
INITIAL PRESENTATION
Chief Complaint: Bilateral white cataracts in a patient with untreated diabetes
History of Present Illness:
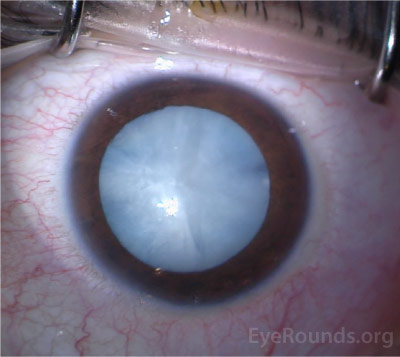
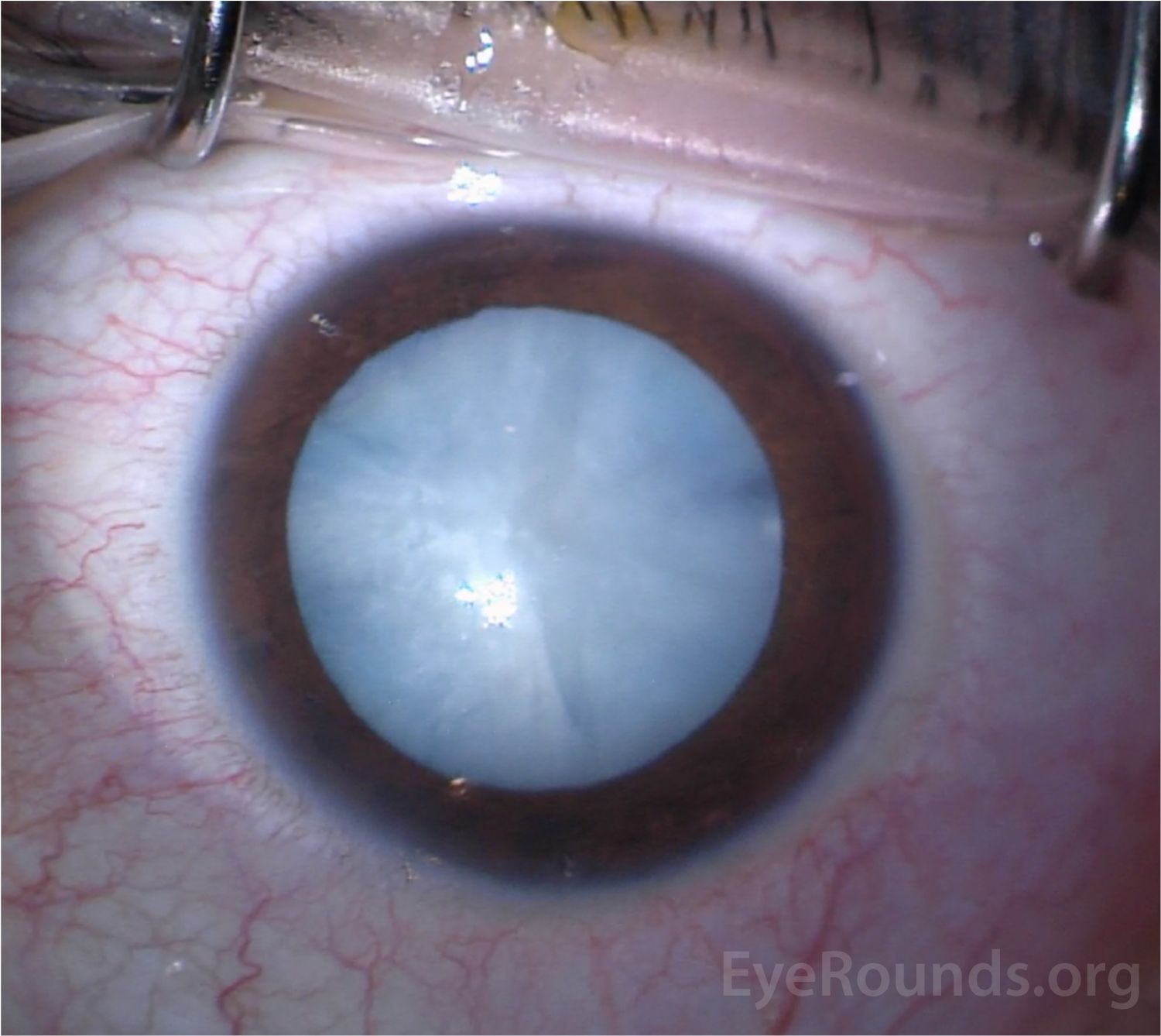
A 21-year-old gentleman was referred from a prison medical center for evaluation of bilateral white cataracts. He was diagnosed with type 1 diabetes mellitus at age 17 and reported “going blind” at age 18. He stated that he could only see lights and shadows. He had been using insulin (detemir and regular) intermittently since diagnosis for glucose management. The patient otherwise denied a history of congenital cataracts or metabolic disorders.
