Photophobia
A 23-year-Caucasian male presents with bilateral photophobia, foreign body sensation, and tearing that is worse in the left eye. He reports a decade-long history of similar relapsing and remitting symptoms in both eyes, although not necessarily at the same time. The episodes are associated with minimal or no redness and without discharge. There are no exacerbating or alleviating factors. He does not use contact lenses. These episodes have always responded well to topical steroids or cyclosporine drops.
Negative with the exception of the present illness
Non-contributory
Non-contributory
Non-contributory
Right eye (OD): 20/20
Left eye (OS): 20/20
OD: 14 mmHg
OS: 13 mmHg
OD: 615 microns
OS: 609 microns
No injection or discharge
Lids/Lashes: Mild meibomian gland inspissation
Conjunctiva: White and quiet; 1+ upper tarsal conjunctival papilla; no follicles
Cornea: Clear and compact; good pre-corneal tear film with normal break-up time; no fluorescein staining
Anterior Chamber: Deep and quiet
Iris: Normal architecture
Lens: Clear
Vitreous Normal
Lids/Lashes: Mild meibomian gland inspissation
Conjunctiva: White and quiet; 1+ upper tarsal conjunctiva papilla; no follicles
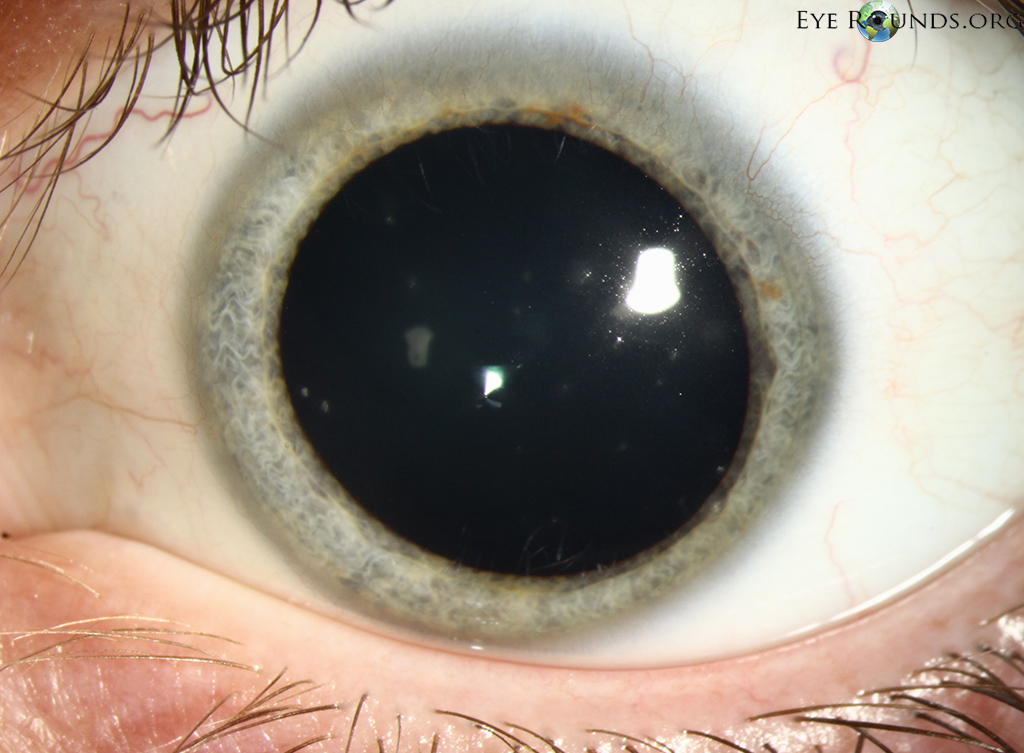
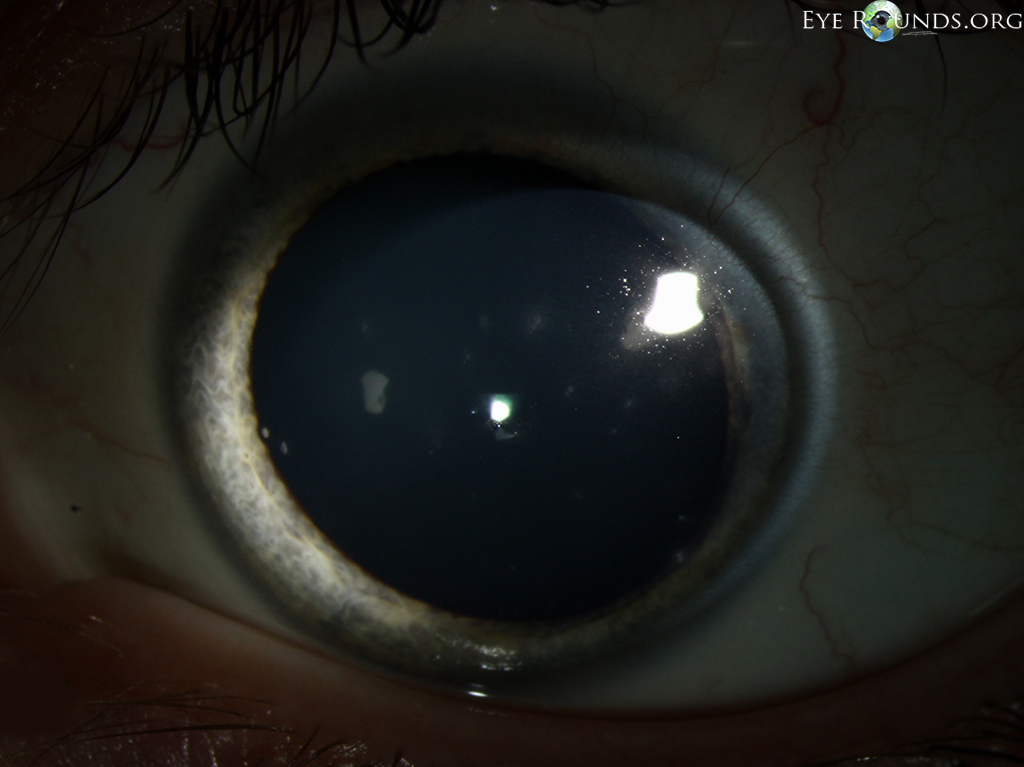
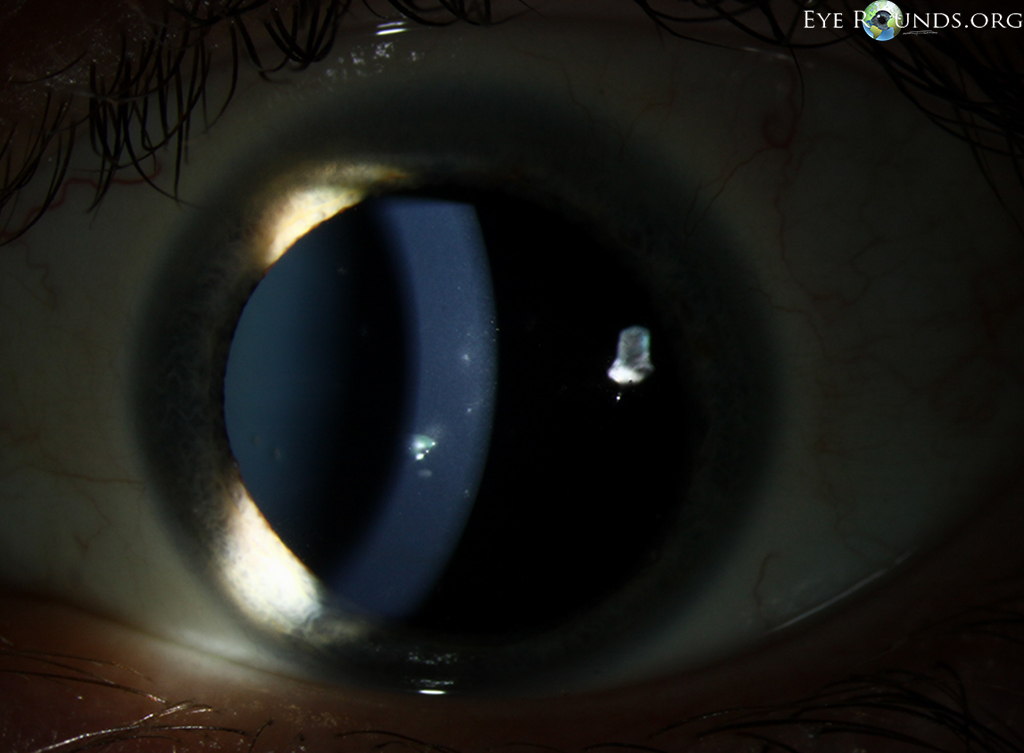
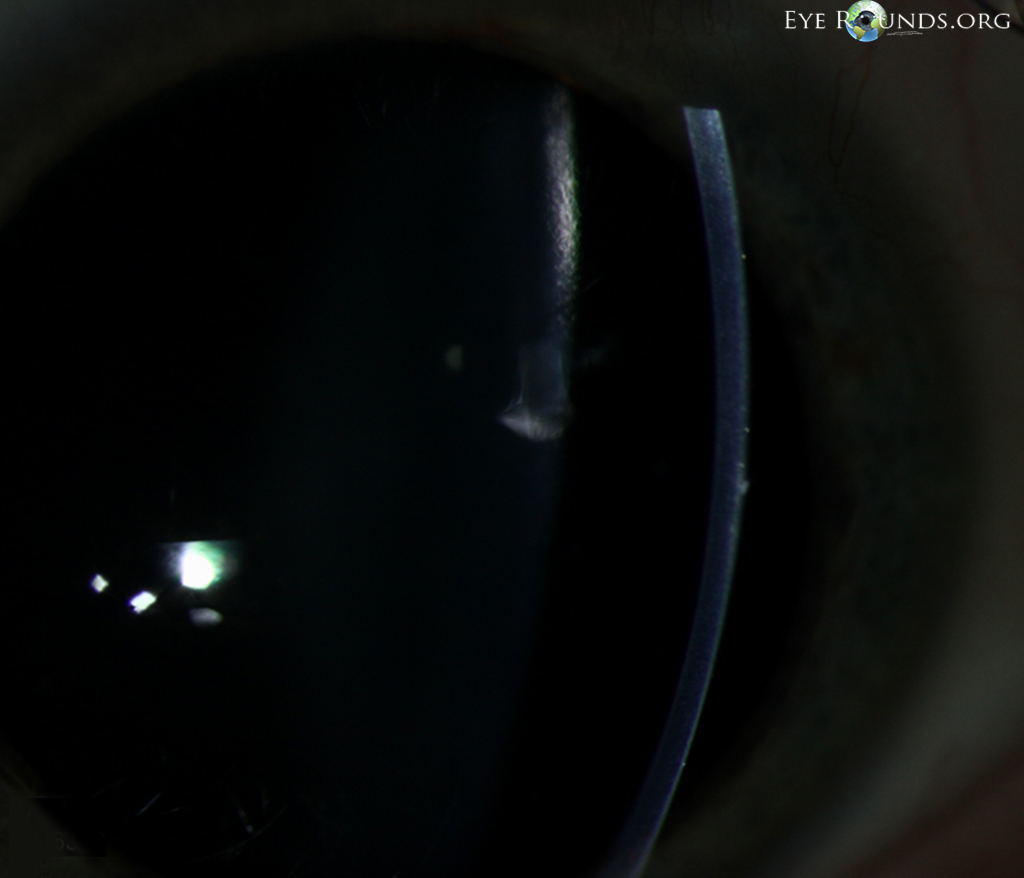
Cornea: Multiple, small stellate intraepithelial opacities in a paraxial distribution without fluorescein staining (Figure 1a-d); good pre-corneal tear film with normal tear film break-up time; no fluorescein staining in areas without opacities; clear and compact stroma
Anterior Chamber: Deep and quiet
Iris: Normal architecture
Vitreous: Normal
Normal, both eyes
Figure 1
|
|
| a | b |
|
|
| c | d |
This patient was treated with bandage soft contact lens therapy for symptomatic relief. He responded well to the introduction of topical loteprednol 0.5% four times daily (QID), followed by a slow taper that was facilitated by the introduction of cyclosporine 0.12%. It has not been possible to completely discontinue topical steroids or cyclosporine due to recurrent disease.
