INITIAL PRESENTATION
Chief Complaint: Objects warped inward with a blurry spot in the right eye
History of Present Illness
The patient is a 32-year-old male with a history of myopia. Three months ago, the patient was cutting down trees at work when an electrical wire was accidentally cut leading to electrocution. He sustained diffuse burns that affected 15% total body surface area including the face, scalp, left upper extremity, left lateral trunk, and left lower trunk. Initial ocular examination around the time of the incident revealed superficial, bilateral periocular electrical burns with bilateral central corneal epithelial defects. Serial intraocular pressures were normal and there was no evidence of lens pathology. Corneal defects improved with topical erythromycin and artificial tears.
The patient now presents to clinic with continued distortion near the center of the vision of his right eye with objects appearing to be “warped inward”. He endorses similar but more mild symptoms in the left eye. He also reports a gray and blurry spot in the central visual field of the right eye extending temporally. This started approximately 2 weeks after the electrocution event when he was able to start wearing glasses again. More recently, he developed hazy vision over the entire visual field of the right eye, which is different than what he has previously been experiencing. This is significantly affecting his daily activities. He endorses rare flashes of light of unknown laterality. He denies diplopia, discomfort, redness, tearing, or floaters.
Past Ocular History
Past Medical History
Medications
Allergies
Family History
Social History
Review of Systems
OCULAR EXAMINATION
Pinhole
GlareTesting
CLINICAL COURSE
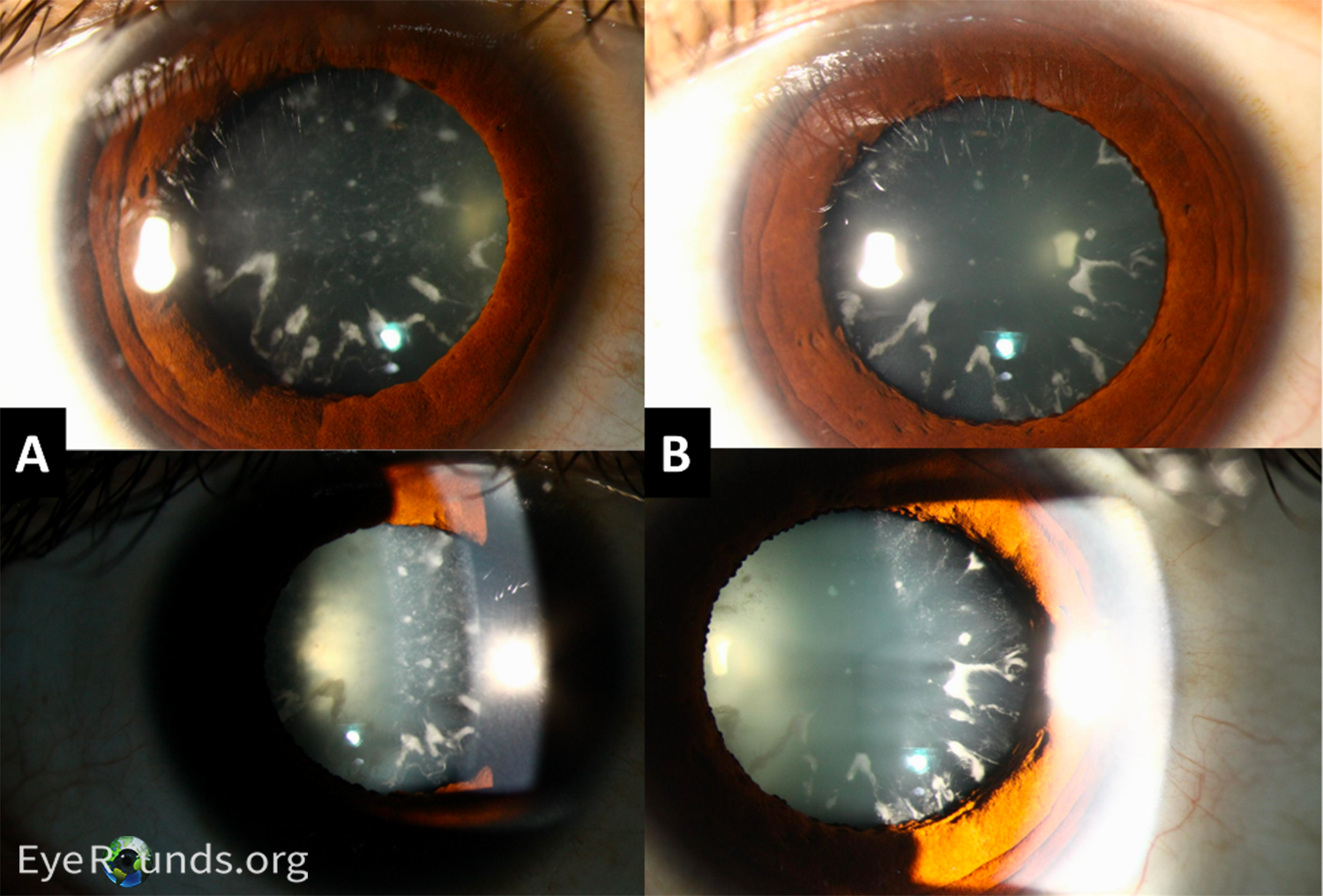
A review of the history showed a thorough eye exam near the time of admission following accidental electrocution with no evidence of prior cataracts. This information along with the rapid cataract progression over the following 2-3 months was consistent with cataract development secondary to electrocution. Subsequent bilateral phacoemulsification with intraocular lens (IOL) implantation was performed. At follow-up 4 months later, he was noted to have 20/25 visual acuity in the right eye with 20/20 visual acuity in the left eye.