Past Ocular History:
Past Medical History:
Medications:
Allergies: No known Allergies
Family History: : Non-contributory; denies family history of congenital cataracts or metabolic disorders
Social History:
Review of Systems: Otherwise negative
OCULAR EXAMINATION
A-scan echography:
| 25.41mm | 25.20mm | |
| 3.90mm | 3.33mm | |
| Lens thickness | 5.90mm | 4.54mm |
Differential diagnosis of white cataract in young patient:
DIAGNOSIS: White cataract secondary to diabetes mellitus
CLINICAL COURSE
Ocular findings were consistent with bilateral white cataracts, most likely due to uncontrolled type 1 diabetes mellitus. Alternative etiologies in a patient this age include congenital cataract or metabolic disturbance such as galactosemia, but these are less likely given the relatively recent onset of symptoms, the lack of nystagmus (which might indicate deprivation amblyopia), and the history of poor diabetic control. Additionally, the patient had no history of significant trauma to the eyes and/or orbits to result in a traumatic cataract.
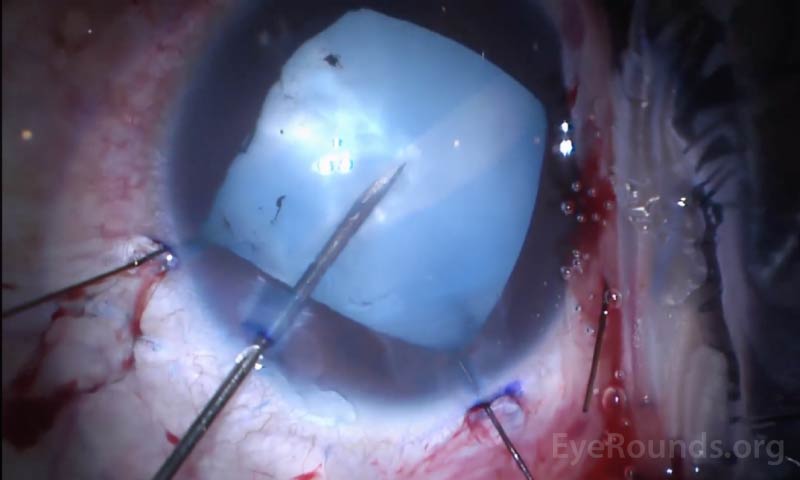
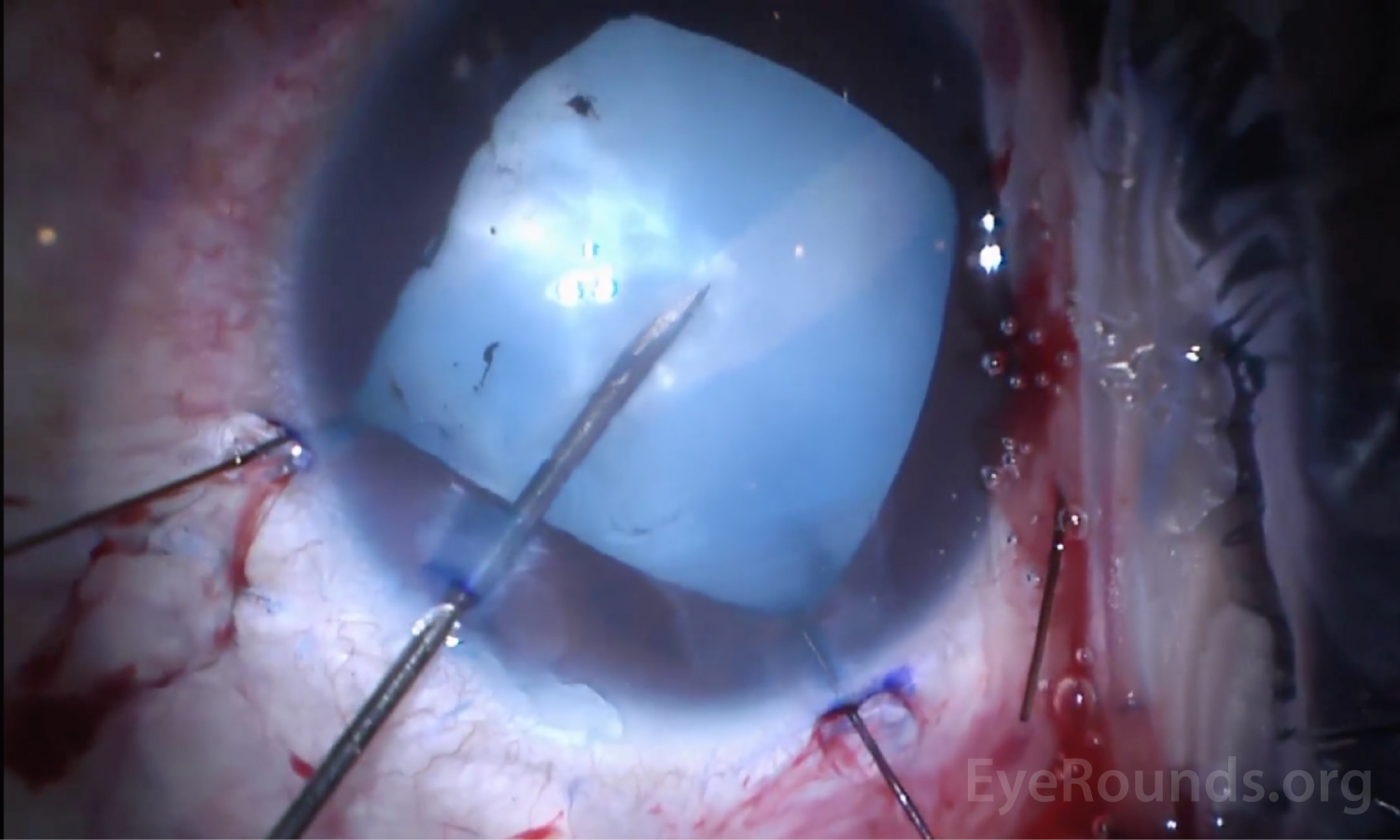
The decision was made to proceed with cataract extraction with intraocular lens placement under retrobulbar block in the right and then left eye. At the time of surgery, trypan blue was injected to stain the anterior lens capsule, thus allowing for improved capsule visualization. The anterior capsular tear was initiated with a 27-gauge needle on a syringe to simultaneously decompress the capsular bag. In the right eye, a capsular tension ring was placed due to diffuse zonulopathy, attributed to the maturity of the cataract. A continuous curvilinear capsulorhexis was then performed successfully, and the cataract was removed without complication (Video 1). In the left eye, the capsulorhexis radialized, but the margins were recovered with the use of microscissors and micrograspers (Video 2). The cataract was then removed using standard techniques. Both eyes had good post-operative appearances, with improvement in acuity to 20/20 OD and 20/20-2 OS after manifest refraction. The fundus exam was performed at the postoperative day 30 visit and there was no evidence of diabetic retinopathy in either eye. .
