

INITIAL PRESENTATION
Chief Complaint: Decreased vision and new floaters in both eyes
History of Present Illness:
A 76-year-old female with a history of chronic interstitial cystitis presents with decreased vision and new visual disturbances in both eyes. She has been on Pentosan for 10 years prior to this visit.
She states that over the last year her vision has been blurry at distance and near in both eyes. She has also noticed “blue floaters” intermittently associated with walking into the sunlight that last for a few seconds at a time. She denied flashes of light or light sensitivity.
Past Ocular History:
Past Medical History:
Medications:
Allergies:
Family History:
Social History:
Review of Systems:
OCULAR EXAMINATION
DIFFERENTIAL DIAGNOSIS:
CLINICAL COURSE
Based on the gradual visual decline and symmetric macular changes with characteristic fundus autofluorescence, the patient was diagnosed with presumed pentosan polysulfate maculopathy and asked to discontinue the medication. She stopped the medication and returned 6 months later with relatively stable visual acuity in both eyes. There was mild progression of the atrophic areas which appeared more rapidly than what is expected with typical ARMD, further supporting a diagnosis of Pentosan-associated maculopathy. Her cumulative dose of pentosan polysulfate sodium at the time of presentation was approximately 1,460 g.
DIAGNOSIS: Pentosan polysulfate maculopathy
DISCUSSION
Etiology/Epidemiology
Pentosan polysulfate sodium (PPS) is a medication approved by the FDA in 1996 to treat bladder pain and discomfort associated with interstitial cystitis. Pharmacologically, Pentosan works as a heparin-analogue that is thought to adhere to bladder mucosal cells and act as a protective-barrier to urinary irritants [2] . Interstitial cystitis has been estimated to affect between 2.7%–6.5% of women aged ≥18 years and 1.9%–4.2% of men with a strong female predominance [3, 4].
Emerging studies have shown that the use of PPS can be associated with a pigmentary maculopathy in a dose-dependent manner, the first of which was a case-series published by Pearce et al in 2018 identifying 6 patients whose clinical presentations were unified by the long-term use of PPS [2]. Since then, a few other studies have identified patients with similar presentations who had taken or were currently taking PPS.
Given this is a newly discovered association, no current prevalence is well documented. However, there is a large study from Kaiser Permanente Medical Center which attempted to quantify prevalence via identification in the electronic medical record. Of 1,120 patients with a diagnosis of IC, 475 (42%) were currently taking PPS. They identified 138 patients who had been dispensed at least 500g of PPS in the prior 20 years and successfully examined 117 patients with a complete ophthalmic examination as well as multimodal imaging. They found that approximately 1/4th of patients who had taken at least 500g of PPS developed clinical characteristics similar to those reported by Pearce et al and this rate increased with increasing cumulative dose [5]. The average age of these patients was approximately 60 and most patients were female. Another study examined a group of 50 patients who were prescribed PPS in a 6 year period and found that roughly 20% exhibited clinical findings consistent with pentosan polysulfate maculopathy [6]. Other risk factors such as body weight, renal or liver disease (pertinent in Plaquenil toxicity) have yet to be identified.
Pathophysiology
The exact mechanism by which PPS causes retinal toxicity is currently unknown. Current theories suggest that blockage of fibroblast growth factor ei¬ther causes direct RPE damage or interferes with repair and maintenance of the RPE [6, 7]. Additional studies are needed to investigate this further.
