INITIAL PRESENTATION
Chief Complaint: Evaluation of a choroidal lesion in the left eye
History of Present Illness:
A 95-year-old woman with a medical history of type 2 diabetes, hypertension, and exudative age-related macular degeneration (AMD) presented for evaluation of a choroidal lesion in the left eye. An elevated inferotemporal lesion was first observed by her local ophthalmologist five weeks prior, prompting referral for further evaluation. Review of prior imaging showed the lesion was present eight months earlier but had since developed a darker central component. The patient denied acute vision changes but reported ongoing light sensitivity and difficulty reading related to her AMD. She had not required intravitreal injections in several months.
Past Ocular History:
Past Medical History:
Medications:
Allergies:
Family History:
Social History:
Review of Systems:
OCULAR EXAMINATION
| OD | OS | |
|---|---|---|
| Disc | Normal | Normal |
| Cup-to-disc ratio | 0.10 | 0.2 |
| Macula | Geographic atrophy involving the fovea, no subretinal hemorrhage or subretinal fluid, rare microaneurysms | Geographic atrophy involving the fovea, no subretinal hemorrhage or subretinal fluid, dot-and-blot hemorrhages in the superior macula |
| Vessels | Normal | Normal |
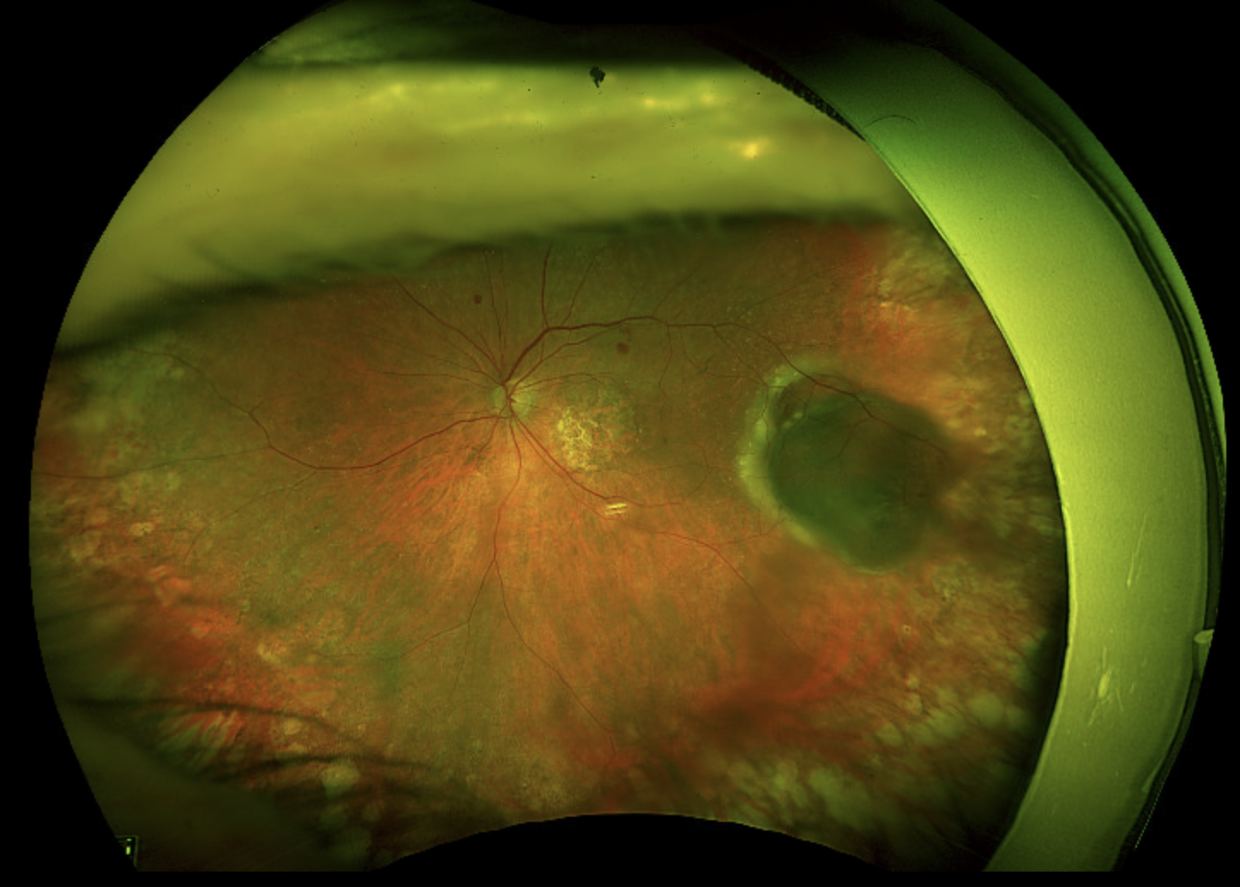
