
INITIAL PRESENTATION
Chief Complaint: Right retroorbital pain radiating to the jaw
History of Present Illness:
A 61-year-old male presented to the ED with a 3 to 4 day history of pain behind the right eye. He described the pain as constant and dull with radiation to the jaw. He could not identify any aggravating or alleviating factors. He reported that a few days prior to the onset of his symptoms he had slipped out of a chair landing hard on the ground. He did not sustain any head trauma during this incident. He described the fall as “jarring” but denied head or neck pain immediately following the incident. He denied other trauma or recent chiropractic manipulation. His wife stated that she thought his right eye “looked smaller” than the left. The patient also stated that his voice seemed more hoarse since the incident. He did not report any anhidrosis. He denied fever, chills, vision changes, headache, or any focal sensory or motor changes.
Past Ocular History:
Past Medical History:
Ocular Medications:
Systemic Medications:
Allergies:
Family History: :
Social History:
Review of Systems: :
OCULAR EXAMINATION
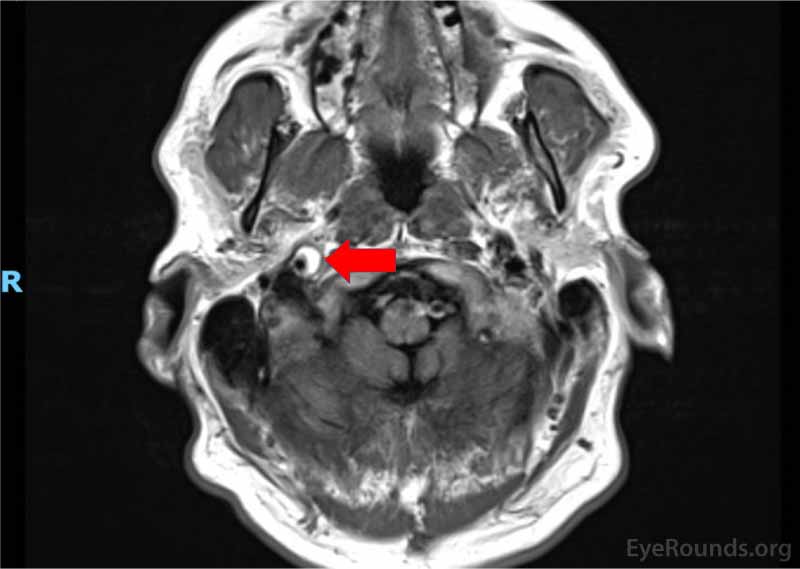
