
Blurry vision, right eye
A 39-year-old male with a history of uncharacterized syndromic pigmentary retinopathy, optic atrophy, childhood cataracts, and multiple ocular surgeries was referred for blurred vision and persistent corneal edema in the right eye for the past three to four months.
In his early 20s, he underwent cataract extraction with intraocular lens (CEIOL) implantation in both eyes followed by Nd:YAG laser capsulotomies. He had good vision (~20/60) for many years until the IOL in the right eye dislocated. He underwent pars-plana vitrectomy (PPV), IOL explantation, and scleral-fixation of a secondary IOL (SS-IOL) approximately 4 months prior to presentation. Since that time, he had noted blurred vision and was found to have corneal edema on follow up exams. He denied any pain, fluctuation in symptoms throughout the day, or any improvement in vision with sodium chloride 5% ophthalmic solution (Muro128).
Sodium chloride 5% ophthalmic solution (Muro128) three times daily, both eyes
Non-contributory
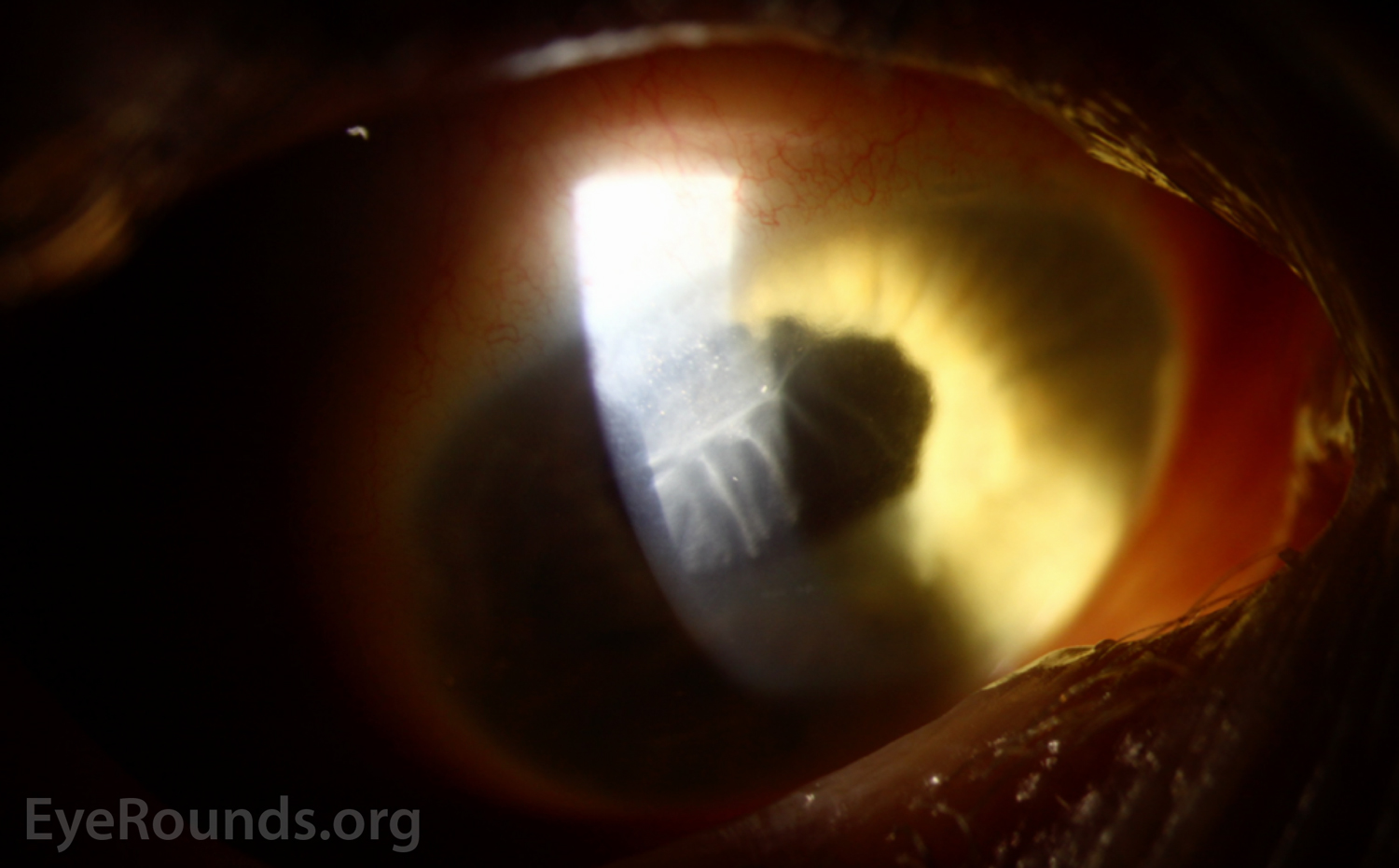
Figure 1: Color slit lamp photograph (broad beam) of the right eye demonstrating a grey sheet with scalloped edges extending along the endothelium with overlying mild corneal edema.