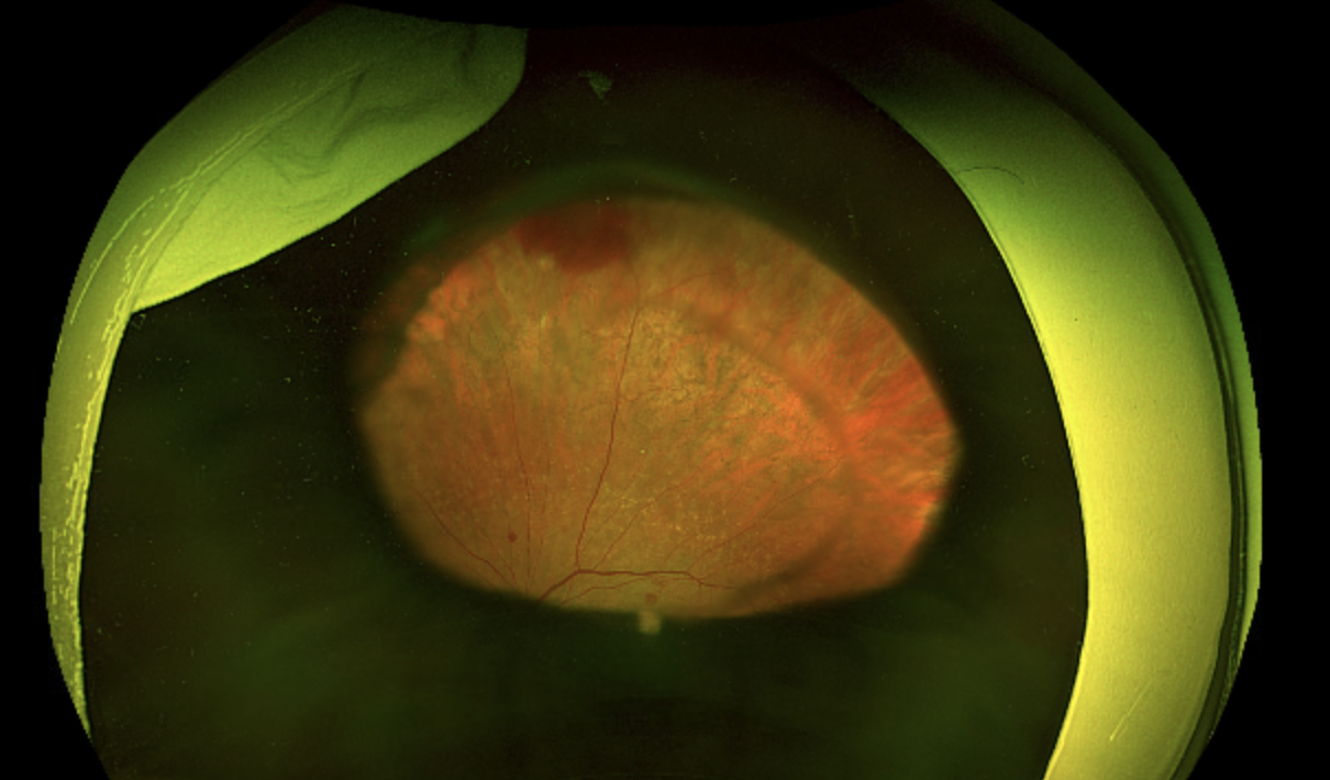
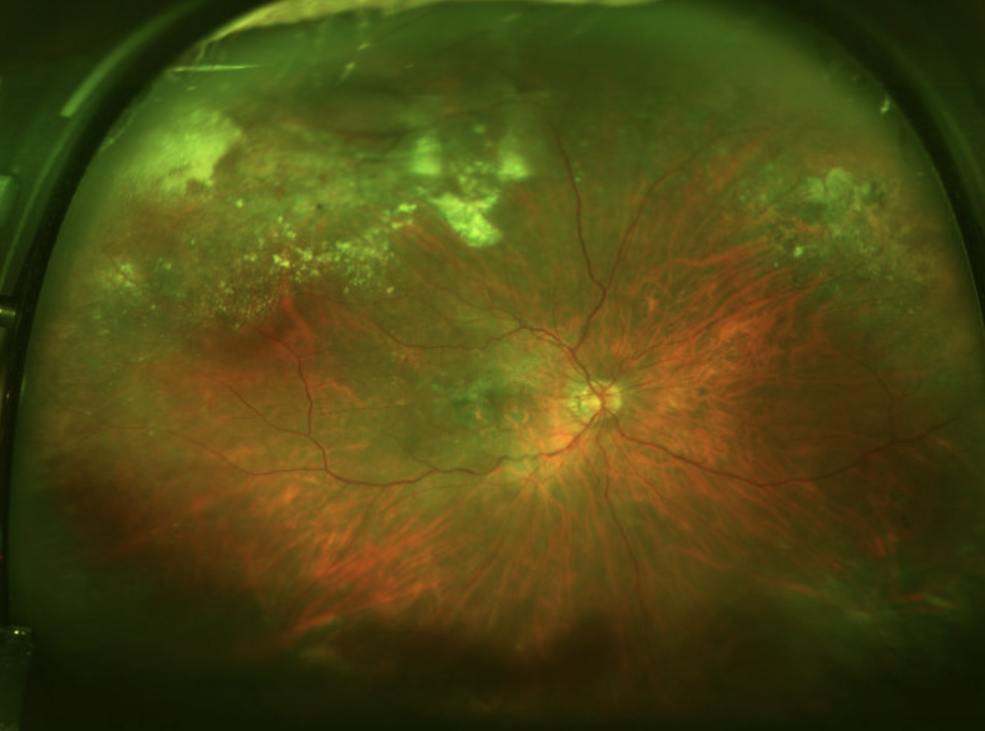
| Periphery | Extramacular drusen and extensive chorioretinal atrophy anterior to the equator, nearly 360 degrees | 7 x 7 x 3.6 mm semi-translucent, sharply-demarcated lesion in the temporal mid-periphery with areas of dark hemorrhage, bordered nasally by lipid exudates, extensive chorioretinal atrophy anterior to the equator, nearly 360 degrees, few additional intraretinal hemorrhages |
Optical Coherence Tomography (OCT) – Macula:
Color Fundus Photography:
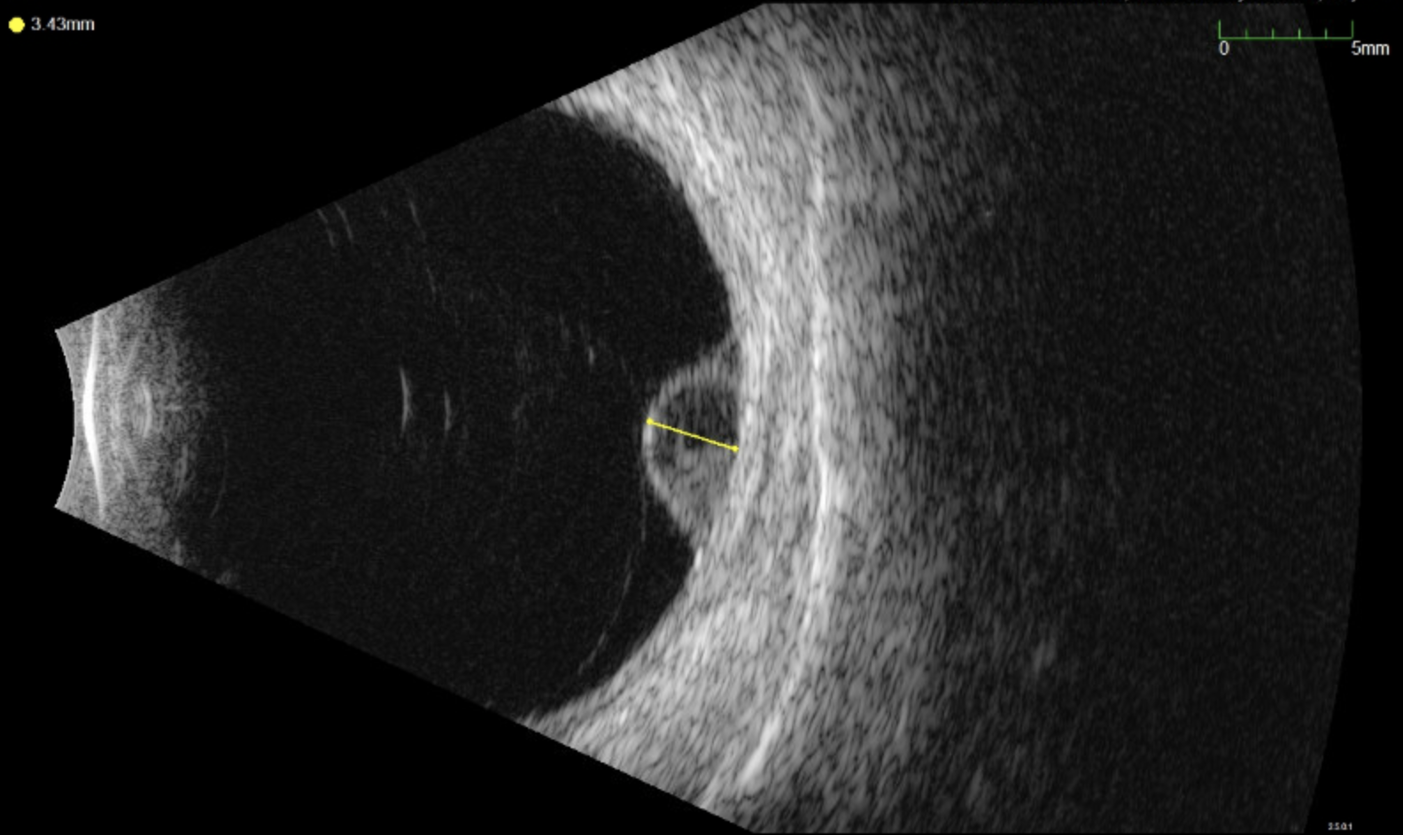
Standardized Ocular Echography – OS:
DIFFERENTIAL DIAGNOSIS:
CLINICAL COURSE
The diagnosis of PEHCR was supported by the patient’s age, female gender, history of hypertension and anticoagulation, absence of vascular polyps, and the presence of bilateral peripheral chorioretinal atrophy. Based on the exam and imaging findings of a dome-shaped RPE elevation with irregular, layered opacities and lack of intrinsic vascularity, a hemorrhagic PED was diagnosed in the setting of PEHCR. FA was deferred given the patient’s age and findings supporting the diagnosis of hemorrhagic PED.