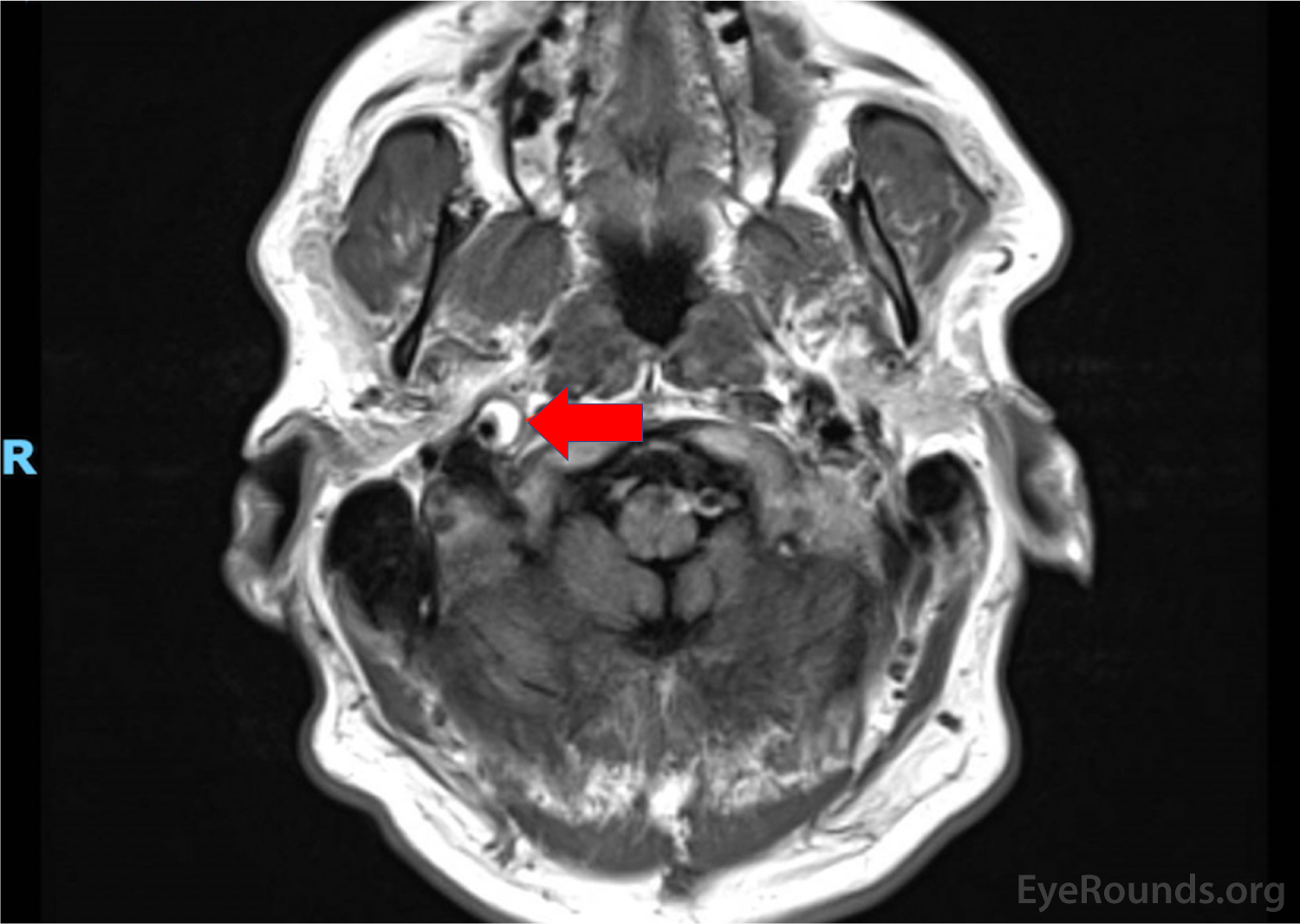
MRI/MRA head/neck/upper chest (Figure 2)
DIAGNOSIS: Horner syndrome secondary to right ICA dissection
CLINICAL COURSE
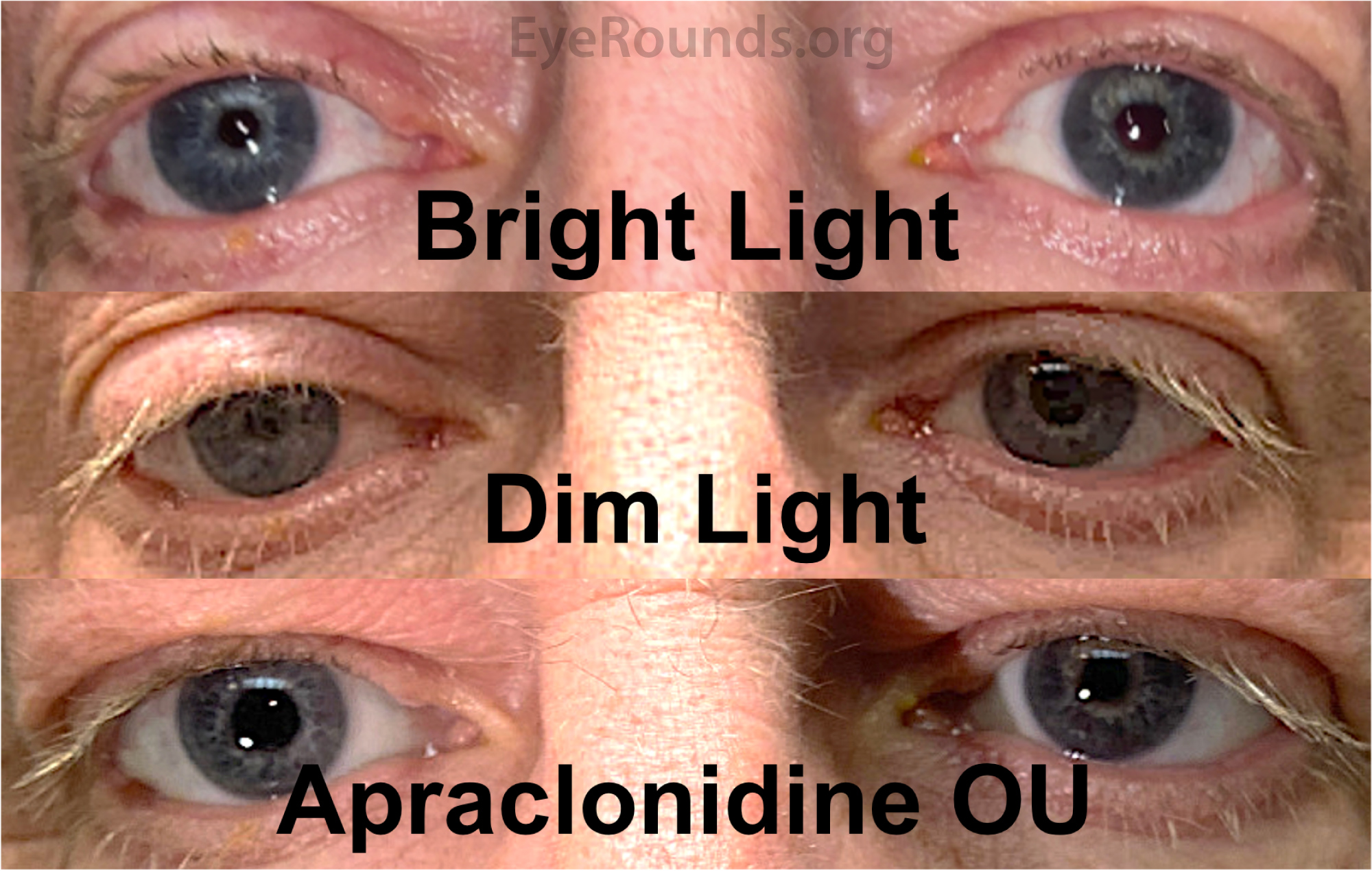
The patient was found to have mild ptosis of the right eyelid and anisocoria greatest in dim light with a mild dilation lag, raising the suspicion of a right oculosympathetic defect. Apraclonidine testing demonstrated reversal of anisocoria and reduction in ptosis, confirming a right Horner syndrome. MRI/MRA of the head and neck confirmed the clinical suspicion of a right ICA dissection and associated pseudoaneurysm. Neurosurgery performed a diagnostic angiogram which confirmed the dissection with non-flow-limiting stenosis and a small pseudoaneurysm noted in the cervical right ICA segment. No neurosurgical procedure was indicated. The patient was started on aspirin 325 mg daily. He was monitored for the subsequent months with resolution of pain and no symptoms of stroke.
DISCUSSION
Introduction
The first step in evaluating any patient with clinically significant anisocoria, which is defined as anisocoria >0.5 mm, is determining if the anisocoria is greatest in dimly versus brightly lit conditions. Anisocoria which increases in bright conditions implies a deficit of the sphincter muscle in the larger pupil suggesting a parasympathetic lesion, pharmacologic mydriasis, or direct damage to the sphincter muscle. Anisocoria that is greater in dim conditions implies a deficit of the dilator muscle in the smaller pupil which suggests a sympathetic lesion or alternatively, a physiological anisocoria. The most common cause of anisocoria that increases in dim light is physiologic anisocoria; however, anisocoria >1mm or a lesser anisocoria that is accompanied by ptosis in the eye with the smaller pupil should be investigated for Horner syndrome. Horner syndrome is a condition that presents with characteristic clinical signs as a result of damage to the ipsilateral oculosympathetic pathway.[1] The classical triad of Horner syndrome is: (1) ipsilateral upper eyelid ptosis, (2) miosis and (3) facial anhidrosis.[2] The diagnosis is based on clinical signs but may be confirmed with pharmacologic testing. Understanding the anatomical neuronal pathways of the sympathetic innervation to the eye and face is critical to understanding the signs and symptoms of Horner syndrome.