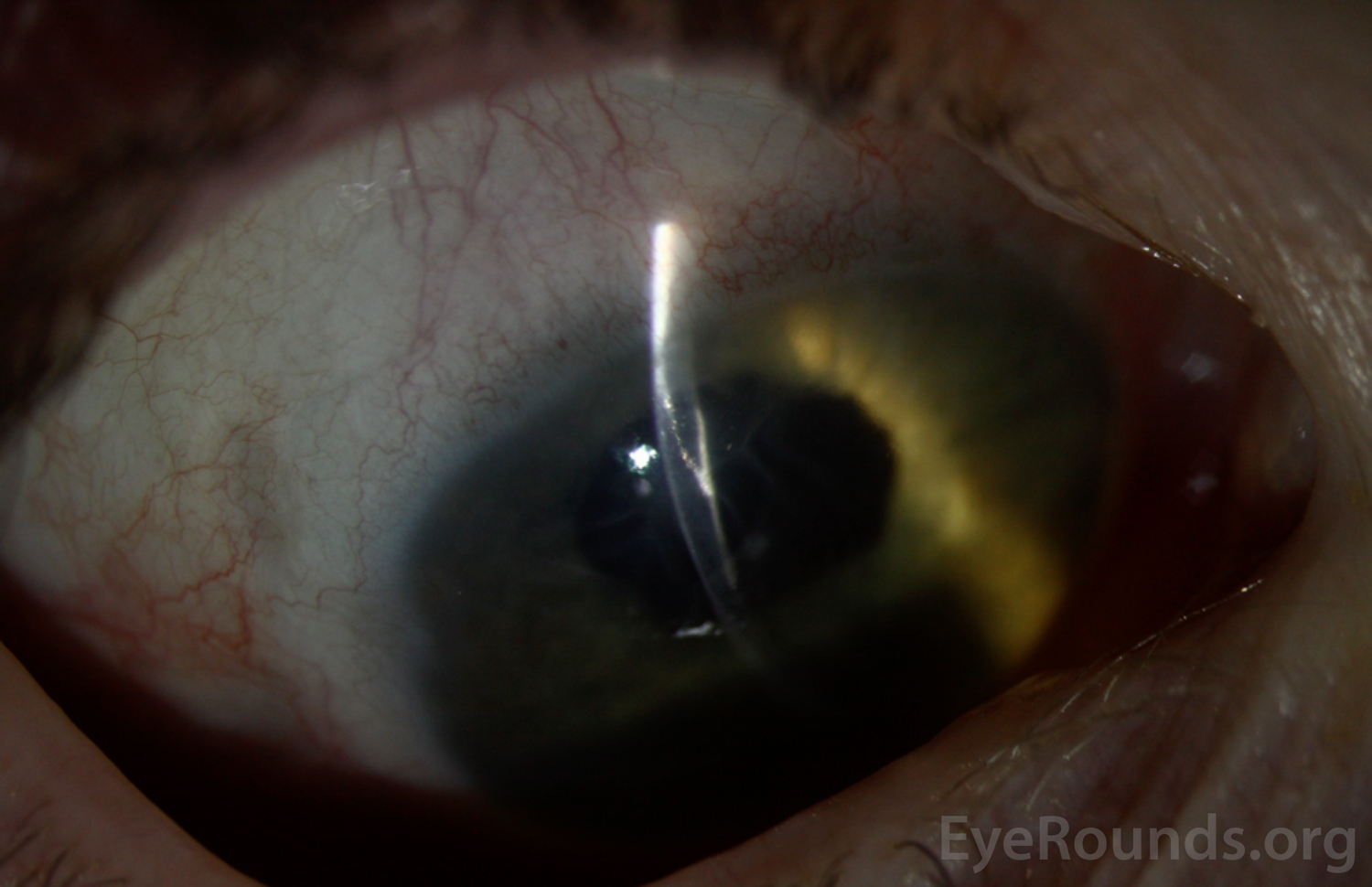
Figure 2: Color slit lamp photograph (narrow beam) of the right eye demonstrating hyperreflective cells extending along the clear corneal incision site.
