INITIAL PRESENTATION
Chief Complaint: Severe bilateral vision loss
History of Present Illness:
The patient is a 62-year-old female with a history of metastatic small cell lung carcinoma (SCLC) to the brain status post radiation and chemotherapy urgently referred by hematology-oncology for bilateral subacute vision loss. Following her diagnosis of SCLC, the patient received whole brain radiation (30 Gy in 10 fractions) over the course of two weeks. Nine months after initial diagnosis of SCLC during her 10th cycle of chemotherapy with Carboplatin/Etoposide/Durvalumab and Ceralasertib, she began to complain of intermittent peripheral foggy vision. Local eye examination revealed visual acuity of 20/400 OD and 20/100 OS without objective pathology on eye examination nor on brain MRI. One month later, she complained of progressive visual loss, with reports of foggy vision, especially in peripheral vision. Her chemotherapy was held, and she was urgently referred to neuro-ophthalmology. The patient denied headaches, double vision, flashes or floaters, or trauma to her head or face prior to her vision loss. She also denied scalp tenderness or jaw claudication.
Past Ocular History:
Past Medical History:
Past Surgical History:
Medications:
Allergies:
Family History:
Social History:
Review of Systems:
OCULAR EXAMINATION
| OD | OS | |
|---|---|---|
| Lids/lashes | Dermatochalasis, meibomian gland dysfunction | Dermatochalasis, meibomian gland dysfunction |
| Conjunctiva/sclera | White, quiet | Small ~3.1mm flat nasal nevus without vascularity |
| Cornea | Clear | Clear |
| Anterior chamber | Deep and quiet | Deep and quiet |
| Iris | Normal architecture | Normal architecture |
| Lens | Nuclear and cortical cataracts | Nuclear and cortical cataracts |
| Anterior vitreous | Normal | Normal |
| OD | OS | |
|---|---|---|
| Vitreous | Normal | Posterior vitreous detachment |
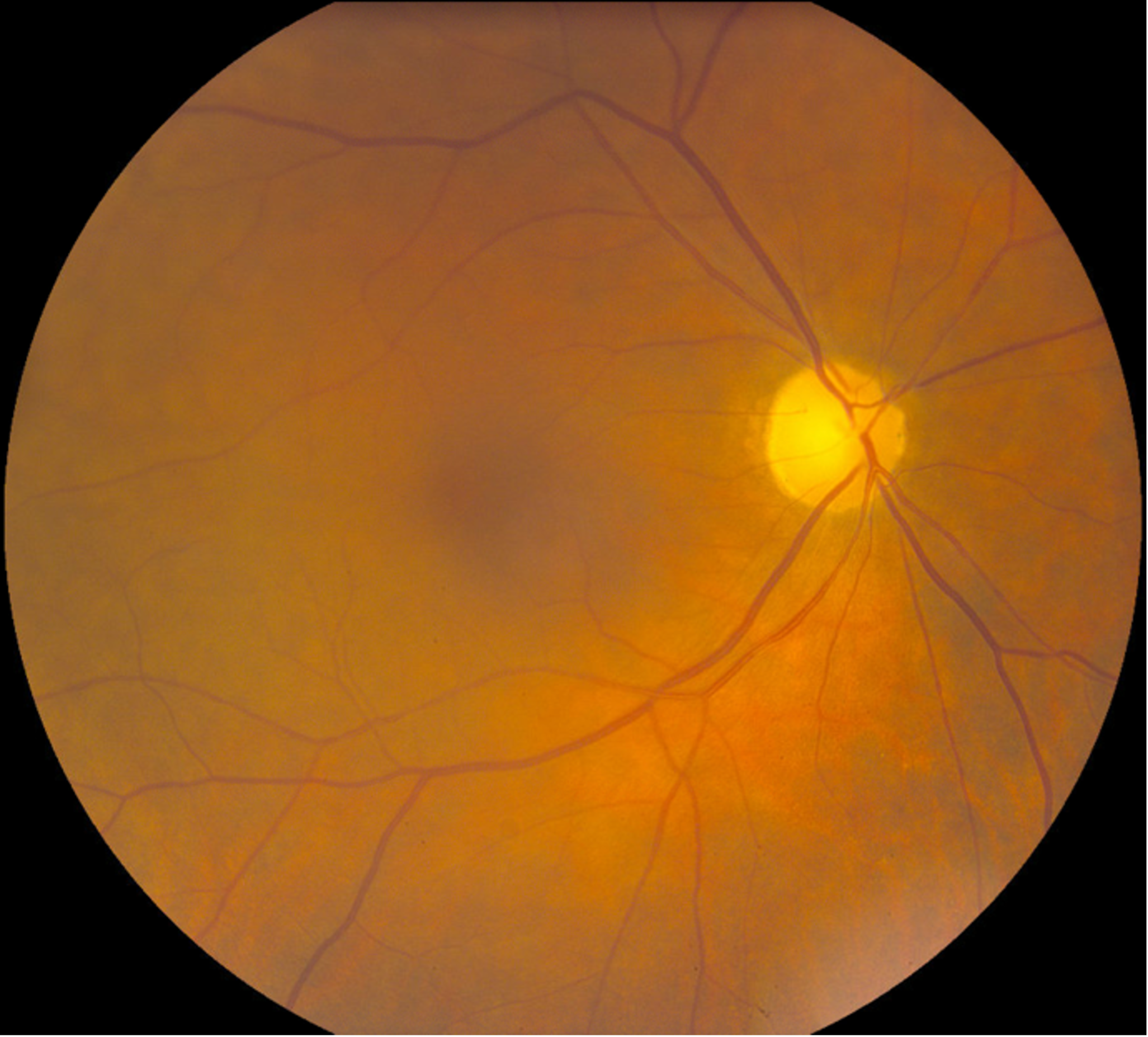
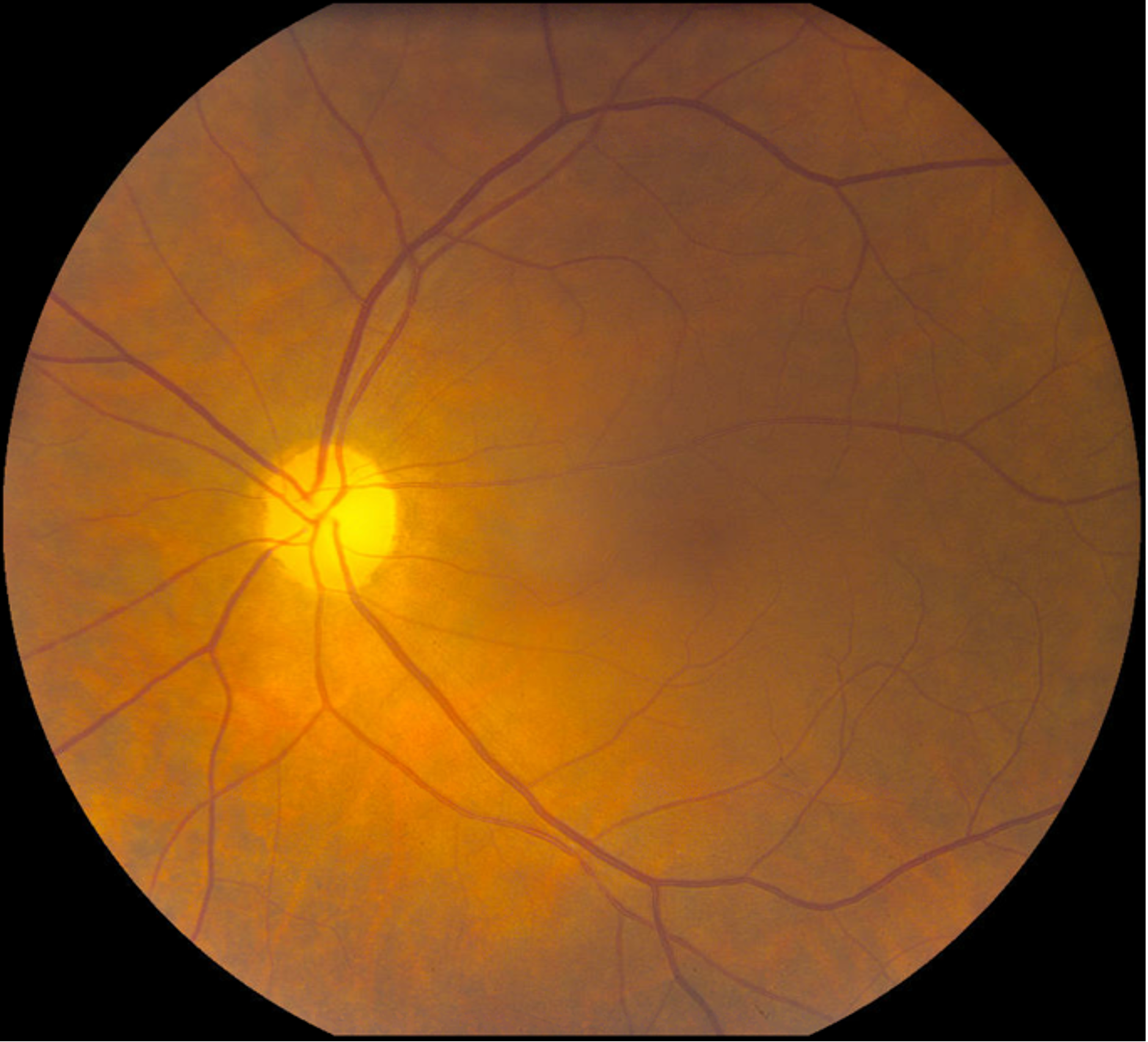
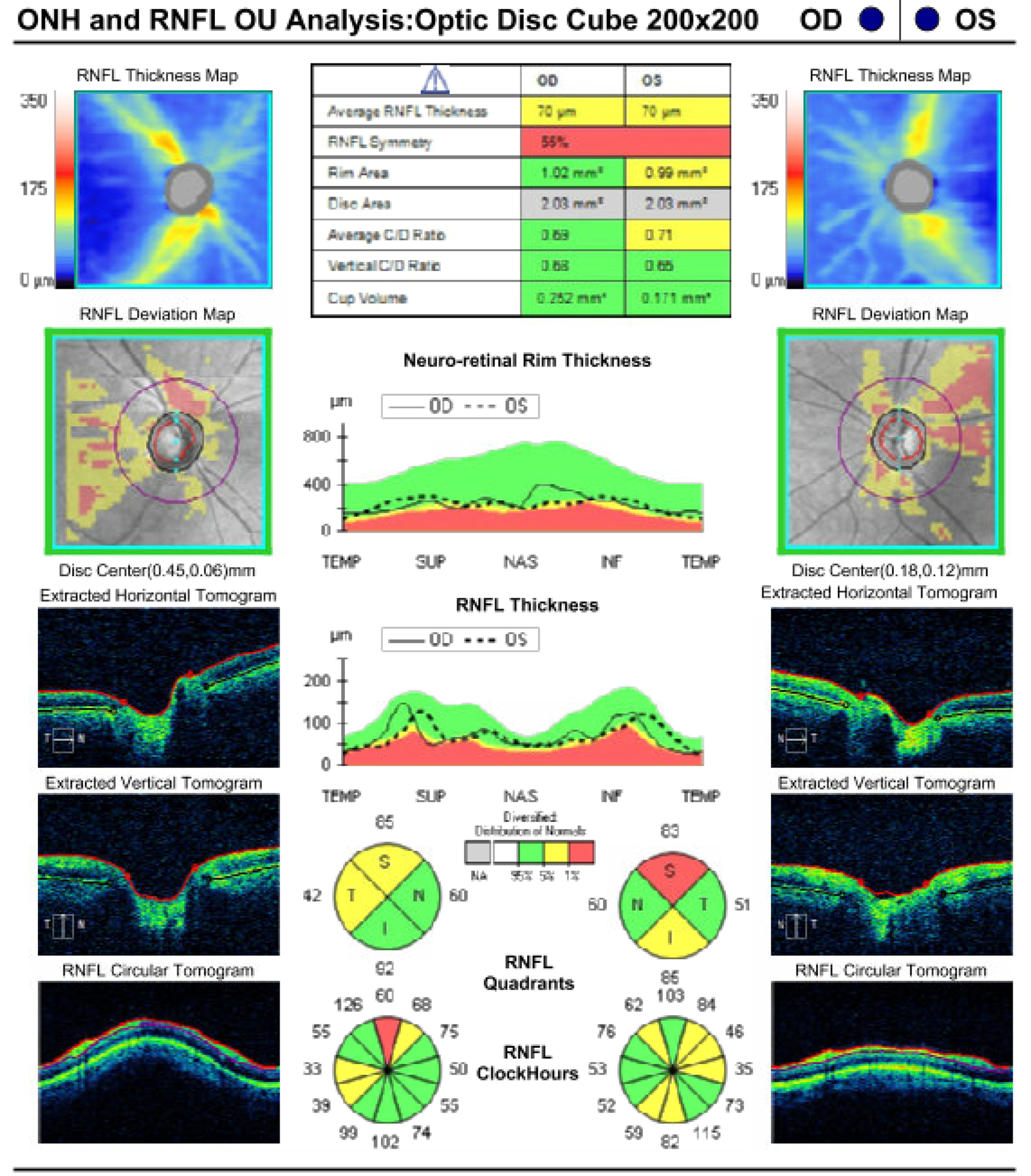
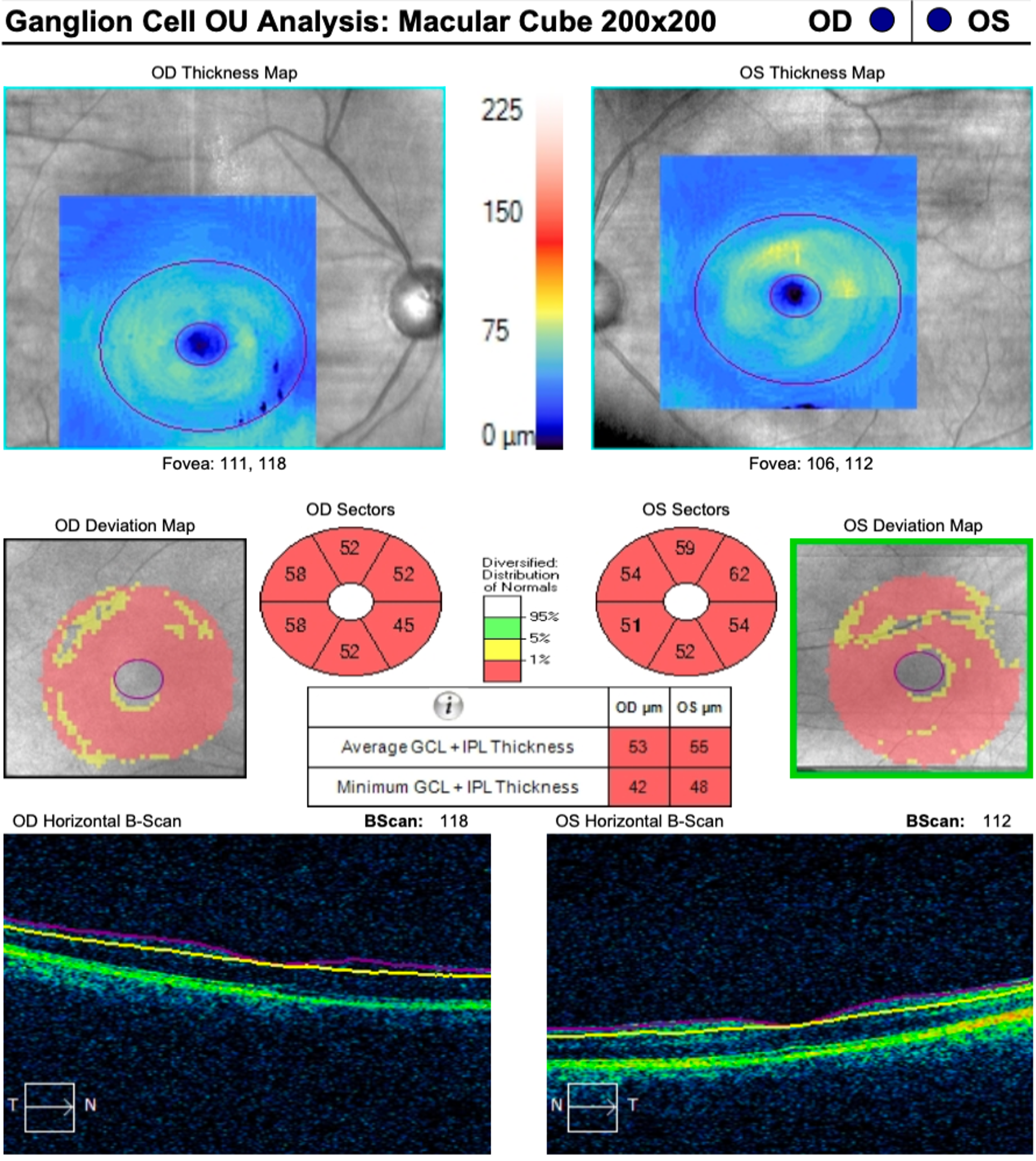
| Disc | Marked diffuse pallor | Marked diffuse pallor |
| Cup-to-disc (C/D) ratio | 0.3 | 0.3 |
| Periphery | Flat reticular pigmentary changes | Flat reticular pigmentary changes, rare drusen |
DIFFERENTIAL DIAGNOSIS:
DIAGNOSIS: Radiation optic neuropathy
CLINICAL COURSE
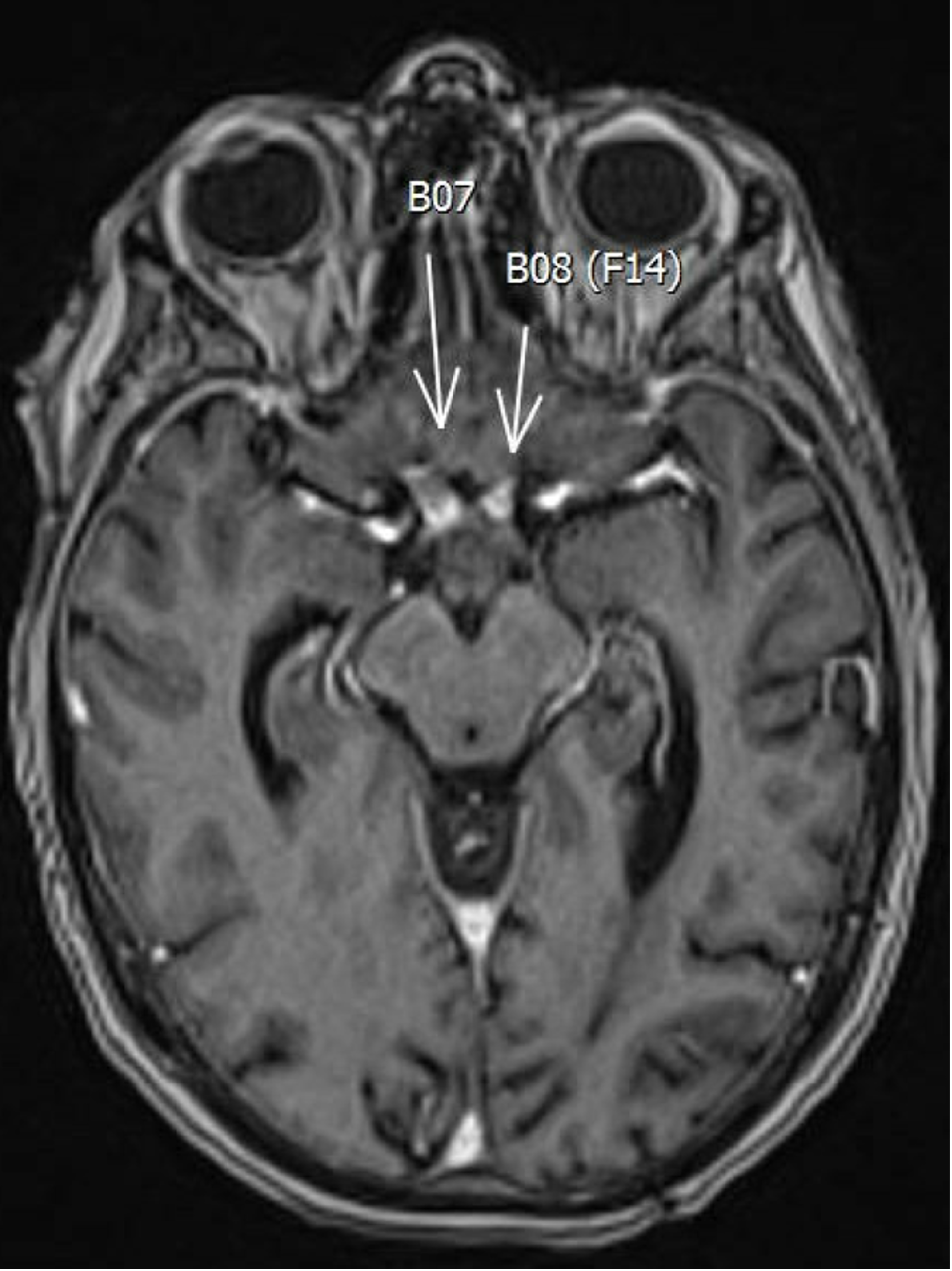
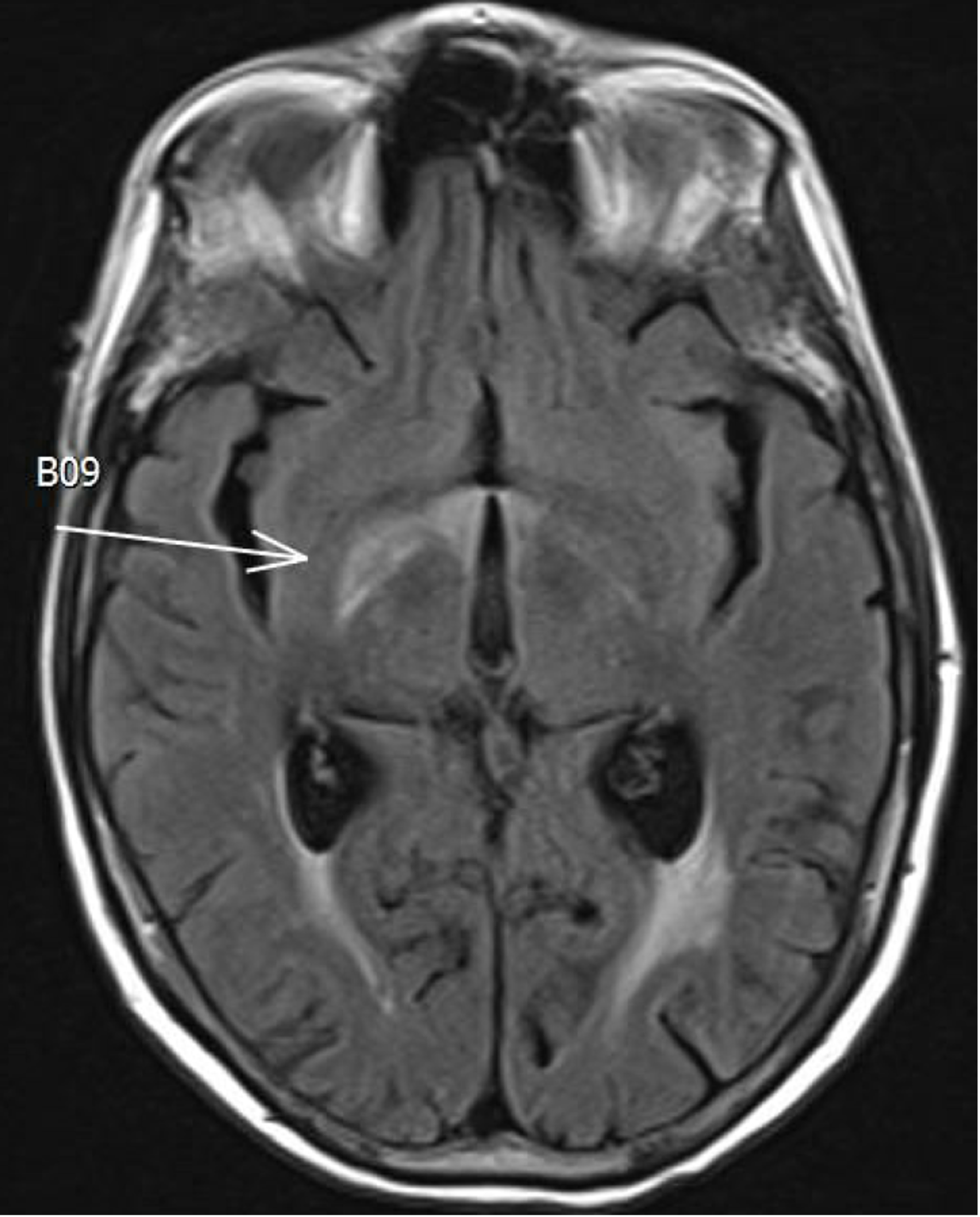