DISCUSSION
In this section, we will discuss the pathophysiology and management strategies for performing surgery on a white cataract. Although these strategies apply to a white cataract of any cause, we will focus specifically on the diabetic white cataract.
Clinical Features and Pathophysiology:
Cataracts are a well-known consequence of untreated diabetes mellitus, and a common cause of visual impairment. Cataracts are 3-4 times more common in young diabetic patients compared to their non-diabetic counterparts [1]. While several mechanisms have been proposed to explain the earlier and more rapid onset of cataracts in diabetic patients, the primary risk factors include poor glycemic control and longer duration of disease [2]. In younger patients with early or mild cataracts, good glycemic control may allow for reversal in cataract severity, although this is not the case for older adults or patients with mature cataracts [3].
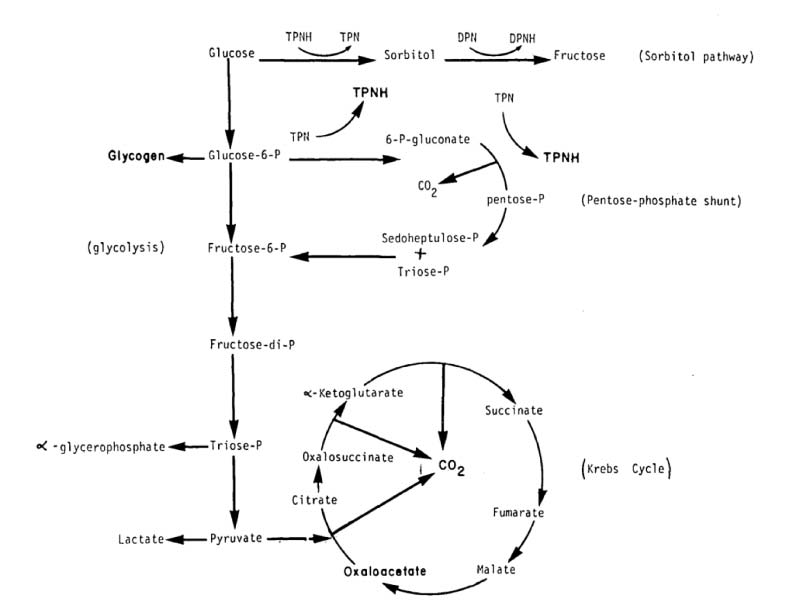
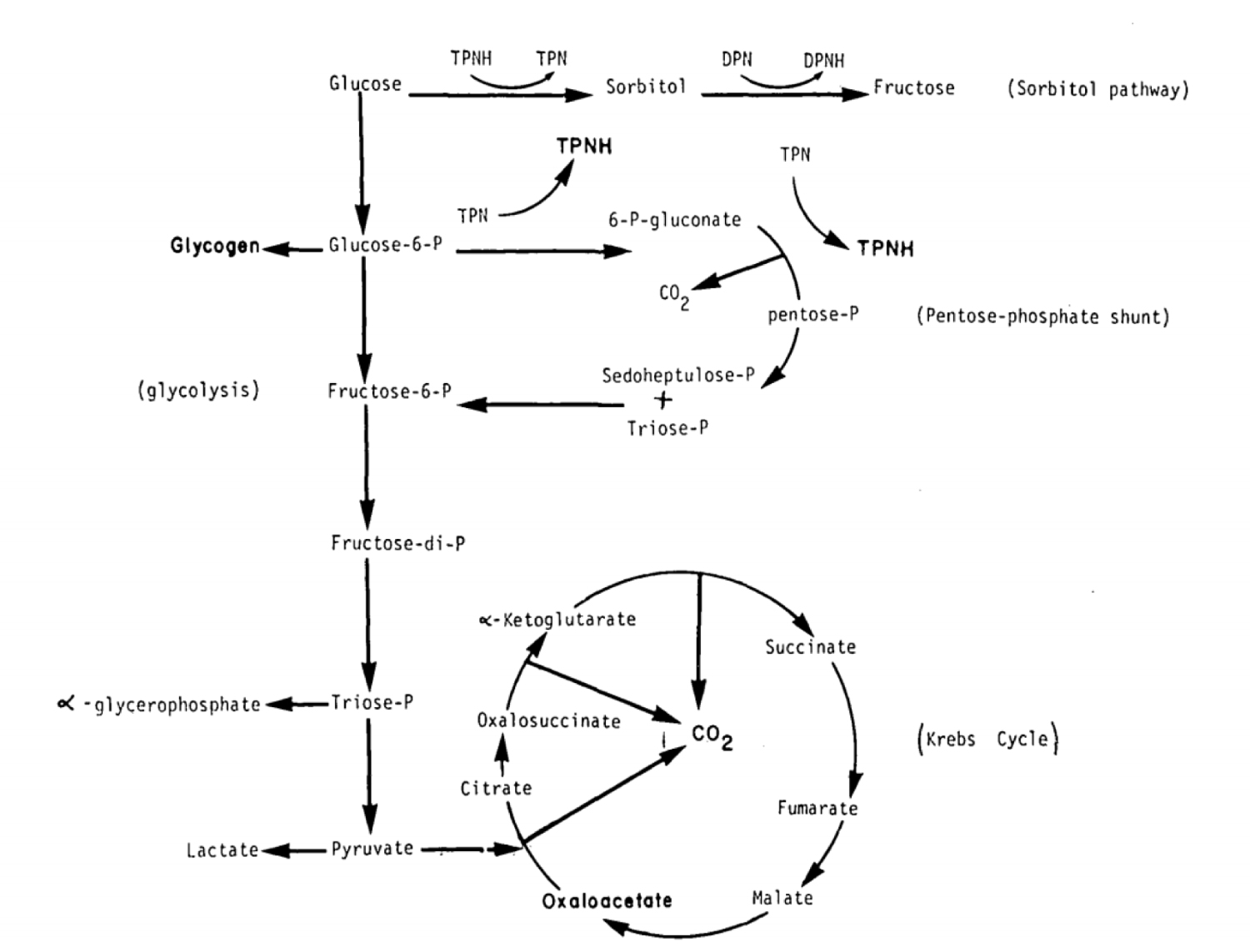
The activation of the polyol (sorbitol) pathway of intralenticular glucose metabolism in chronic states of hyperglycemia is thought to play a crucial role in the development of the diabetic cataract [4-5]. In a typical, non-diabetic physiologic environment, glucose is present in the aqueous humor and is metabolized by the lens primarily through anaerobic glycolysis, owing to the low oxygen tension in the aqueous. In this pathway, cells of the crystalline lens rely on the enzyme hexokinase to phosphorylate glucose (G6P) and retain this molecule within the intracellular compartment (Figure 2) [7].
The hexose monophosphate (HMP) shunt is an auxiliary, parallel pathway in which glucose is metabolized under normal conditions for maintaining lens clarity (Figure 2). While these parallel pathways are efficient under typical physiologic conditions, they are not adequate in hyperglycemic states, such as in type 1 diabetes mellitus. Under these conditions, excess glucose overwhelms the traditional pathways and thus is shunted towards the polyol, or sorbitol, pathway within the lens (Figure 2). Glucose in this pathway is converted to sorbitol by aldose reductase, and subsequently to fructose by polyol dehydrogenase.
Eventually, retained sorbitol and fructose increases the osmotic pressure within the lens, causing lens fiber swelling and opacification [4-6], both contributing to the development of a white cataract. Longstanding hyperglycemia may lead to the formation of a hypermature cataract, hallmarked by the degeneration of cortical material into a hyperosmotic liquid. This further draws in surrounding fluid and creates a tense capsule with a free-floating nucleus. Additional contributory mechanisms include formation of hydroxyl and nitric oxide free radicals within the lens due to osmotic stress on the endoplasmic reticulum [5].
