
INITIAL PRESENTATION
Chief Complaint: Bloody tears from the right eye
History of Present Illness:
A 63-year-old woman with hereditary hemorrhagic telangiectasia, portal hypertension, pulmonary hypertension, and seasonal allergies was referred to the comprehensive ophthalmology clinic by family medicine for bloody tearing from her right eye. She was admitted to the hospital for altered mental status secondary to hepatic encephalopathy. During her hospital course, she had two episodes of bright red blood from the nasal corner of her right eye. She reported having itchy eyes due to her chronic seasonal allergies, and as she went to wipe her right eye with a tissue, she noticed blurry vision and blood on her finger, both lasting approximately five minutes. She denied any blurred vision or bleeding from the left eye. She also denied ocular pain, flashes of light, curtaining, or double vision from either eye. She normally wore reading glasses but did not bring them with her to the hospital. She used artificial tears occasionally for dry eye symptoms.
Past Ocular History:
Medical History:
Medications:
Allergies:
Sensitive to cyclosporine, glyburide, and naproxen sodium – reactions unspecified.
Family History:
Social History:
Retired, lives with her daughter. Patient does not consume alcohol or use recreational drugs. She has never smoked.
Review of Systems:
Negative except for what is detailed in the history of present illness
OCULAR EXAMINATION
Differential Diagnosis:
CLINICAL COURSE
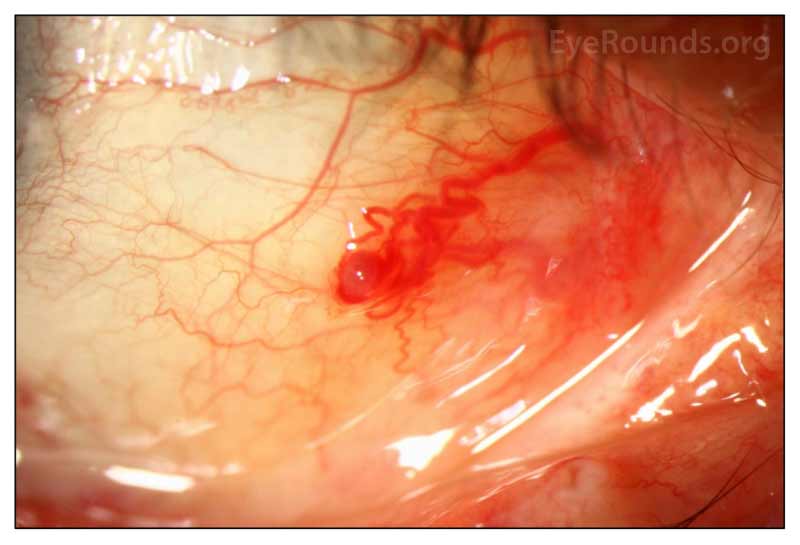
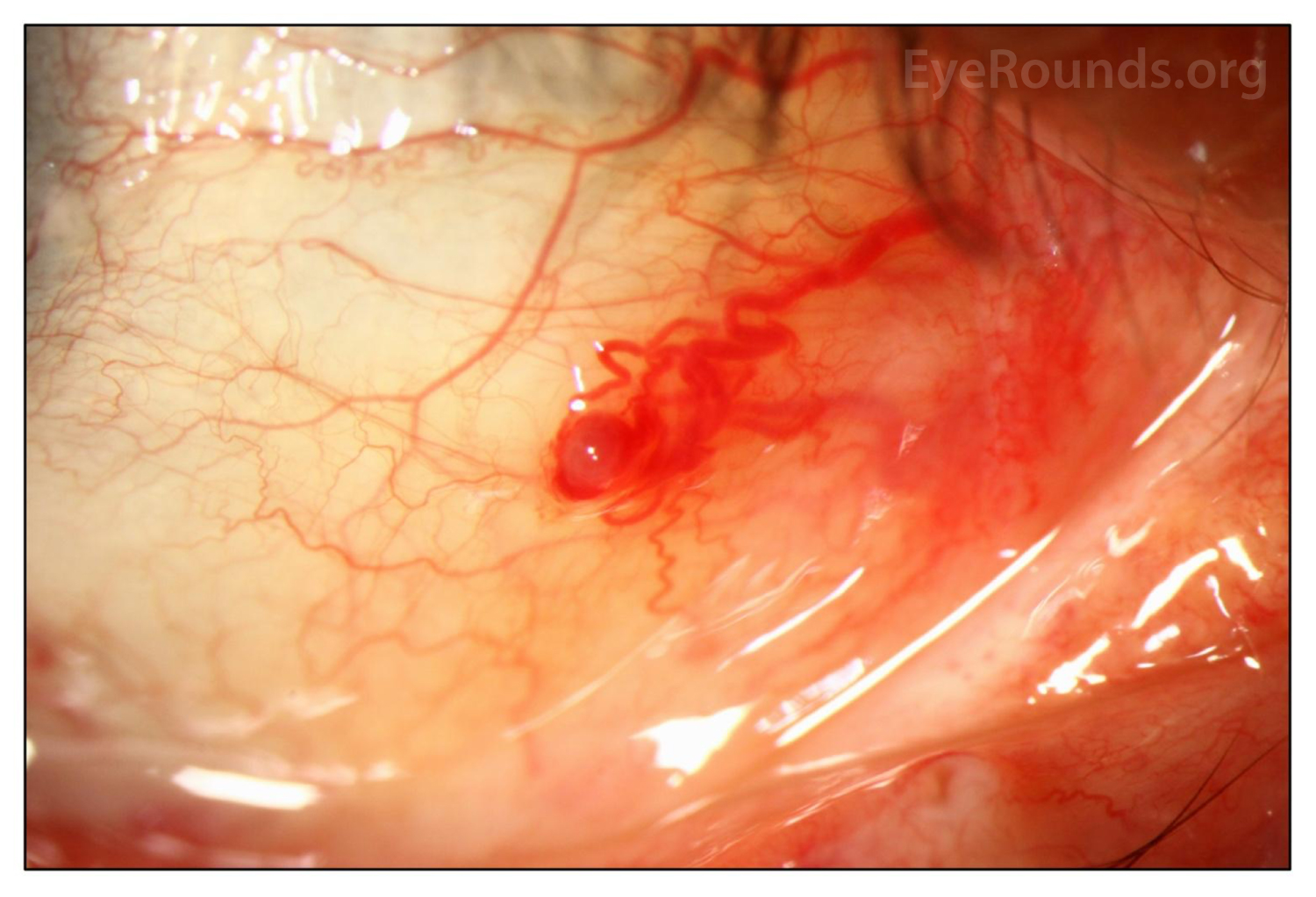
Slit lamp examination revealed a 1x1 mm superficial telangiectasia on the nasal bulbar conjunctiva OD (Figure 1). The bleeding was thought to be likely due to minor ocular surface trauma secondary to eye rubbing around the telangiectasia, resulting in the reported bloody tears. She has underlying dry eye disease and seasonal allergies that may have contributed to irritation and ocular surface fragility. Her baseline blurry vision was thought to be due to her dry eye symptoms.
DIAGNOSIS: Hemolacria secondary to Hereditary Hemorrhagic Telangiectasia
DISCUSSION
