INITIAL PRESENTATION
Chief Complaint: Right eye tearing
History of Present Illness:
A 5-year-old girl presented to the UIHC pediatric ophthalmology clinic with excessive tearing of the right eye. The parents reported frequent tearing and clear discharge with dried discharge noted upon awakening since infancy. At 13 months old, the patient was evaluated at a local eye clinic, diagnosed with right nasolacrimal duct obstruction (NLDO), and the family elected to monitor. Since then, the patient continued to have watering from the right eye and noted that the skin sometimes became red and irritated.
The family had no concerns regarding eye crossing or drifting.
Past Ocular History:
Past Medical History:
Medications:
Allergies:
Family History:
Social History:
Review of Systems:
OCULAR EXAMINATION
| OD | OS | |
|---|---|---|
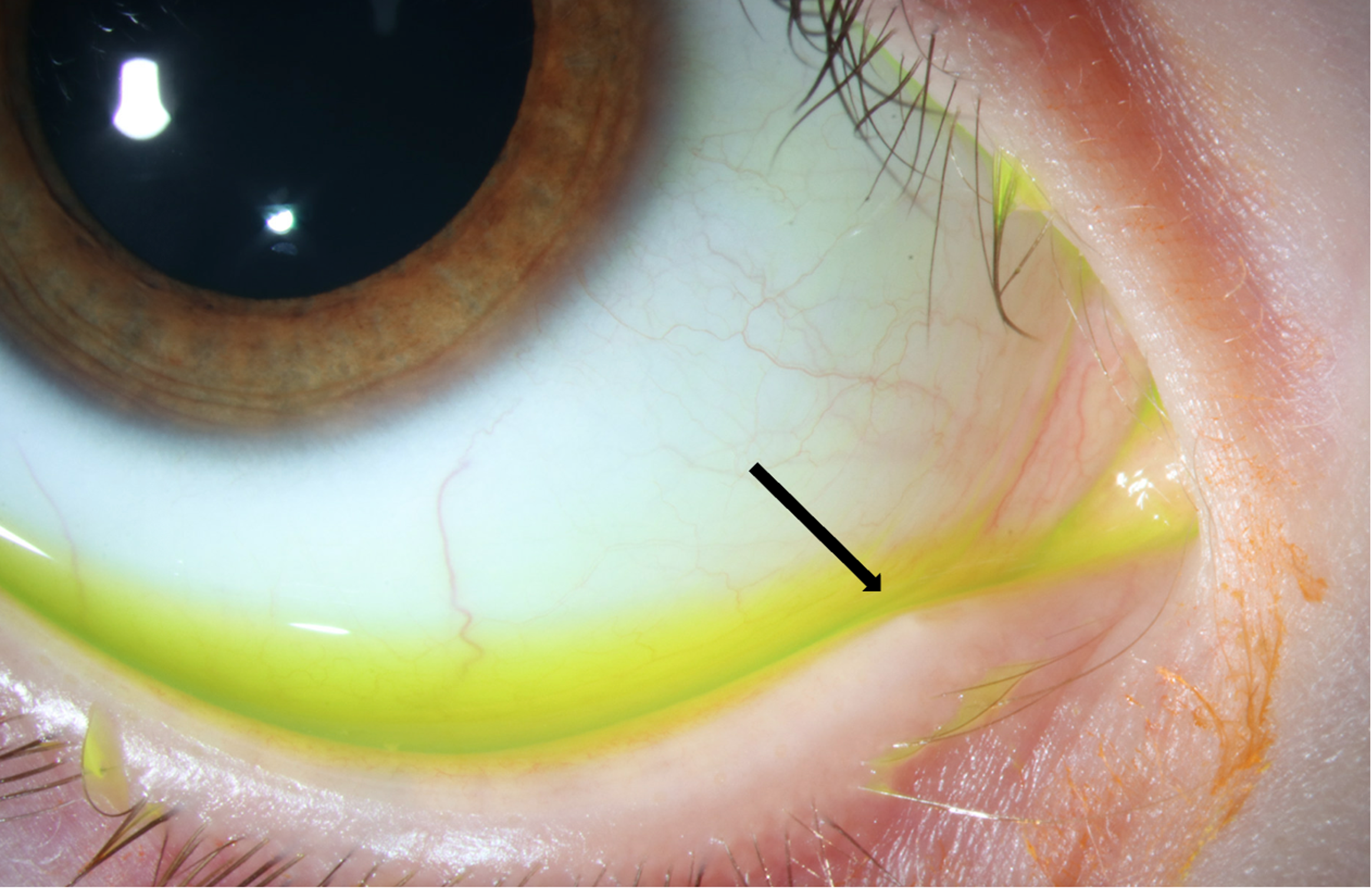
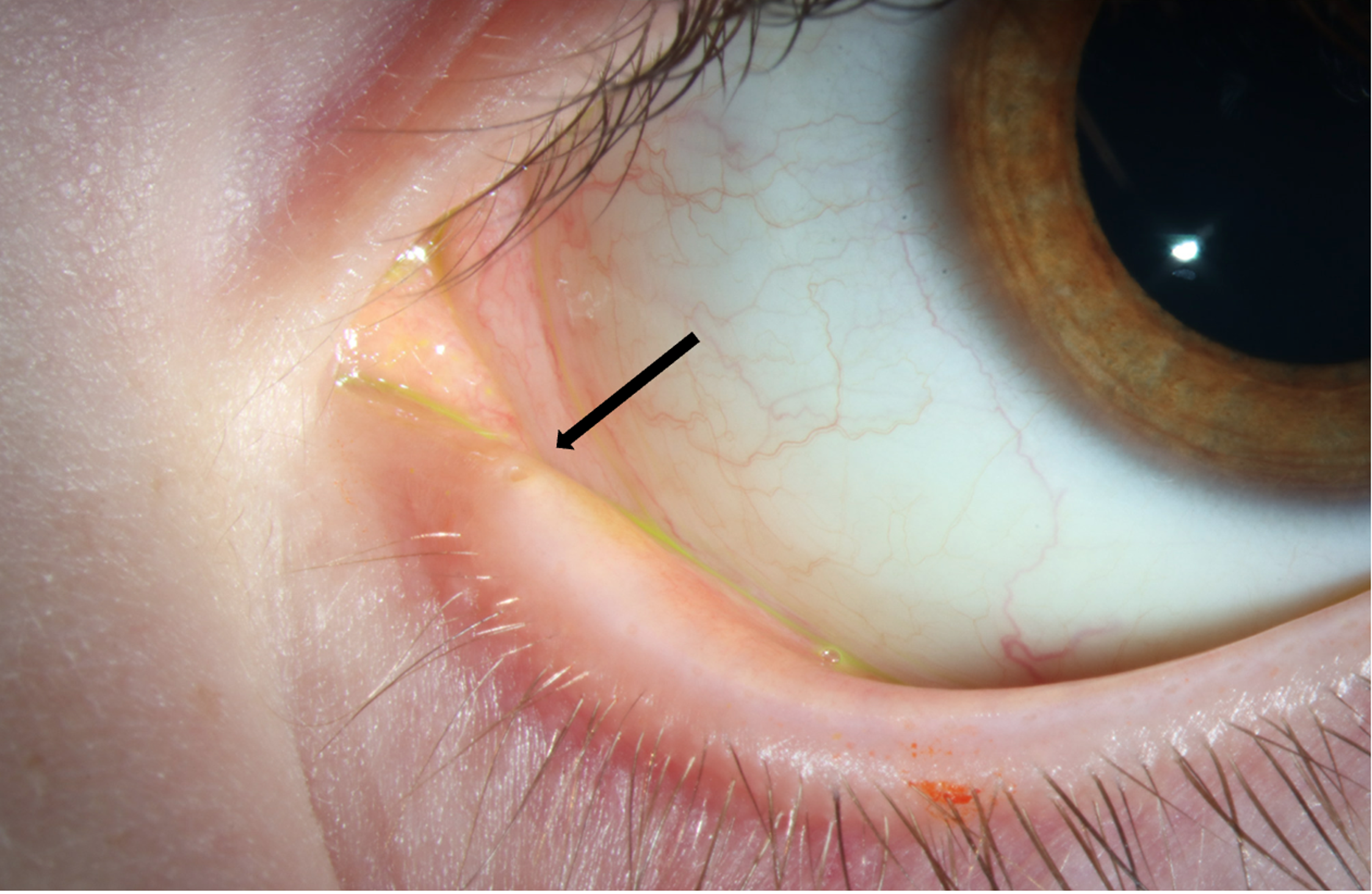
| Lids/Lashes | No punctal opening of right lower lid noted, possibly right upper punctum | Normal, normal puncta on left lower and left upper lids |
| Conjunctiva/Sclera | Clear and quiet, elevated tear lake | Clear and quiet |
| Cornea | Clear | Clear |
| Anterior Chamber | Deep and quiet | Deep and quiet |
| Iris | Normal architecture | Normal architecture |
| Lens | Normal | Normal |
| Vitreous | Normal | Normal |
| OD | OS | |
|---|---|---|
| Disc | Normal | Normal |
| Cup/Disc Ratio | 0.2 | 0.2 |
| Macula | Normal | Normal |
| Vessels | Normal | Normal |
| Periphery | Normal | Normal |
| Sphere | Cylinder | Axis | |
|---|---|---|---|
| Right | +1.50 | +0.25 | 090 |
| Left | +1.25 | +0.25 | 090 |
Lacrimal Exam:
DIFFERENTIAL DIAGNOSIS:
CLINICAL COURSE
The patient was diagnosed with atresia of the right lower punctum and possibly the right upper punctum. The family was informed of treatment options, including continued observation or surgical management. The oculoplastic service was consulted to determine options for surgical management, including punctoplasty or conjunctivodacryocystorhinostomy (CDCR).