Radiation-induced optic neuropathy was considered the most likely cause given the painless subacute catastrophic vision loss in the setting of a prior history of brain radiation. Checkpoint inhibitor optic neuropathy was considered but deemed less likely since she was not on a medication known to cause subacute and catastrophic visual loss. Leptomeningeal spread and focal metastasis were similarly considered but the dedicated orbital MRI images and cerebrospinal fluid studies were normal.
The patient was admitted with a presumed diagnosis of radiation-induced optic neuropathy and was started on IV methylprednisolone and IV bevacizumab. The patient also received two rounds of abatacept and IVIG In the event the visual loss was due to checkpoint inhibitor induced optic neuropathy. Following discharge, the patient was continued on IV bevacizumab and steroid treatment. Despite continued treatment, the patient’s vision failed to recover, and her vision remained stable at no light perception OD and light perception OS one year after her initial presentation.
DISCUSSION
Radiation-induced optic neuropathy (RION) is a devastating delayed complication of radiation therapy. It is characterized by profound, severe, and painless vision loss that occurs in the setting of previous radiation administration to the visual pathways. Other diagnoses, including checkpoint inhibitor optic neuropathy due to her treatment with durvalumab and ceralasertib, and metastatic involvement of her optic nerves, were also initially suspected. There are no current reports of optic nerve complications due to durvalumab, but related anti-programmed death-ligand 1 (PD-L1) and anti-programmed cell death protein-1 (PD-1) antibodies have been associated with a wide variety of neuro-ophthalmic complications including optic neuritis, neuroretinitis, giant cell arteritis, myasthenia gravis, thyroid-like eye disease, orbital myositis, general myositis with ptosis, internuclear ophthalmoplegia, opsoclonus-myoclonus-ataxia syndrome, and oculomotor nerve palsy. (1,2,3,4,5) Basic science reports have found ceralasertib make fibroblasts more radiosensitive but no complications related to visual function have been reported.(6) In addition, catastrophic visual loss is not consistent with checkpoint inhibitor optic neuropathy, and checkpoint inhibitor optic neuropathy is highly responsive to corticosteroids with or without stopping the checkpoint inhibitor.(1, 2) One study examined the best-corrected visual acuity (BCVA) and visual fields for 16 eyes of 8 patients treated with CTLA-4 and PD-1/PD-L1 checkpoint blockage. All patients had bilateral optic nerve involvement characterized as optic neuropathy, optic neuritis, optic disc edema, or papilledema. Ophthalmic