In 1950, Dr. Phillips Thygeson described 26 patients with a distinctive, relapsing and remitting type of superficial punctate keratitis (SPK) (1). This disorder carries his name to distinguish it from several other forms of keratitis with distinctly different clinical appearances and courses.
The condition is considered to be idiopathic, although various reports have linked it to preceding viral keratitis (2-4). There is an HLA DR3 association (5).
Thygeson's SPK typically presents in patients aged 20-30, with an equal prevalence between men and women (2). Most cases are bilateral, but the presentation is usually asymmetric. The condition relapses and remits and tends to have a prolonged course of one to two decades, although duration as long as 40 years has been reported (3).
The prototypical symptom of Thygeson's SPK is photophobia. Patients may also experience mild blurring of vision, foreign body sensation, and tearing. Redness is characteristically absent or minimal. There is no discharge.
The clinical appearance of Thygeson's SPK is pathognomonic. There are multiple (usually 5 to 30), small, white-to-gray, oval-to-stellate, granular-to-breadcrumb-like, corneal intraepithelial opacities that usually occur in a paraxial distribution. Direct involvement of visual axis occurs less commonly, with a commensurate mild decrease in vision (usually in the 20/25 to 20/30 range). Peripheral involvement is rare, but has been reported. The most superficial intraepithelial lesions may stain with fluorescein and be associated with mild discomfort. There are no subepithelial or stromal opacities or stromal ulceration or edema associated with this condition.
For more than a half-century, topical corticosteroids have been the treatment of choice for Thygeson's SPK. Generally complete, prompt (within 1 to 3 days) induction of remission and relief of symptoms can be achieved with initiation of a course of low dose topical steroids (typically never more than prednisolone acetate 1.0%, or its equivalent, twice daily). Resolution of the intraepithelial opacities is invariably associated with a return to baseline vision. Next, it is possible to maintain remission with a relatively rapid (within 2 to 4 weeks) taper to prednisolone acetate 0.12%, or its equivalent, twice daily. To prevent recurrences that often occur in conjunction with attempts at complete steroid cessation (6), an ultra-slow (3-12 months) taper is recommended to a final maintenance (or point of discontinuation) dose of prednisolone acetate 0.12%, or its equivalent, once weekly. At this point, the choice can be made to continue this dosage and frequency indefinitely, or to attempt to discontinue treatment completely. In some cases, this therapeutic maneuver may be associated with recurrent disease.
Topical cyclosporine (7) and, more recently, tacrolimus (8) have been found to be effective steroid-sparing agents in the treatment of this disorder. Traditionally, compounded cyclosporine 2% in peanut oil was used, although recent anecdotal experience suggests that equal efficacy can be achieved with commercially available cyclosporine 0.05% (Restasis®). Tacrolimus is used as a 0.03% eye ointment that is instilled in the inferior fornix. When used at the outset, these agents are slower in inducing remission and relief of symptoms. Like steroids, both agents required prolonged use to maintain remission. A pragmatic approach may be to initially treat episodes with steroids at the outset and substitute steroid-sparing agents during the slow taper phase. The use of steroid-sparing agents may increase, but not guarantee, the likelihood of being able to complete taper off steroids without the development of a recurrence.
Bandage soft contact lenses can be used for temporary symptomatic relief, especially if the relatively slower-acting steroid sparing agents are used as initial therapy. Epithelial debridement provides only temporary remission. Topical antiviral agents, although they have been used, are minimally effective.
Epidemiology
|
Signs
|
Symptoms
|
Treatment
|
Chung A, Lenci, LT, Wagoner MD. Thygeson's Superficial Punctate Keratitis. EyeRounds.org. posted Oct 21, 2015; Available from: https://eyerounds.org/cases/223-Thygesons-SPK.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links