Signs/Symptoms
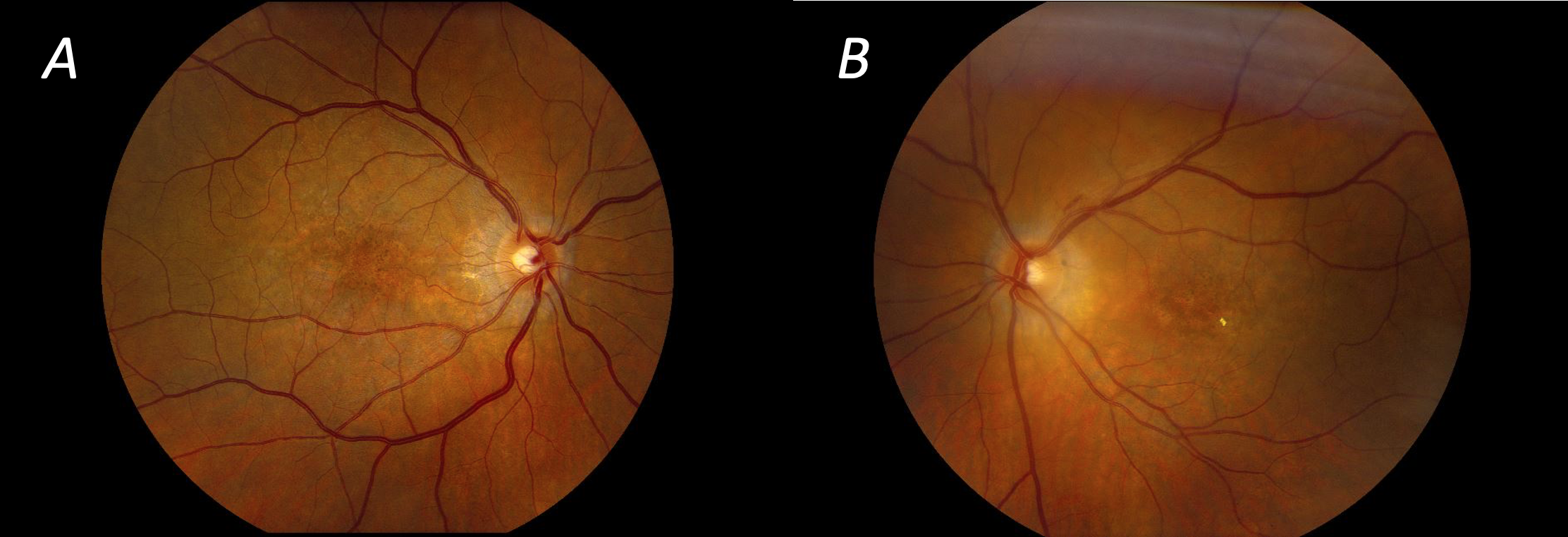
Although some patients are asymptomatic, the most commonly reported symptoms include prolonged dark adaptation, metamorphopsia, and blurred vision [2, 8]. Best-corrected visual acuity is often preserved with 20/40 or better vision, although there were a few patients reported with significantly poorer visual acuity who had more pronounced foveal involvement. Fundus examination often revealed paracentral hyperpigmentation and pale-yellow or orange vitelliform-like deposits. More severe presentations included areas of geographic atrophy [2, 6, 8]. Pentosan associated maculopathy can share features of inherited retinal diseases and age-related macular degeneration which can lead to misdiagnosis and a potentially worse outcome if a patient remains on pentosan until the correct diagnosis is made [1].
Imaging
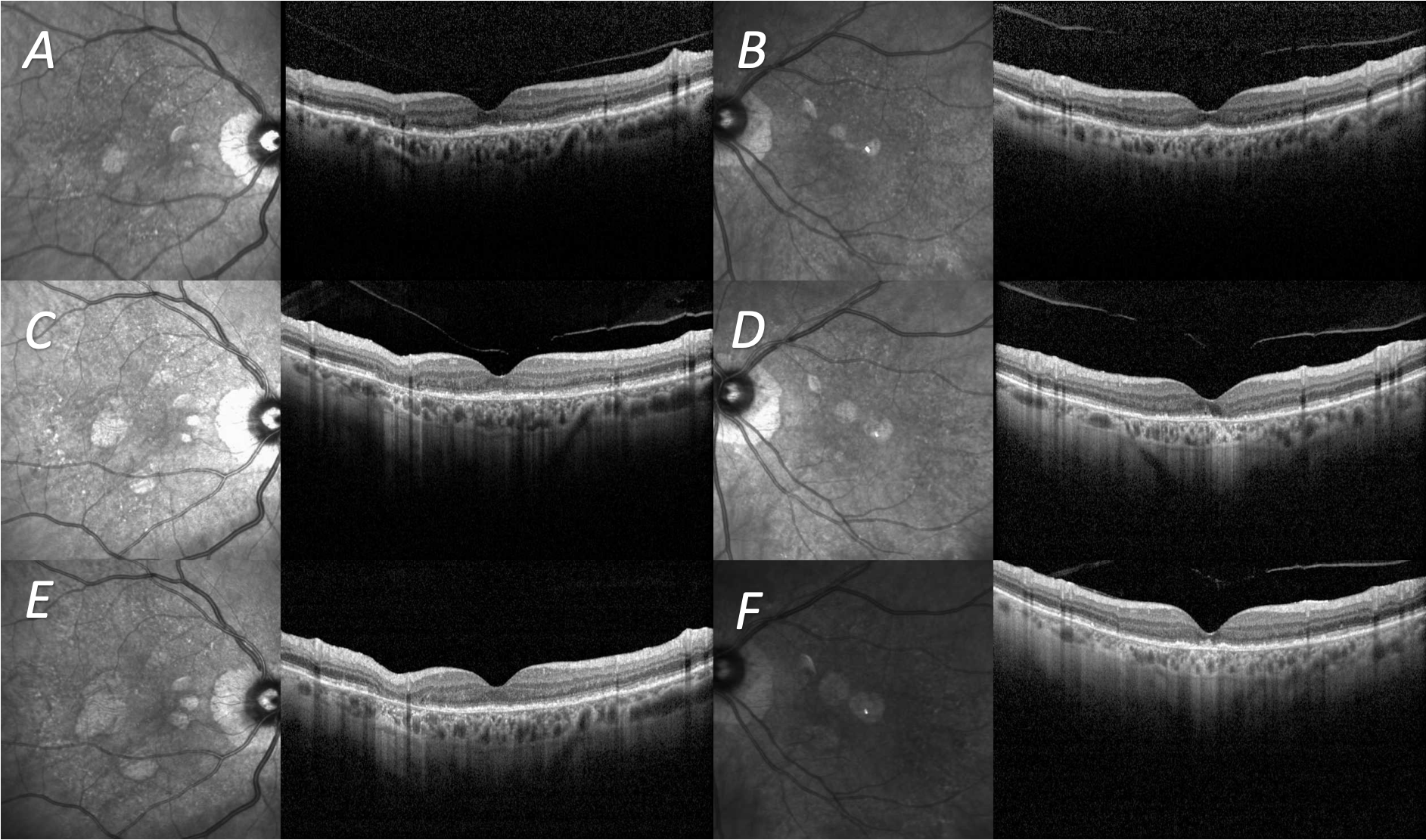
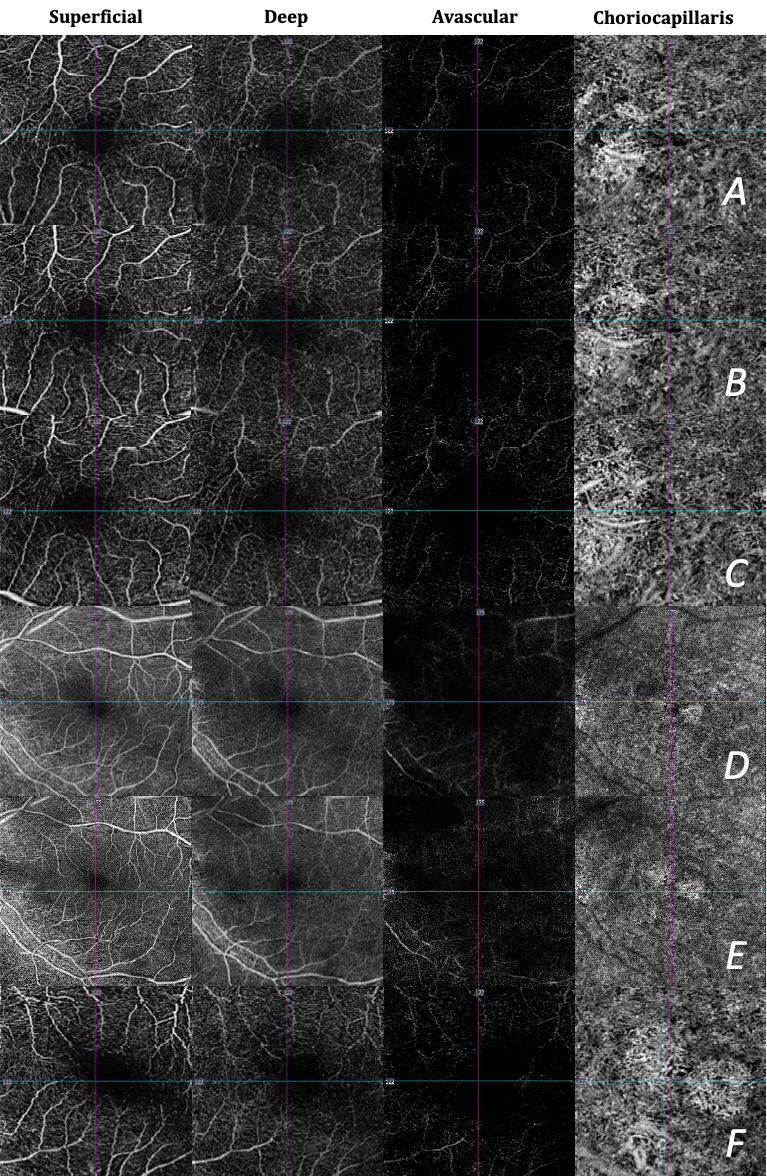
