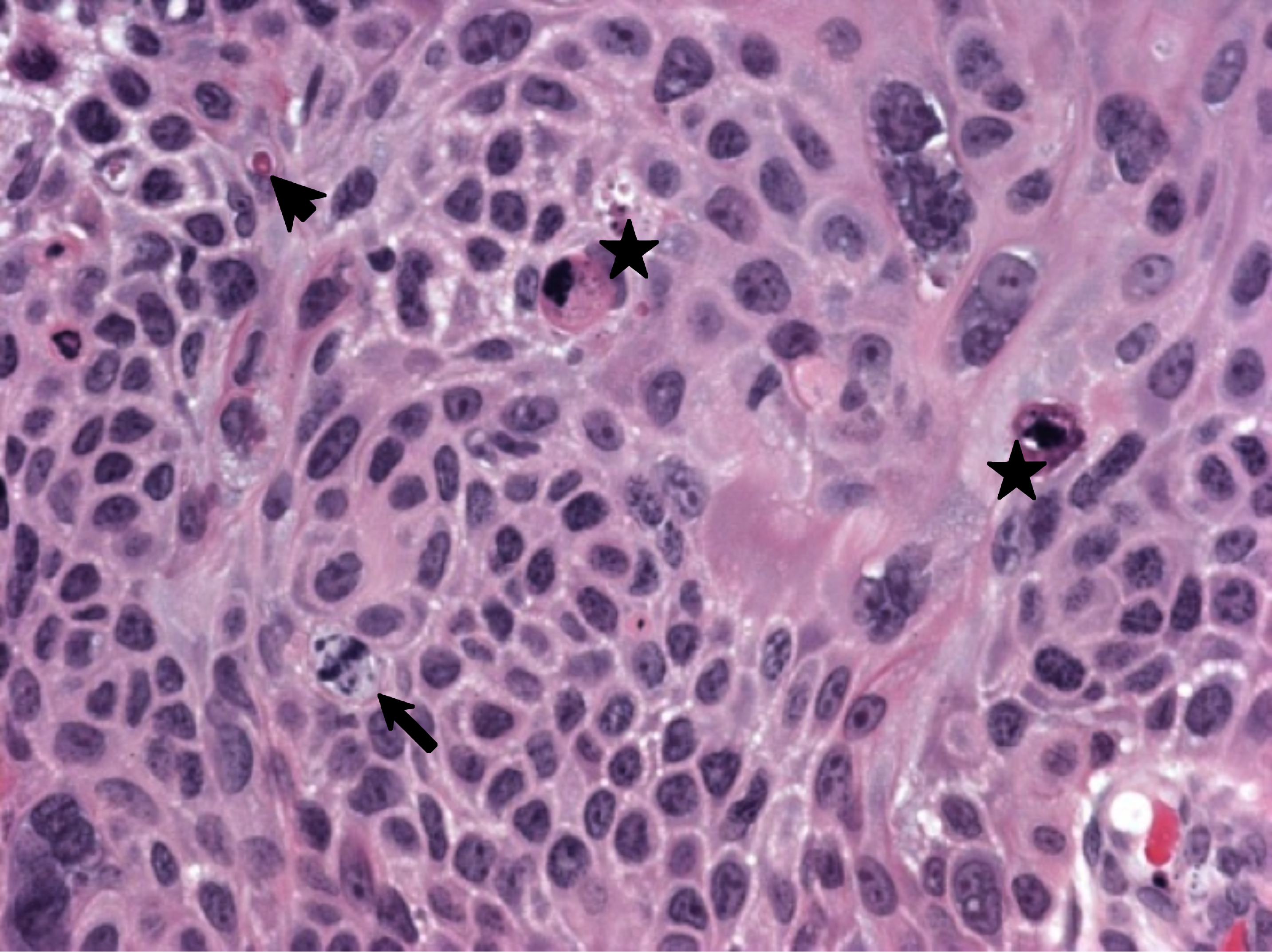
The patient's clinical presentation was very concerning for a squamous cell carcinoma. Testing for HIV was negative. Four weeks after presentation he underwent an excisional biopsy with cryotherapy, intraoperative mitomycin C, absolute alcohol, and an amniotic membrane graft on the left eye. Histopathologic analysis demonstrated invasive squamous cell carcinoma, moderately differentiated, extending into all horizontal and deep surgical margins (Figures 3 & 4).