PATHOPHYSIOLOGY
Sympathetic innervation to the eye is mediated by a three neuronal chain that begins in the hypothalamus. First order neurons arise in the posterolateral hypothalamus and descend through the intermediolateral brain stem before synapsing in the lateral column of the spinal cord at the ciliospinal center of Budge at the level of C8-T1.[2] Infarctions and neoplasms near the hypothalamus or along the pathway of the first order neuron may interrupt the sympathetic supply and cause Horner syndrome. In addition to the classical triad of miosis, ptosis, and anhidrosis, central preganglionic lesions often have additional clinical manifestations due to the close proximity of nearby neurological structures. For example, in Wallenberg syndrome, which is an infarction of the lateral medulla, patients can present with a Horner syndrome in addition to nystagmus, skew deviation, ataxia, ipsilateral sensory loss on the face, and contralateral hemisensory loss on the body, dysphagia, hoarseness, hiccups and vertigo.[3]
Preganglionic second order neurons originate in the ciliospinal center of Budge, then exit the spinal cord at T1 and pass across the pulmonary apex before synapsing in the superior cervical ganglion located at the level of the bifurcation of the common carotid artery.[2] Neck surgery, trauma, pneumothorax, and neoplasms along the apex of the lung, such as Pancoast tumors, can damage the second order neuron. Preganglionic lesions are often associated with ipsilateral shoulder pain and weakness/numbness in the C8-T1 distribution.[3]
Postganglionic or third-order neuronal cell bodies originate in the superior cervical ganglion. The sympathetic nerve fibers then travel along the adventitia of the internal carotid artery into the cavernous sinus. In the cavernous sinus, they travel with the abducens nerve before joining the ophthalmic division of the trigeminal nerve. Efferent fibers enter the orbit via the superior orbital fissure and travel along the two long ciliary nerves to the iris dilator, and also supply the Müller smooth muscle in the upper and lower eyelid.[3 ,4] Postganglionic sympathetic fibers also travel along the external carotid artery, and supply skin sweat glands and blood vessels in the face with the exception of the skin over the brow.(3)
Internal carotid artery dissection affects the third-order neuron and can classically present with Horner syndrome. An internal carotid artery dissection is due to a spontaneous or trauma-related tear in the intimal layer of the artery which can lead to the formation of an intramural hematoma. This hematoma can bulge inwards towards the lumen of the artery, causing stenosis or the hematoma can expand outwards causing a pseudoaneurysm.[5] When intimal internal carotid artery dissections cause stenosis, there is an increased risk of thrombus formation in the lumen, which can cause a stroke. Dissections of the adventia can also cause a Horner syndrome, but there is no associated luminal narrowing. Expanding hematomas or pseudoaneurysms along the internal carotid artery compress postganglionic sympathetic fibers in about half of carotid dissection cases.[6] Lesions to the postganglionic neurons in this region do not affect facial sweating (except in the area of skin above the eyebrow) because the sympathetic supply to the sweat glands ascends along the external carotid plexus.[6]
Signs/Symptoms:
Patients with Horner syndrome most commonly present with mild ipsilateral eyelid ptosis and anisocoria. The ptosis involves both the upper and lower eye lid (“upside down” or reverse ptosis) due to loss of sympathetic innervation to the Müller muscle located in both the upper eyelid and lower eyelid. The upper and lower lid ptosis can give the false appearance of enophthalmos. Denervation of the iris dilator muscle results in miosis of the affected pupil most pronounced in dim light. In comparison, anisocoria caused by a parasympathetic lesion affects the sphincter muscle; thus the anisocoria is most pronounced in bright light.[4] In addition to miosis, patients with Horner syndrome will exhibit a dilation lag of the affected pupil. The normal pupillary response to the removal of a light is brisk dilation. In Horner syndrome there is a dilation lag, or delay in dilation, due to the weakness of the dilator muscle. This is most evident between 5 to 15 seconds after a light stimulus is removed, during which time the parasympathetic innervation continues to be inhibited at a central level in darkness, allowing the involved pupil to passively dilate. Another sign often included in the classical triad of Horner, but is less often clinically apparent, is ipsilateral facial anhidrosis.[3] Preganglionic lesions tend to cause more noticeable loss of sweating over a larger area of skin besides the face, compared to the postganglionic lesions.[1] Reinnervation of the sweat glands over time is common, so anhidrosis may not be long-lasting. Most oculosympathetic lesions are incomplete or partial and may affect one end organ more than another (e.g. anisocoria may be disproportional to the ptosis or vice versa).
Lastly ipsilateral facial pain, retroorbital pain, jaw or tooth pain are common in carotid dissection and their presence should raise the clinical suspicion for this diagnosis.[6] Physicians should maintain a high index of suspicion for carotid artery dissection in patients with recent head or neck trauma, surgery, history of repeated neck movements with sports activity or spinal manipulation by a chiropractor. Carotid dissection have even been reported after amusement park rides in which high G forces occur.
DIAGNOSIS
Diagnosing Horner Syndrome begins by acquiring a detailed history and performing a thorough pupillary examination. Horner syndrome should always be considered in a patient presenting with anisocoria > 0.5mm that is more prominent in dimmer conditions. Physicians should also note the presence of an associated ipsilateral ptosis, dilation lag of the smaller pupil, and a history of anhidrosis. The diagnosis is confirmed through pharmacologic testing using topical cocaine or apraclonidine. Cocaine blocks the reuptake of norepinephrine (NE) at the synaptic cleft. A normal pupil should dilate 40 to 60 minutes following instillation of 4% cocaine. Any disruption of the sympathetic chain will result in decreased NE release leading to poor pupillary dilation on the ipsilateral side. Anisocoria >0.8mm after cocaine testing is highly suggestive of a Horner syndrome.[2] The initial difference in pupil size between the affected and unaffected pupil is less reliable for diagnosing Horner than the net change in the pupillary difference after administrating cocaine.