Optical coherence tomography (OCT) of the macula shows excrescences at the level of the RPE early in the disease. Later in the disease, excrescences in the RPE may collapse and RPE atrophy and outer retinal tubulations can be seen [2, 6]. OCT-A shows abnormalities in the foveal avascular zone and areas of choriocapillaris dropout [6, 9].
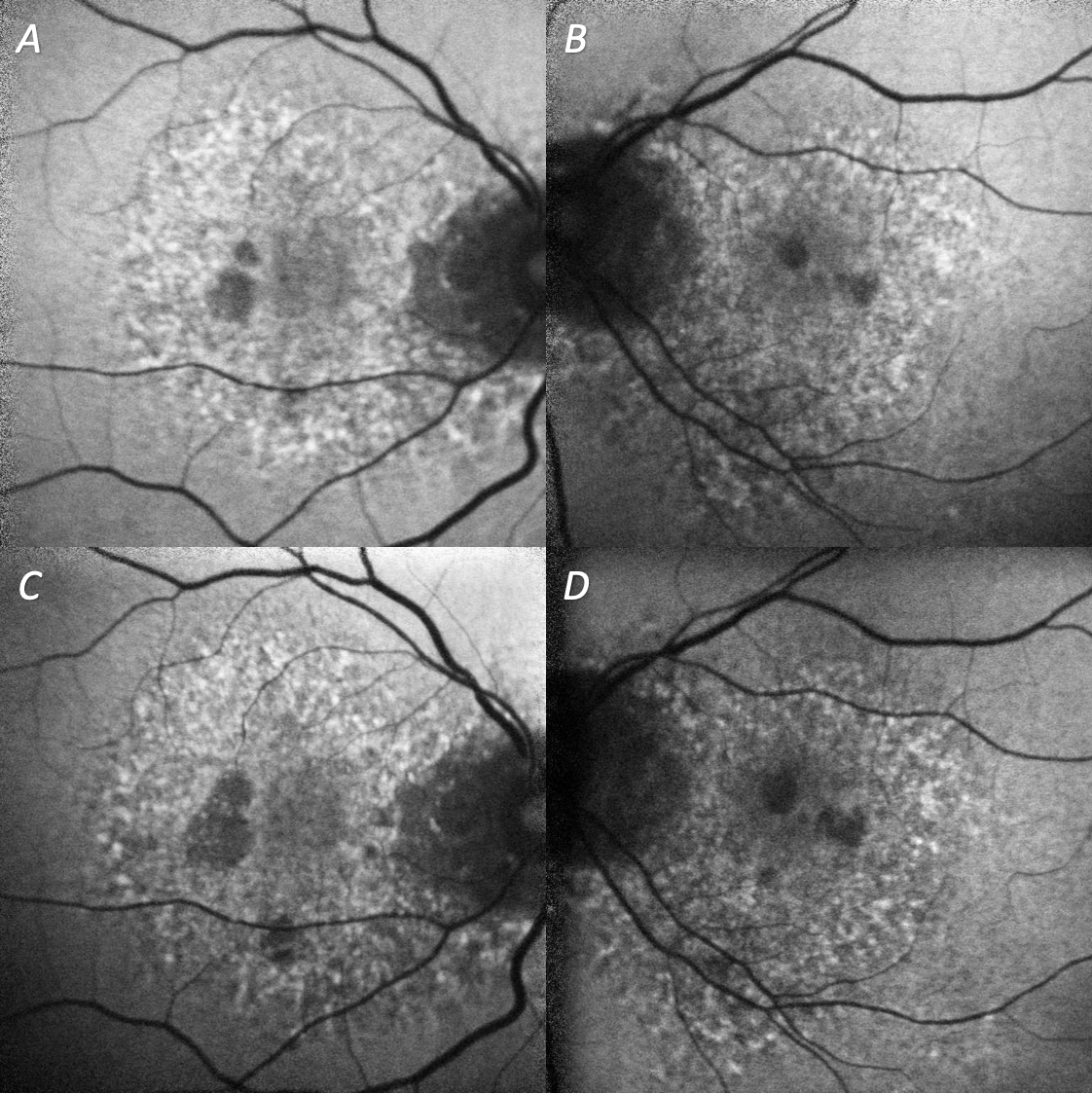
The most striking feature of this disease is seen on fundus autofluorescence (FAF) which shows a highly irregular, speckled autofluorescence pattern in the posterior pole (including around the optic disc) surrounded by normal autofluorescence elsewhere. Hyperautofluorescent dots correspond to the pale-yellow and orange vitelliform-like deposits and hypoautofluorescence corresponds to areas of RPE atrophy [2, 5, 6, 8]. One study that followed a patient with a cumulative dose of 1,300-2,000g over 18 years with clinical features of pentosan polysulfate maculopathy found progression of changes on FAF up to 6 years even after cessation of PPS [10].
Standard automated perimetry with a Humphrey Field Analyzer can show central or cecocentral scotomas but is otherwise mostly full [2, 8].