side effects occurred in a median time of less than 3.5 months with 9 eyes having BCVA at presentation of 20/30 or better and 7 having 20/50 or worse (range 20/15 to 20/125). All 16 eyes had improvement of BCVA after corticosteroid treatment. Visual field results were available for 9 patients and were described as altitudinal for 3 patients, arcuate in 4, enlargement of the blind spot in 3, and inferotemporal depression in 1 patient. The average mean deviation at presentation was –9.90 dB and improved to –6.782 dB with treatment.(2)
Although its course has a more rapid progression, severe ocular and orbital toxicity has been reported following intracarotid administration of the combination therapy carboplatin/etoposide. One case report described a patient developing nonpupillary block angle-closure glaucoma within 7 hours of infusion, followed by orbital inflammation, vision loss, proptosis, optic neuropathy, and total external ophthalmoplegia of the eye, which improved after lateral cantholysis and intravenous corticosteroids. Two weeks later, anterior uveitis developed, which responded to corticosteroids. Within two months, vision, motility, and intraocular pressure largely recovered.(7)
Etiology/Epidemiology:
RION is believed to be caused by radiation necrosis of the anterior visual pathway following radiation therapy in amounts greater than 2 Gy in a single dose and 50 Gy cumulatively.(8) The incidence of RION is rare and dependent on the radiation dose and nature of the tissue. Resected adenomas have an occurrence of 0.53%, resected anterior visual pathway meningiomas have a rate of 2.04%, and tumors of the nasopharynx, nasal cavity, and paranasal sinuses result in RION in 8.7 to 9.0% of cases.(9) The latency period ranges from months to years following radiation therapy exposure, depending on the radiation dose, distribution, and nature of the irradiated tissue.(9) Risk factors include age, pre-existing compression of the optic nerve or chiasm by a tumor, concurrent chemotherapy, or previous external beam radiation.(10)
Pathophysiology:
Although not fully understood, the pathophysiology of RION is considered to be delayed radionecrosis which predominately affects the white matter.(10,11) The generation of free radicals damages neuroglial cell progenitors and vascular endothelial tissue, although the primary site cellular injury is debated.(11, 12, 13, 14) Endothelial damage leads to a leaky blood-brain barrier, thus explaining the high signal with gadolinium-enhanced MRI.