
INITIAL PRESENTATION
Chief Complaint: Worsening floaters in the left eye
History of Present Illness:
A 40-year-old male was referred to the University of Iowa for worsening floaters in his left eye starting two months prior to presentation. Additionally, he reported a subjective decrease in visual acuity in his left eye during this time period. He otherwise denied flashes of light and eye pain, and denied symptoms in the right eye. His review of systems was significant for diffuse, scattered inflammatory skin nodules consistent with a known diagnosis of hidradenitis suppurativa (HS) managed with oral doxycycline.
Past Ocular History: None
Past Medical History:
Medications: Doxycycline 50 mg once daily
Allergies: None
Family History: Non-contributory to current presentation
Social History: Denied tobacco and ethanol use
Review of Systems: As per noted in HPI, otherwise negative.
OCULAR EXAMINATION
|
Left Eye |
Right Eye |
|
|
Vitreous |
Clear, no cell or flare |
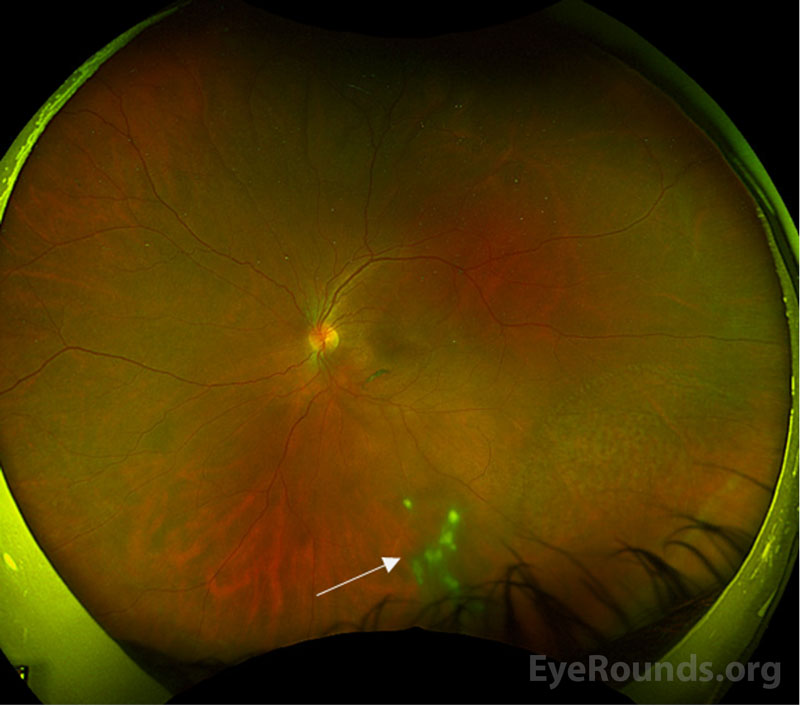
2+ anterior vitreous cells, trace flare, inferior vitreous snowballs |
|
Disc |
Normal |
Normal |
|
Cup-to-disc ration |
0.2 |
0.2 |
|
Macula |
Normal |
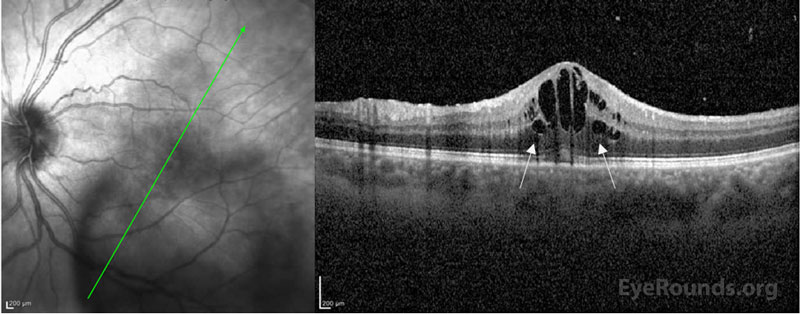
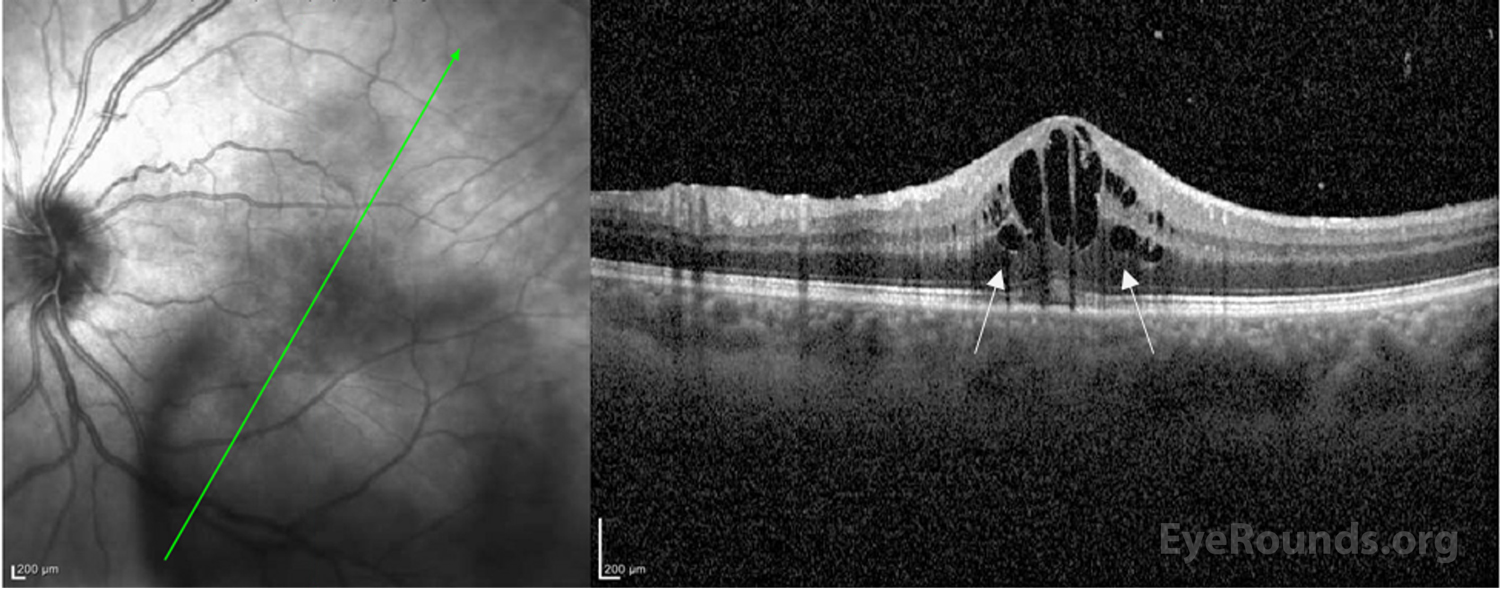
2-3+ cystoid macular edema |
|
Vessels |
Normal, no vascular sheathing |
Normal, no vascular sheathing |
|
Periphery |
Normal |
Normal |
IMAGING
Differential Diagnosis:
DIAGNOSIS: Intermediate uveitis associated with hidradenitis suppurtiva