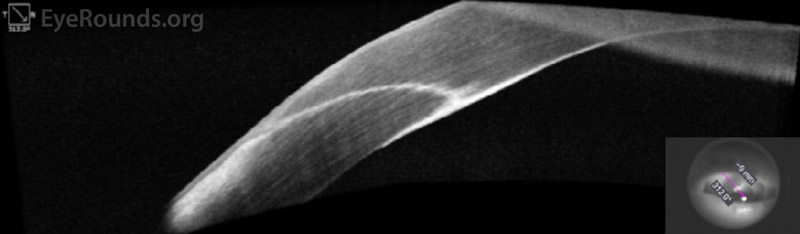
Figure 3: Anterior segment optical coherence tomography (AS-OCT) of the right eye demonstrating a hyperreflective sheet extending through the previous surgical incision and spreading across the endothelium.
The patient's history of numerous ocular surgeries coupled with the exam findings support a diagnosis of epithelial downgrowth. Management options, including careful surveillance, intracameral 5-fluorouracil (5-FU), cryotherapy, membrane peel, excision, and endothelial keratoplasty, were discussed with the patient.
The degree of blurred vision (20/800) was felt to be out of proportion to the corneal findings. The corneal edema was confined to the superotemporal quadrant and minimally involved the central visual axis. Central pachymetry was thickened but comparable to the contralateral eye. It was thought the patient may have thick corneas at baseline related to his congenital ocular syndrome. Thus, the decision was made to proceed with careful surveillance while continuing Muro128.
Epithelial downgrowth
Epithelial downgrowth is a rare but potentially devastating complication that can occur following any intraocular surgery or penetrating ocular trauma. The proliferation of epithelial cells within the eye can lead to endothelial decompensation, recalcitrant glaucoma, and severe vision loss. Treatment is variable and, unfortunately, often ineffective.
The first reported case of epithelial invasion into the anterior chamber following a perforating eye injury was in 1832. During this era, epithelial downgrowth was cited as the cause of up to a quarter of all enucleations after cataract surgery.[1] Advances in surgical technique, including improved corneal wound construction, have greatly reduced the incidence of this vision-threatening complication.[1 ,2] The most recently cited incidence of epithelial downgrowth following cataract surgery was 0.076 - 0.12% at Massachusetts Eye and Ear Hospital over the years 1953 – 1983.[1] Common risk factors are cataract surgery, penetrating trauma, and penetrating keratoplasty. Epithelial downgrowth most often presents within the first year of the inciting event, but has been reported to occur up to 10 years post-operatively or post-trauma.[3]
Epithelial invasion occurs when non-keratinized squamous epithelial cells from the conjunctiva or cornea migrate through a surgical or traumatic corneal wound. This can occur either at the time of surgery or trauma, or secondarily through an incompetent wound or fistula. Additional risk factors include repeated ocular procedures,[4] vascularized corneal stroma, and damaged endothelium, which may predispose to epithelial migration due to loss of normal contact inhibition.[5]
Commonly, the proliferating cells take on the form of a retrocorneal sheet. Other less common presentations include cysts or free-floating cells.