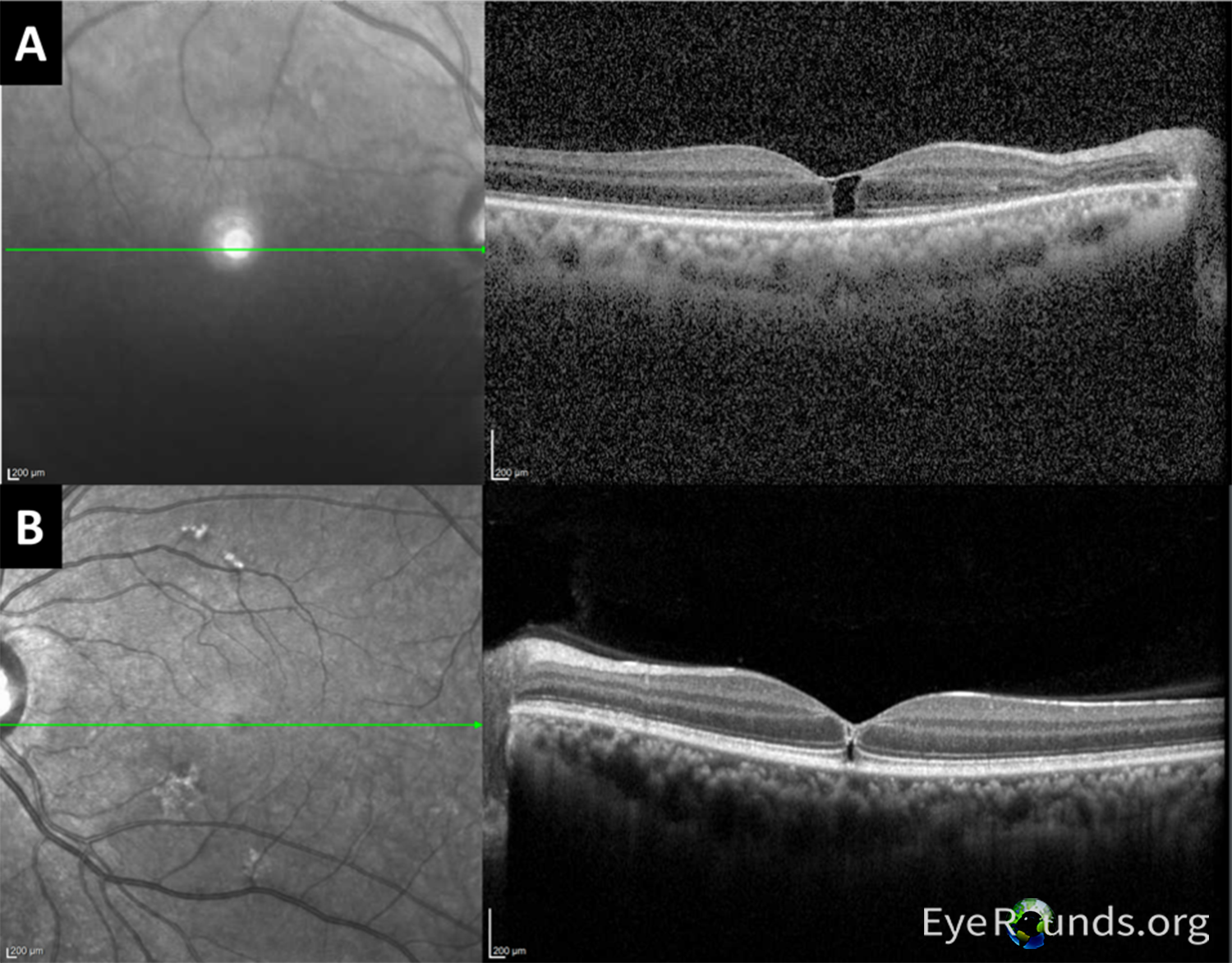
The patient’s complaints of warped vision, visual field loss not mapping to a neurologic region, and OCT findings were significant for a full thickness left macular hole, and the patient was referred for vitreoretinal surgical evaluation. A membrane peel surgery on the right eye was planned to follow 1 month after cataract surgery; however, the patient was lost to follow up. The patient returned 6 months later, and the left macular hole had resolved, and the right hole was noted to be resolving.