CLINICAL COURSE
Given that intermediate uveitis has a broad differential, a comprehensive work-up was obtained. A complete metabolic panel, complete blood cell count with differential, serum erythrocyte sedimentation rate, serum C-reactive protein, rheumatoid factor, antinuclear antibody testing, anti-neutrophil cytoplasmic antibody testing, angiotensin-converting enzyme level, Lyme antibody, QuantiFERON gold testing for tuberculosis, and syphilis antibody testing were all negative or normal. While pars planitis was considered as a diagnosis, this is a diagnosis of exclusion. In this case, however, the intraocular inflammation was linked to the patient’s known history of hidradenitis suppurtiva. He was treated with difluprednate 0.05% four times daily in the left eye and monitored with serial imaging. Co-management with dermatology was required to ensure appropriate systemic treatment for his underlying disease. In this case, oral doxycycline was used. Ultimately his visual acuity returned to 20/20 in both eyes with resolution of cystoid macular edema and intermediate uveitis. Fluorescein angiography was obtained post-treatment and ensured resolution of petaloid macular leakage. The patient’s treatment course was complicated by steroid response ocular hypertension, which was treated with dorzolamide/timolol twice daily. He was eventually transitioned to prednisolone acetate 1% and tapered to once daily treatment of the left eye with continued quiescence of his ocular inflammation.