Given the lesion’s peripheral location and visual stability, observation was recommended. The patient was advised to continue AREDS vitamins and maintain glycemic control, with follow-up arranged with her local ophthalmologist in 3-4 months. Should the lesion show signs of increased hemorrhage or exudation threatening the macula, intravitreal anti-VEGF therapy may be considered.
DIAGNOSIS: Hemorrhagic retinal pigment epithelial detachment of the left eye in the setting of PEHCR-spectrum disease
DISCUSSION
PEHCR was first described in detail by W.H. Annesley in 1980, who recognized it as a distinct peripheral retinal condition, differentiated by its temporal peripheral location, hemorrhagic and exudative features, and tendency toward spontaneous regression (1). He also proposed that systemic hypertension may contribute to subretinal hemorrhage, linking PEHCR to broader vascular disease (1). Since then, a growing body of literature has provided insights into this condition’s clinical presentation, imaging characteristics, and outcomes (2,3). PEHCR is often misdiagnosed due to its resemblance to other peripheral retinal lesions, particularly choroidal melanoma, making familiarity with its imaging features essential (3).
Epidemiology
PEHCR is most frequently reported in White patients, typically presenting between 70 and 80 years of age, with a slight female predominance (60%-70%) (2,3). Hypertension is the strongest associated risk factor (3). Systemic anticoagulants and antiplatelet medications are frequently reported in affected individuals, but this may reflect coexisting vascular comorbidities rather than a direct causative role (2-4). The true incidence of PEHCR is unknown, though it is considered rare. The most extensive series described 173 affected eyes in 154 patients over 31 years at a tertiary center (3).
Pathophysiology
PEHCR’s pathophysiology remains largely unclear. Although it shares some features with AMD and PCV, such as hemorrhage, exudation, macular drusen, and RPE changes, its exclusive peripheral distribution and lack of direct macular involvement in most cases support its distinction as a separate entity (3,5). However, others argue that PEHCR may represent a peripheral variant of PCV. This is supported primarily by overlapping indocyanine green angiography (ICGA) findings, including abnormal choroidal vasculature and polyp-like telangiectasias (6,7). A study using enhanced-depth imaging OCT proposed that PEHCR may be part of the pachychoroid spectrum, as it found increased choroidal thickness, dilated outer choroidal vessels, and attenuation of the choriocapillaris in eyes with PEHCR; all of these findings are considered hallmarks of pachychoroid disease (8).