These metabolic disturbances of untreated type 1 diabetes can affect the crystalline lens in a myriad of ways, including reducing lens clarity, altering the refractive index, and impairing accommodation. Diabetic cataracts typically begin with diffuse subcapsular changes with subsequent vacuole and cleft formation in the adjacent cortex. Maturation into a dense, white, possibly intumescent cataract typically can occur with longstanding poor glycemic control. These changes are observed at earlier ages in diabetic patients compared to non-diabetic patients [4]. Acute myopic or hyperopic shifts may precede evidence of cataract formation in patients with undiagnosed or recently uncontrolled diabetes. See https://webeye.ophth.uiowa.edu/eyeforum/cases/295-refractive-changes-in-diabetes.htm for further explanation of the pathophysiology of these refractive shifts. Of note, similar pathways of metabolic shunting occur in the formation of a type 2 diabetic cataract.
Treatment and Surgical Considerations:
When the diabetic cataract has become visually significant, cataract extraction with placement of an intraocular lens is indicated. However, special surgical considerations must be made in the case of white cataracts, as detailed below.
A lack of red reflex through a white cataract adds difficulty in visualizing the anterior lens capsule and thus in the creation of the continuous curvilinear capsulorhexis. For this patient, the anterior capsule was stained with trypan blue to allow for adequate visualization during capsulorhexis formation, as has been recommended previously [8]. Utilization of an anterior capsular dye was first described by Hoffer and McFarland in 1993 with the use of fluorescein [9]. Since then, both trypan blue and indocyanine green have been documented as safe methods to enhance intraoperative visualization of the anterior capsule [10]. Jacob et al. report high success with trypan blue as an adjunct for safe phacoemulsification in eyes with white cataracts, reporting that just 3.85% of cases required conversion to a conventional extraction due to loss of the capsulorhexis [11]. Further, Chung et al. demonstrated that eyes that underwent mature cataract extraction with use of either indocyanine green or trypan blue did not experience longer phacoemulsification time or significant loss of endothelial cell count compared to their control counterparts [12].
Further complicating matters, the swollen lenticular material created by the osmotic shifts of hyperglycemia can cause the capsule to become tense and pressurized. To achieve a controlled entry into the anterior capsule and facilitate in decompression of the capsular bag, a central incision in the capsule with a 27-gauge needle, as shown in Video 1, may benefit the surgeon. In this case, no fluid emanated from the nucleus, indicating that it was safe to extend the capsular tear without significant risk of extension under pressure. In a case where liquified material does exit the capsule, immediate aspiration and gentle depression of the lens is recommended in order to decompress the capsular bag [13].
When operating on a pressurized lens capsule, including in white cataracts with variable quantities of liquified cortex, careful initiation of the capsular tear is prudent to prevent an uncontrolled radial splitting of the capsule to the equator, as is seen in the “Argentinian flag sign” [14] (Figure 3). Should the capsulorhexis radialize, the “Little technique” [15] may be used. After filling the anterior chamber with an ophthalmic viscosurgical device (OVD) and lying the capsule flap flat against the cortex, the tractional force applied to the free capsule flap is reversed to redirect centrally. The tear can be advanced by gripping the free edge of capsule close to its root and pulling backwards and along the circumferential path, with consistent horizontal traction used throughout. In some cases, a second paracentesis may be necessary to allow for adequate positioning and angle of approach. See http://webeye.ophth.uiowa.edu/eyeforum/atlas-video/Little-rescue.htm for further explanation.
Additional considerations include using phaco-chop or miLoop to limit usage of excessive phacoemulsification energy in dense cataracts. Zonulopathy occurs more frequently with higher density white cataracts [16], and the use of capsular tension hooks or capsular tension rings may be warranted to provide adequate stability of the capsular bag [17]. Finally, parasympathetic neuropathy may hinder adequate pupillary dilation. This may require a Malyugin ring or iris hooks to maintain visualization and access to the lens capsule [8].
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
References
Silverman J. I.M., Stiff HA, Fortenbach CR, Oetting TA. Diabetic White Cataract. EyeRounds.org. Posted September 23, 2020. Available from http://www.EyeRounds.org/cases/304-Diabetic_White_Cataract.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links

{kind=link}
{kind=link}
{kind=link}