This case highlights the importance of considering HS in association with inflammatory eye disease and of performing a thorough review of systems in all patients presenting with ocular inflammation. [1,2] Furthermore, the presence of inflammatory eye disease may be indicative of uncontrolled systemic disease that may require treatment escalation; therefore a careful systemic review of systems is critical for these patients. [2]
DISCUSSION
Etiology/Epidemiology
Intermediate uveitis represents a type of uveitis in which the primary site of inflammation is the vitreous. [3] Specifically, intermediate uveitis includes pars planitis, posterior cyclitis, and hyalitis. Given the ambiguity of these terms, however, the International Uveitis Study Group (IUSG) reserves the diagnostic term pars planitis for the subset of intermediate uveitis that occurs in the absence of an identifiable cause (ie, infection or associated disease). [3] Intermediate uveitis is the least common form of uveitis. It represents about 15% of all uveitides based on previous surveys performed worldwide. [4, 5] Intermediate uveitis is described primarily as a disease of young adults, and most commonly occurs in patients under the age of 40 years. [6] It does not have gender, racial, or ethnic predilection. [5, 6] The majority of intermediate uveitis cases have bilateral involvement. [5] Systemic associations are reported in up to 30% of patients and varies with population studied. [10] Of the systemic associaions, sarcoidosis and multiple sclerosis are most commonly identified and reported. [10]
Hidradenitis suppurativa (HS) is a chronic, recurrent inflammatory skin disease preferentially affecting the intertriginous skin and epidermis-containing apocrine glands. [11, 12] The condition manifests as painful nodules in intertriginous areas that can progress to abscesses, fistulae, and sinus tracts. These characteristic lesions may rupture and form scars. Globally, the prevalence of HS is estimated to range from 0.05% to 4.10%, although the exact prevalence is unknown. [11] Depression, anxiety, pain, and high body mass index are highly correlated with HS due to its profound negative effect on quality of life measures. [13, 14]
Pathophysiology
The exact underlying pathogenic mechanisms of intermediate uveitis are not well understood. The common effector mechanisms identified in experimental models implicate the release of major cytokines IL-17 and IFN- γ via a T cell-mediated pathway. [15] There are some associations between human leukocyte antigens (HLA) haplotypes, specifically HLA-DR15, HLA-DR51, and HLA-DR17, that may suggest an immunogenetic predisposition. [4, 9]
In terms of HS, the exact underlying pathogenesis also remains unknown but is postulated to include a combination of genetic predisposition and environmental triggers that predispose to epithelial fragility. [14] The primary cytokines identified in this inflammatory process are TNF-alpha and IL-17. [14] These cytokines are also well established in the pathogenesis of inflammatory eye disease. Despite this plausible link, few reports exist identifying the prevalence of inflammatory eye disease in patients with HS. In the largest retrospective cohort to date, only one of 236 patients had intermediate uveitis associated with HS. [1]
Signs/Symptoms:
Patients typically present with blurry vision or new floaters. Sudden vision loss may occur secondary to exudative or rhegmatogenous retinal detachment. Though many cases are bilateral at presentation, symptom severity tends to be asymmetric.
A diagnosis of intermediate uveitis requires the presence of pars plana exudates (“snowbanks”) or accumulation of fibroinflammatory debris in the inferior vitreous (“snowballs”), but can also be associated with other clinical findings of ocular inflammation (see Table 1). [3] Floaters reported by patients are the result of the shadows cast by vitreous cells and debris on the retina.
|
Clinical manifestations of Intermediate Uveitis |
|
|
Required findings |
OR
|
|
Possible associated findings |
|
Laboratory work-up:
In an individual presenting with intermediate uveitis, a broad infectious and inflammatory work up must be completed. If a comprehensive work-up is normal or negative, then a diagnosis of pars planitis should be considered. The initial work-up is guided by clinical suspicion but should include basic inflammatory and infectious tests to rule out commonly missed diseases such as syphilis and tuberculosis (see Table 2).
In children, care should be taken to differentiate intermediate uveitis from other forms of chronic uveitis such as juvenile idiopathic arthritis. [18] Another important association for the clinician to bear in mind is the strong association between intermediate uveitis and multiple sclerosis (MS) in patients of all ages. [19] If there are signs or symptoms suggestive of multiple sclerosis, evaluation with magnetic resonance imaging (MRI) of the brain with possible cerebrospinal fluid analysis should be considered.
Imaging:
Imaging is not required for the diagnosis of intermediate uveitis but can provide helpful adjunctive information and for tracking disease progression (see Table 2).
|
Laboratory testing |
|
|
Imaging |
|
Treatment & Management:
Patients with intermediate uveitis typically have a long treatment course often complicated by relapsing and remitting disease. Treatment options vary based on severity of intraocular inflammation and individual practice, but include consideration of topical steroids, local injections of corticosteroids, intravitreal injection of corticosteroids, oral steroids, and systemic immunomodulatory therapy. [10] Despite the long disease course and frequent complications of intermediate uveitis, the visual prognosis remains favorable with a recent cross-sectional study reporting a median 10-year visual acuity of 20/30. [10]The most frequent cause of vision loss in patients with intermediate uveitis is cystoid macular edema (CME). [20] Other less common complications include vitreous hemorrhage, epiretinal membrane, and development of ocular hypertension/uveitic glaucoma. [21]
In the setting of systemic disease, the patient may benefit from multi-disciplinary management as in this case.
EPIDEMIOLOGY & ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
|
References
Mansoor M, Diel RJ, Abramoff MD. Intermediate uveitis associated with hidradenitis suppurativa. EyeRounds.org. August 25, 2022. Available from https://EyeRounds.org/cases/328-hidradenitis-suppurativa.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links

{kind=link}
{kind=link}