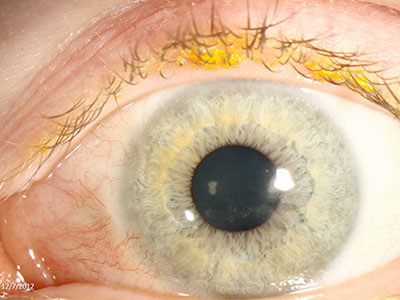
Adjuvant treatment with topical interferon alpha 2B (1 million units/mL) four times per day was started with plans to continue this medication for at least 12 months. In addition, monthly subconjunctival injections of 10 million units of interferon alpha2B were performed for 6 months. At the 4 month postoperative visit, the visual acuity on the left eye with correction was 20/60, pinhole 20/40. Although there was some pannus and conjunctival injection inferonasally, the clinical appearance of the ocular surface was much improved without any evidence of recurrent squamous cell carcinoma (Figures 5 and 6). At the 10 month postoperative visit, the visual acuity on the left eye was 20/25, pinhole 20/20, and there was no clinically visible evidence of squamous cell carcinoma (Figure 7).
 |
 |
 |
 |
 |
Ocular surface tumors are relatively rare with an incidence of 0.13-1.9 per 100,000.[1,2] Ocular surface squamous neoplasia (OSSN) is an umbrella term that encompasses dysplastic lesions involving the squamous epithelium of the conjunctiva or cornea, which includes squamous papilloma, conjunctival-cornea intraepithelial neoplasia (CIN), carcinoma in situ (CIS), and invasive squamous cell carcinoma (SCC). The clinical presentation of OSSN varies across a wide spectrum and is classified by the degree of epithelial and stromal (substantia propria) infiltration. The epithelial infiltration can range from mild to severe dysplasia (i.e. mild, moderate, or severe CIN) to full-thickness epithelial dysplasia (CIS) to invasive SCC, when tumor cells invade through the epithelial basement membrane.[1,3] Fortunately, of these conditions, invasive SCC is the least common.
The highest incidence of OSSN occurs in men between the ages of 50 and 75 years of age.[1,2] Fair skin, pale irises, high propensity to sunburn, and a past history of skin cancer have all proven to be related risk factors.[3,4] Other risk factors for OSSN include: chronic infection by HPV (human papilloma virus), HIV, or trachoma, vitamin A deficiency, xeroderma pigmentosum, chronic irritants, and chronic epitheliopathies.[1,3-5] Immunosuppression, whether due to organ transplantation or secondary to AIDS, is a major risk factor, especially in conjunction with one of the above risk factors.; it is estimated that the risk of conjunctival malignancies increases 13-fold in patients with HIV.[6] The disease also behaves in a much more aggressive manner in patients with AIDS or xeroderma pigmentosa.
An OSSN lesion in a younger patient should raise suspicion for the possibility of underlying immunodeficiency; a study conducted in Miami suggested that as many as half of patients younger than 50 years with OSSN have HIV.[7] In addition to HIV testing, a thorough investigation of other potential sources of immunodeficiency should be performed.
In the particular case presented above, the patient is a very atypical presentation OSSN; the patient is very young, and a thorough investigation revealed that the patient is HIV negative and not immunosuppressed. Even at the age of 22, the patient already had a decade long history of an epitheliopathy. It is possible that the chronic ocular surface irritation put the patient at higher risk for OSSN.
Lesions rarely affect vision prior to presentation, but due to its readily visible location, OSSN is often recognized early. OSSN can involve the conjunctiva or the cornea individually but more commonly involves both.
Over 95% of OSSN cases originate in the limbus, often in the interpalpebral region (i.e. at 3:00 or 9:00 on the bulbar conjunctiva).[8] The reason for the propensity of the lesions to this region is thought to be due to a combination of factors, including the presence of transitional type epithelium, high UV exposure, and a high mitotic rate.[8]
Lesions have been described as varying in appearance with color ranging from a pearly gray to a reddish brown (if pigmented), and surface from papilliform to gelatinous. A white plaque (leukoplakia) may develop on the surface of the lesion, which indicates secondary hyperkeratosis secondary to squamous cell dysfunction, and is concerning for invasive disease. There may or may not be prominent feeder vessels, but unfortunately, their presence does not help narrow the differential.[3] Clinically, symptoms may range from asymptomatic to a chronically irritated, red eye. Masses are initially mobile; the conjunctiva in later stages becoming fixed to the globe with deeper scleral infiltration. Rose Bengal staining can help identify the extent of the lesion.
Through close careful exam with slit-lamp biomicroscopy, OSSN lesions can frequently be distinguished from other conjunctival lesions, such as pterygia and conjunctival lymphoma. However, studies have shown it is very difficult to distinguish between the different types of OSSN; experienced physicians were only able to accurately diagnose OSSN stages 40% of the time.[2] Thus, a tissue specimen is needed for histologic diagnosis to distinguish CIN from invasive SCC.