Patients classically present with painless decrease in vision, but redness, pain, tearing, and photophobia are also common.[1] Slit-lamp exam usually demonstrates a retrocorneal translucent or grey membrane extending from a prior surgical or traumatic wound. Careful gonioscopy and dilated exam should be performed to assess for epithelial growth in the iridocorneal angle or posterior pole, respectively.
The degree of ocular morbidity depends on which structures are affected. These may include the corneal endothelium (with subsequent corneal edema), iridocorneal angle (leading to obstruction of the trabecular meshwork), iris (with distortion or irregularity of the iris stroma), crystalline lens (cataract) or artificial intraocular lens (sheet), vitreous body (free-floating cells) and retina.[6] With the growing popularity of endothelial keratoplasty (EK) procedures, epithelial cells can also be found within the EK-stroma interface.
Secondary complications include chronic inflammation, corneal decompensation, pupillary block, secondary glaucoma, tractional retinal detachment, phthisis bulbi, and permanent loss of vision.[1 ,7]
Anterior segment OCT may demonstrate a hyperreflective sheet extending from a previous surgical or traumatic wound. Corneal confocal microscopy will reveal round, nucleated epithelial cells displacing normal hexagonal endothelial cells.[8] If the epithelial sheet involves the iris stroma, laser photocoagulation will confirm the diagnosis by causing the sheet of abnormal cells to blanch,[9 ,10] compared to laser burns to uninvolved iris which turn dark brown or black. Aqueous aspiration with subsequent cytologic examination can assess for the presence of free-floating epithelial cells.[11]
Proliferating epithelial cells are difficult to remove and often recur despite aggressive treatment. Sheet-like growth, the most common presentation, has the worst prognosis due to difficulty identifying the borders of the lesion and the destructive nature of the surgical procedures required to excise it. In the late 1960s, Maumenee et al found that 27.5% of eyes surgically treated for epithelial downgrowth had vision of 20/50 or better.[12] In a clinicopathological review of 124 patients with epithelial downgrowth from 1953-1983, 50% of patients treated surgically eventually lost vision, required enucleation, or had phthisis bulbi.[1] More recent techniques may lead to improved outcomes.
Treatment depends on the location and extent of involvement. Localized epithelial cells can be devitalized using transcorneal cryotherapy or laser photocoagulation.[13] A confined retrocorneal membrane may be surgically scraped off. However, more extensive involvement may require en-bloc surgical excision of all compromised tissue.[14] In addition, care must be taken not to seed epithelial cells further. For instance, in the case of epithelial cells within an EK graft-stromal interface, complete removal with a penetrating keratoplasty, as opposed to repeat EK, is recommended.[15]
In an effort to reduce surgical destruction of tissue, physicians have started treating epithelial downgrowth with intracameral 5-fluorouracil (5-FU),[3 ,16] which is a pyrimidine-analog antimetabolite. 5-FU selectively inhibits rapidly dividing cells. It has other ophthalmic applications including topical treatment for ocular surface squamous neoplasia and prevention of fibrosis after trabeculectomies. Various methods have been employed to concentrate delivery of the medication intracamerally for treatment of epithelial downgrowth, including mixing 5-FU with viscoelastic followed by with face-down positioning by the patient.[17]
Management of the cyst form of epithelial downgrowth has a higher success rate. Cystic lesions are easily identifiable and the implanted cells are circumscribed within the cyst. Various techniques have been described, such as aspiration of the cyst, intra-cystic irrigation with a sclerosing agent such as absolute alcohol, and surgical excision of the cyst including its stalk.[18-20]
Whatever the treatment modality chosen, careful surveillance is required to identify any recurrence of these aggressively replicating cells.
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
Colwell L, Diel RJ, Benage M, Jiang L, Greiner MA, Ling JJ. Epithelial Downgrowth. EyeRounds.org. Posted February 24, 2020; Available from https://EyeRounds.org/cases/292-epithelial-downgrowth.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