In recent years, apraclonidine has been replacing cocaine as the gold standard. Recent studies comparing the efficacy of cocaine and apraclonidine suggest that apraclonidine has higher sensitivity and is a more accurate test for diagnosing Horner syndrome.[7] The sympathetic denervation caused by Horner syndrome leads to alpha-1 receptors upregulation on the iris dilator muscle; a process called denervation hypersensitivity. The denervation supersensitivity takes place 48 hours or more after the decrease in sympathetic tone. Apraclonidine is a strong alpha-2 agonist with weak alpha-1 agonist activity. Approximately 60 minutes after apraclonidine is instilled, a pupil affected by Horner syndrome will dilate . A major limitation of apraclonidine is false negativity if testing is done less than 48 hours from injury, due to the lack of denervation hypersensitivity. Furthermore, apraclonidine has also been associated with CNS and respiratory depression in children younger than one year of age and therefore, should be avoided in pediatric patients or they should be closely monitored after drop administration.[4 ,7]
Once a diagnosis of Horner syndrome is confirmed with cocaine or apraclonidine, hydroxyamphetamine can be used to localize the lesion to preganglionic (1st and 2nd order neurons) or postganglionic (3rd order neurons).[8] Hydroxyamphetamine causes release of presynaptic NE stores in the nerve ending supplying the iris dilator muscle. Testing is performed by instilled 1% hydroxyamphetamine in both eyes then examining the pupils 60 minutes later. If the lesion is preganglionic, hydroxyamphetamine testing will result in dilation of the Horner pupil because the postganglionic neurons innervating the iris dilator muscle are intact and have NE stores. If the lesion is postganglionic, and at least one week has elapsed, the NE stores will have become depleted. This results in less dilation of the denervated affected pupil compared to the contralateral normal eye resulting in increased anisocoria. In the setting of a postganglionic carotid dissection of less than one week’s duration, the hydroxyamphetamine test may falsely indicate a preganglionic lesion because the postganglionic presynaptic neuron stores of NE may not have yet become depleted. Because cocaine inhibits the uptake of adrenergic agents, such as hydroxyamphetamine, hydroxyamphetamine testing should be performed at least 72 hours after a cocaine test.[2 ,8] Unfortunately, topical hydroxyamphetamine has become less available for use, and it is also not always a reliable method of localizing preganglionic lesions in congenital or in cases where Horner syndrome occurred in infancy, which has been associated with secondary anterograde degeneration of the third order neuron, producing a false localization to the post-ganglionic neuron.[4]
Imaging:
Newly diagnosed Horner syndrome always warrants imaging. The imaging modality of choice depends on the suspected etiology. Brainstem infarcts, tumors, or demyelinating disease are evaluated using MRI. Carotid dissections are assessed using CT angiogram or MRI/MRA of the head and neck. CT of the chest is often performed to evaluate a suspected tumor or lesions in patients with arm pain and/or a heavy smoking history.[3 ,8]
Treatment/Management:
Management of Horner syndrome focuses on identifying and treating the underlying etiology. Imaging of the oculosympathetic pathway should be performed in patients with isolated Horner syndrome without an obvious etiology. Most often this condition is benign or idiopathic with normal imaging but appropriate evaluation of secondary causes is essential to recognize and treat life-threatening underlying pathology. The most common identifiable cause of isolated Horner syndrome is carotid artery dissection.[9] The ptosis and miosis of Horner syndrome usually does not result in loss of functional vision and is typically asymptomatic. For cosmetic purposes, apraclonidine eye drops can be used for reversal of ptosis for 4-6 hours duration. Lastly, eyelid surgery has also been shown to be effective in reducing ptosis and offers a more permanent treatment.[3]
ETIOLOGY
|
DIAGNOSIS
|
SIGNS
|
TREATMENT/MANAGEMENT
|
References
Wole B., Diel RJ, Stiff HA, Kardon RH. Horner syndrome due to ipsilateral internal carotid artery dissection. EyeRounds.org. Posted December 8, 2020. Available from http://www.EyeRounds.org/cases/300-miller-fisher-syndrome.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links


{kind=link}
{kind=link}