DIAGNOSIS: Punctal atresia
DISCUSSION
Excessive tearing or epiphora can be caused by a variety of etiologies. Tears drain through the punctum, canalicular system, lacrimal sac, and nasolacrimal duct.(1) The lacrimal system originates from a cord of ectodermal tissue around the seventh week of gestation.(1) The cord then canalizes, which occurs simultaneously across the entire lacrimal system and is generally complete by birth.(1) Obstruction or improper development of any of these structures can cause tearing.(2) For context, the most common type of tearing in infancy is caused by a membrane at the valve of Hasner, under the inferior turbinate of the nose, causing obstruction at the distal end of the nasolacrimal duct. Immediately after birth, the lacrimal gland is small and does not function fully until about six weeks of life. Thus, in the setting of tear outflow obstruction, an excess of tears is not typically noticed until six weeks or later.(3)
Upper lacrimal system dysgenesis (punctal or canalicular) can vary in severity. In minor cases, the punctal opening is merely covered by a thin layer of tissue, which allows for more conservative treatment, detailed below. In more severe cases, in which there is agenesis of both the punctum and the canalicular system, more invasive surgical approaches are necessary.(4)
The mechanism behind punctal atresia occurs during embryological development. Thus, the absence of the punctum is present from birth. Most cases are considered sporadic, with a minority occurring as a symptom of an underlying syndrome.(5) Syndromes known to present with punctal atresia include CHARGE syndrome, neurofibromatosis type 1, 22q11.2 deletion syndrome, and lacrimo-auriculo-dento-digital (LADD) syndrome.(6-8)
The most common symptom associated with agenesis or atresia of the punctum is excessive tearing, also known as epiphora. Eye discharge, crusting, and in some cases, irritation of the skin around the eye, may also be present. The first step in evaluation of a baby or child with epiphora is a slit lamp examination. Of note, infants and young children with tearing should be evaluated for congenital glaucoma with intraocular pressure measurement, and assessment for corneal clouding. Clinical signs that may increase the suspicion for punctal atresia include the presence of eyelashes medial to the punctum, absence of a dimple in the area of the punctum, or eyelid tags.(9)
A dye disappearance test can be useful in characterizing tear drainage.(10) This test is done by putting fluorescein drops in each eye, waiting five minutes, and then grading how much fluorescein remains in each eye.(10) A positive dye disappearance suggests abnormal drainage of the tears through the lacrimal system and may be a sign of obstruction, agenesis or dysgenesis of a portion of the system.
If punctal involvement is suspected, it is important to distinguish between punctal stenosis or occlusion and true punctal atresia to determine the appropriate course of management. It has been anecdotally reported that the presence of a dimple overlying the punctum increases the likelihood of the presence of a patent canalicular system. Although rare in a childhood presentation, a history of trachoma or HSV infection, trauma to the canaliculi or puncta, or even the use of topical netarsudil for glaucoma treatment may increase the chances of punctal stenosis.(11,12)
In an uncooperative patient, an exam under anesthesia (EUA) may be performed to adequately assess the degree of dysgenesis or agenesis of the lacrimal system. If there is a dimple in the area of the punctum, probing can be attempted under anesthesia to assess if there is a membrane overlying the punctum and gauge if the canaliculi are intact. A dacryocystogram, an imaging technique to view contrast in the lacrimal system, is another option in the assessment of patients with epiphora to assess the patency of the tear drainage system.(13,14) However, a dacryocystogram can only be used in patients with at least one patent punctum – necessary to inject the contrast - and may not be useful in a patient with true punctal atresia of the upper and lower puncta.
For patients who are asymptomatic or have minimal symptoms, observation alone may be preferred. For symptomatic patients with punctal veil overlying an otherwise intact lacrimal drainage system, initial management consists of puncture and dilation(13) performed under anesthesia in children. If a stenotic punctum is found, trephination may be attempted to create a wider opening. If there is no dimple present, options include using a needle or cutting down the area in an attempt to create an opening.
In cases of true punctal atresia, patients may require a conjunctivodacryocystorhinostomy (CDCR) with Jones tube placement, which is a more invasive approach. A CDCR involves creating a fistula between the medial commissural conjunctiva into the nasal cavity with a tube placed to maintain patency.(15,16)
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS AND SYMPTOMS
|
ASSESSMENT
|
TREATMENT/MANAGEMENT
|
DiGioia ON, Pham CM, Kemp PS. Punctal Atresia. EyeRounds.org. September 11, 2025. Available from https://EyeRounds.org/cases/373-punctal-atresia.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links