Hemolacria (bloody tears) is a rare condition with a broad differential diagnosis ranging from idiopathic, infectious, inflammatory, vascular, traumatic, and neoplastic etiologies to side effects of topical medications (e.g., silver nitrate) [1]. However, most cases of hemolacria are secondary to benign conjunctival lesions [2]. Due to the association between severe systemic and ocular diseases, a thorough evaluation is recommended for all patients presenting with new onset hemolacria. Patients should undergo a comprehensive ophthalmic and systemic examination to identify organic causes or sources of bleeding, whether it be from the conjunctiva, lacrimal puncta, lid margin, tear glands, or orbit [1]. Treatment of hemolacria is diverse and is aimed at correcting the underlying condition. If the history, physical exam, and imaging studies are consistent with a benign conjunctival lesion, it is reasonable to observe to ensure resolution of symptoms. If an infection is suspected, application of topical antibiotics may be appropriate.
Hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber disease) is a rare genetic disorder characterized by the formation of vascular malformations. Diagnosis of HHT is based on Curaçao's clinical criteria, which include the presence of multiple telangiectasias in the skin and mucous membranes, recurrent epistaxis, visceral involvement (e.g., arteriovenous malformations in the lung, brain or liver) and a first degree relative with HHT [3]. It is inherited in an autosomal dominant fashion and is commonly caused by mutations in the ENG (i.e., HHT1 subtype) or ALK1 genes (i.e., HHT2 subtype). Ocular involvement is common in HHT and reports of hemolacria in HHT patients have been previously documented [4]. In a previous cross-sectional study of 206 HHT patients, 44.1% of patients harboring ALK1 mutations developed ocular telangiectasias [3]. Most ocular telangiectasias were located in the tarsal conjunctiva, bulbar conjunctiva, lid margin, and caruncle [3].
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
References
Velez G, Dotson AD, Oetting TA. Hemolacria Secondary to Hereditary Hemorrhagic Telangiectasia. EyeRounds.org. June 18, 2021. Available from https://eyerounds.org/cases/313-Hereditary-Hemorrhagic-Telangiectasia.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links

{kind=link}