Due to its malignant seeding potential, it is recommended that an excisional, rather than incisional, biopsy be performed when possible. This includes all smaller tumors (limbal tumors <4 clock hours or <15 mm basal dimension).[8] If the lesion is too large, an incisional biopsy (punch or incisional wedge) to first obtain a histopathologic diagnosis may be necessary before proceeding to more extensive treatment.[8]
In addition to a histological sample, impression cytology has been occasionally used in the diagnosis of OSSN lesions, such as in our patient's early work-up. Despite it's a high positive predictive vale of 97.4%, its negative predicative value is only 52.9%, making it a poor diagnostic tool but valuable as a non-invasive screening technique.[9]
It is not unusual for invasive SCC to invade locally into the sclera, intraocularly, or into the orbit, with one study estimating incidence rates to be 37%, 13% and 11% respectively.[10] In cases where extensive spread is suspected, it is important to assess the extent of the lesion with ultrasound biomicroscopy (to assess scleral or intraocular invasion), gonioscopy (if angle invasion is suspected), or Gadolinium-enhanced MRI scans (to assess orbital extension). Fortunately, even the most aggressive form of OSSN, invasive SCC, usually is not associated with regional or distant metastases, and only a few cases have been reported.[11, 12]
All forms of OSSN tumors are treated aggressively but with markedly different anticipated therapeutic endpoints; the goal of less invasive disease is complete eradication, while the goal of invasive disease is to minimize spread of the disease. Depending on the lesion and histopathologic findings, treatment can range from topical chemotherapy or excision alone for smaller lesions versus a combination of surgical excision, cryotherapy, and chemotherapy for larger or invasive. Rarely, radiotherapy, and in extreme cases, enucleation and even exenteration, may be necessary.[3,8,13]
A 2 to 4 mm margin beyond clinically evident disease is performed. Intraoperative, cryotherapy can be applied to the edge of the excision to freeze any residual viable cells. During the procedure, mitomycin C (0.2 mg/mL or 0.4 mg/mL) can be applied topically for 1-2 minutes. If the lesion extends onto the cornea, absolute alcohol can be used to remove the involved corneal epithelium. Copious irrigation needs to be performed following the application of mitomycin C or absolute alcohol. After removal of larger tumors, conjunctival autografts or amniotic membrane grafts can be used to help close the conjunctival defect.[8, 13]
Chemotherapy has become the mainstay to adjunctive treatment with surgical excision, and has shown to be very effective. This is typically accomplished through topical eyedrops of mitomycin C, 5-fluorouracil, or interferon alpha 2B. Mitomycin C drops are typically prescribed four times per day for 1-3 weeks, followed by 1-3 weeks of no drops to allow for ocular surface recovery. This cycle is repeated 2 to 4 times depending on the clinical response.[8] Side effects from topical chemotherapy include dry eye, superficial punctate epitheliopathy, punctual stenosis, and rarely stem cell deficiency. Punctal occlusion with punctal plugs is recommended prior to starting these regimens to prevent punctal stenosis.[3,8,13]
A general mechanism of each of the main chemotherapeutic agents is outlined below.
There are two types of radiation therapy employed: external beam radiotherapy and custom-designed plaque radiotherapy. Radiotherapy alone or accompanying enucleation is reserved for particularly severe and wide-spread cases where the extent of the lesion precludes excision.[8]
Many cases of invasive SCC are treated successfully with excisional biopsy combined with adjuvant topical chemotherapy and generally carry a favorable prognosis. Caution must be taken to evaluate for spread of disease. Invasive SCC can invade the scleral wall and infiltrate other tissues of the globe or spread into the orbit. Intraocular spread is typically treated with enucleation and orbital involvement with exenteration.
Recurrence of any form of OSSN is possible, with an overall recurrence rate of 12.9%.[20] Tumor recurrence is largely predicted by the size (>5mm in diameter), stage, and histologic diagnosis of the tumor at the time of presentation; none of the tumors defined histologically as dysplasia recurred, while 12.8% of CIS tumors and 22.2% of SCC showed recurrance.[20]
Epidemiology
|
SignsMass originating from the limbus with the following characteristics:
|
Symptoms
|
Treatment
|
Boese E, Rogers GM, Kitzmann AS. A Very Unusual Case of Ocular Surface Squamous Neoplasia. EyeRounds.org. February 14, 2013; Available from: https://eyerounds.org/cases/163-OSSN.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