Multiple studies have shown full-field electroretinogram (ERG) is mostly normal. Only a few patients, typically those with more severe disease, showed mild attenuation and delay in code and rod responses. Some studies have shown prolonged dark adaptation in affected patients, consistent with reported symptoms [2, 6, 8].
Treatment/Management/Guidelines
Patients with presumed PPS maculopathy need to have this diagnosis discussed with the physician prescribing the medication. Cessation of the medication is strongly recommended to reduce further retinal damage and vision loss, and it is important to discuss that progression may be seen even after cessation of medication. However, some patients may prefer to stay on the medication even with risk of vision loss due to the severity of interstitial cystitis. Thus, it is imperative to discuss the risks and benefits, as well as current knowledge regarding the association of the drug and the maculopathy, with the patient. Some patients can develop secondary complications such as cystoid macular edema which may be treated with carbonic anhydrase inhibitors [9, 11]. If there is suspicion for inherited retinal disease, genetic testing may help clarify the diagnosis. There are no formal screening guidelines currently in place, but with further study these may be implemented. Until these guidelines are developed, patients should undergo a dilated eye examination with OCT and fundus autofluorescence within 6 months of initiating PPS therapy and then at least yearly thereafter. Patients already taking PPS who have not had a dilated eye examination with OCT and fundus autofluorescence within the last year should arrange to be seen.
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
Karam Alawa MD, Alexis Warren MD, Timothy Boyce MD, Elliott Sohn MD. Pentosan Polysulfate Maculopathy. EyeRounds.org. August 2, 2022. Available from https://EyeRounds.org/cases/373-pentosan-polysulfate-maculopathy.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
{kind=link}