Clinical Presentation
PEHCR is asymptomatic in up to 60% of cases (3,4,9). When symptoms are present, visual loss is most common (62.7%), followed by floaters (9.8%) and photopsias (3.9%) (3). More rarely, patients have reported metamorphopsia and visual field defects (3,4). In severe cases, angle closure due to extensive hemorrhage can cause pain (3). Vision loss is typically secondary to vitreous or subretinal hemorrhage, exudates, or macular fibrosis, with best-corrected visual acuity (BCVA) at presentation typically ranging from 20/40 to 20/100 (3,10). However, one-fifth of patients may present with BCVA worse than 20/200 (3). Lesions are most commonly located temporally between the equator and ora serrata, appearing as elevated hemorrhages or PEDs, often mimicking neoplasms (3,9,11). Associated findings include subretinal fluid, serous PEDs, lipid exudation, subretinal fibrosis, RPE hyperplasia or atrophy, and vitreous hemorrhage (3,5). Additionally, macular findings such as drusen and RPE changes are observed in up to two-thirds of cases (3,8). PEHCR can present unilaterally or bilaterally, with bilateral involvement in 30% of cases at diagnosis (3,4).
Diagnosis
Diagnosis is made through clinical evaluation and multimodal imaging, including color fundus photography, FA, ICGA, and OCT (3,9,11). The primary differential diagnosis is often choroidal melanoma, which has distinct management and prognostic implications (3,5). B-scan ultrasonography can show dome-shaped masses with variable echogenicity and internal reflectivity, but notably no choroidal excavation or intrinsic vascularity that can be seen in choroidal melanomas (3,5).
FA may show blockage due to subretinal hemorrhage, sub-RPE hemorrhage, or RPE hyperplasia, as well as peripheral hyperfluorescence and window defects due to RPE atrophy (3,9). Though choroidal neovascularization is rare in PEHCR, ICGA may show a pathologic choroidal network leakage (6,7). Vitreous hemorrhage, when present, typically arises from peripheral subretinal or sub-RPE hemorrhages that rupture through the retina into the vitreous cavity (3,5). This can occur even without classic choroidal neovascular membrane, likely due to fragile or abnormal peripheral choroidal vessels, such as in polypoidal lesions (7).
OCT is useful for detecting subretinal fluid or PEDs, but direct imaging of peripheral lesions can be challenging. Macular OCT may show extensions of subretinal fluid, exudates, or macular fibrosis (10). Since PEHCR lesions are often located anterior to the equator, widefield imaging is valuable for diagnosing and monitoring PEHCR lesions (11).
Differential Diagnosis
Patients with PEHCR lesions are often referred to rule out choroidal melanoma when there is associated subretinal hemorrhage/hemorrhagic PED that can mimic the clinical appearance of a choroidal melanoma (3,5). However, clinical features and multimodal imaging can help to distinguish PECHR from choroidal melanoma, although none of these features are pathognomonic for either condition (3,5). PEHCR is more common in older individuals with a slight female bias, while choroidal melanoma presents over a broader range with a slight male predominance (3,5). PEHCR can present bilaterally in up to 30% of cases, which is exceedingly rare in choroidal melanoma (3). Additionally, while PEHCR lesions are typically located between the equator and ora serrata, choroidal melanoma can be located anywhere in the uvea (3,5).
On ultrasound, the choroid underlying a PEHCR lesion is usually normal, although there can be a clot-retraction cleft separating the subretinal or sub-RPE clot from the underlying choroid (5). In contrast, a mushroom-like shape and echographic intrinsic vascularity suggest choroidal melanoma (3,5).
Management
There is no standard treatment for PEHCR, and the body of literature regarding management is comprised of expert opinion articles and case series. Observation is appropriate for stable peripheral lesions, given that most PECHR lesions resolve spontaneously (3,9). RPE atrophy, hyperplasia, and fibrosis are commonly seen following lesion regression. However, aggressive lesions can lead to significant peripheral vision loss and macular involvement (9, 11). Treatment options for progressive lesions include intravitreal anti-VEGF therapy, photodynamic therapy, laser photocoagulation, and cryotherapy (3,11). Anti-VEGF therapy is the most commonly used treatment, showing favorable outcomes in high-risk eyes with vision- or macular-threatening disease (10). Vitrectomy is considered for non-clearing vitreous hemorrhage (9). Surveillance is recommended for lesion recurrence and progression (3).
In a large case series, the mean final BCVA ranged from 20/40 to 20/200 at mean follow-up periods of more than two years (9-11). Vitrectomy for vitreous hemorrhage was the only treatment associated with statistically significant improvements in visual acuity (9).
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
MANAGEMENT
|
Jennisch M, Wang C, Binkley EM. Peripheral Exudative Hemorrhagic Chorioretinopathy (PEHCR). EyeRounds.org. September 12, 2025. Available from https://EyeRounds.org/cases/368-PEHCR.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links