DIAGNOSIS: Bilateral cortical cataracts and macular holes secondary to accidental electrocution
DISCUSSION
Etiology/Pathophysiology
A significant number of electrical injuries go unreported making electrocution estimates difficult. However, it is estimated that each year in the United States there are 4,400 cases of electric shock with around 400 deaths. (1) There are numerous reports in the literature of ocular damage following accident electrocution, typically following industrial accidents or lightning strikes. As such, a large variety of ocular sequelae following electrocution has been described. A few examples include hyphema, uveitis, anisocoria, Horner’s syndrome, corneal epithelial lesions, cataract, dislocated lens, vitreous hemorrhage, retinal detachment, macular hole, central retinal vein occlusion, and optic disc edema. (2) However, due to tissue characteristics (3), the lens is the most commonly damaged structure with cataract formation. The incidence of cataract development following electrocution is estimated to be between 0.7 to 8.0%(4,5) and is most commonly anterior subcapsular (6). Reports of concurrent cataract and macular hole development are rarer. (7-12)
Electrocution events involving the head are uncommon. (5) However, the closer the shock is to the eye the more likely ocular manifestations will develop; likewise, it is rare for cataracts to form following electrocution events not involving the head. (13) Typically, 200 V is held to be the cutoff for ocular damage to occur, though retinal damage has been reported at lower voltages, although rarely. (14) One case of possible iatrogenic electric cataracts secondary to electrocardioversion has also been reported (15), though no association with electroconvulsive therapy has been demonstrated (16).
Pathophysiology
Throughout the body, electricity causes damage through two main mechanisms: thermal damage and direct effects on cells including cell membrane disruption and processes similar to electroporation. (17) Tissues with higher resistance are at an increased risk for thermal injury. Within the eye, the lens has relatively high electrical resistance compared to other ocular structures such as the optic nerve and retina. Therefore, it is the most injured component in electrocution, and thus the most extensively studied. While the exact mechanism of lens damage leading to cataract formation is unknown, leading theories include effects from protein coagulation and permeability/osmotic changes. (18,19)
Due to the lower electrical resistance of the retina and optic nerve, damage to these structures (such as full thickness macular holes) is believed to be largely related to vascular ischemia (3) with decreased likelihood of thermal injury. An exception to this is the macula which has a higher amount of melanin increasing its resistance relative to other parts of the retina. (20) The increased resistance of the macula is the leading theory explaining the propensity for macular hole development following electrocution. The exact cause of other ocular damage following electrocution is less studied but is likely related to a combination of thermal injury and direct cellular effects.
Signs/Symptoms
The signs and symptoms of ocular damage secondary to electrical injuries are directly correlated to the structure that is damaged, and in most cases have the same features as a primary disorder (such as a primary macular hole). For cataract development, the earliest sign following electrocution includes a collection of fine vacuoles beneath the anterior capsule in the midperiphery of the lens. (4) Likewise, the most common type of cataract following electrocution events is anterior subcapsular. (6) Posterior subcapsular and to a lesser extent cortical cataracts have been reported, although nuclear cataracts are rarer (6) Other signs of lens damage are related to the type of cataract that develops and is evident under slit lamp examination. Patients will typically report general cataract symptoms including clouded or blurry vision, difficulty with night vision, and sensitivity to glare.
Retinal damage such as macular holes classically leads to symptoms of decreased central vision with or without metamorphopsia. (21) Signs include a positive Watzke-Allen testing along with corresponding OCT findings. Signs and symptoms of other ocular damage will depend on the structures involved.
Workup and Management
Information about electrocution related eye damage is largely from case reports and retrospective analysis. As such, there are no definitive management guidelines. For patients presenting with electrical shocks to the head and neck or endorsing ocular complaints, early assessment by an ophthalmologist is recommended. (22) In these cases, a complete eye exam including visual acuity, eye pressures, slit lamp examination, and dilated fundus exam are important. If symptoms are indicative of retinal damage, OCT is likely the next step. The preservation of eyelid structure and function is also important to help prevent secondary corneal damage due to desiccation. It should be noted that a complete eye exam can be difficult in these patients as they will likely have other systemic injuries making transportation to an eye clinic difficult.
As the patient becomes stabilized, future management will be guided by the structures injured. Cataract development is the most common finding and in approximately 80% of cases will progress and require surgical intervention with phacoemulsification and IOL implantation. (5, 24) Historically, cataract development was believed to either be immediate or delayed following a variable latency period with two to six months being the most common time until diagnosis though more than a year had also been reported. (5,13,25) A newer retrospective cohort study disputed the delayed development of cataracts following electrocution. (26) However, patients are still typically followed with frequent eye exams.
There is less information available about the management of macular holes in electrical injuries. As in this case, macular holes have been noted to spontaneously resolve following a period of watchful waiting. In one study, the majority of patients with macular holes following lightning strikes were managed conservatively. (27) If no resolution is noted following conservative management over a couple of months, surgical intervention is indicated, likely including PPV.
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS AND SYMPTOMS
|
PATHOPHYSIOLOGY
|
TREATMENT/MANAGEMENT
|
Heinzman Z, Trejo J, Silverman JIM, Haugsdal JM. Electrocution Induced Cataracts and Macular Hole. EyeRounds.org. April 16, 2024. Available from https://EyeRounds.org/cases/357-electrocution-induced-cataract.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links