(13) Ionizing radiation causes somatic mutations in glial progenitor and endothelial cells which impairs their metabolic activity and functioning. Glial damage accumulates and eventually leads to demyelination and neuronal degeneration, while endothelial damage leads to vascular occlusion and necrosis.(15) Although the pathophysiology and its contribution to the latency period of RION is unclear, the result is “3-H tissue”: hypovascular, hypocellular, and hypoxic- with all three contributing to necrosis and vision loss. The hypoxia in this case forms a gradient between normal and radiated tissue which inhibits spontaneous repair. The end-stage pathology is characterized by stenosed and occluded blood vessels, demyelination, and fibrin exudates.(14)
Signs/Symptoms:
RION often presents as sudden, painless, monocular visual loss that is rapidly progressing and irreversible. It commonly begins monocularly, but second eye involvement can follow within months. A relative afferent pupillary defect would be present if there is unilateral or asymmetric damage to the optic nerve. The visual field can show any pattern of optic nerve or chiasmal defects, depending on the location of the damage.(10)
Characteristic findings of RION may be seen on ophthalmoscopic examination, including scattered vascularization, flame hemorrhages in the retina, optic nerve atrophy, and cotton wool spots.(16) The optic nerve head will appear swollen if ischemic demyelination occurs anterior to the lamina cribrosa. Whether swelling of the optic nerve head is present or not, optic nerve atrophy and pallor begin to develop 6-8 weeks after onset.(10)
Testing/Laboratory work-up:
RION is a diagnosis of exclusion, with the most important condition to rule out being a recurrence of the previously treated tumor. MRI is the preferred imaging modality for diagnosis, since CT will often show no abnormalities in patients with RION. Typically for MRI, the unenhanced T1- and T2-weighted images show no abnormality, but the optic nerve will show post-gadolinium enhancement in T1-weighted images with MRI.(10, 17) The characteristic finding of RION is a discrete region of enhancement of the prechiasmatic optic nerve, often accompanied by expansion and T2 hyperintensity in the enhancing segment.(8) The enhancement of the optic nerve is believed to be due to radiation-induced disruption of the blood-brain barrier and accumulation of gadolinium within the nerve.(18) The exact pathogenesis of the optic nerve damage is unknown but microscopic investigation suggests the initial vascular injury results in perivascular inflammation, hyalinization and fibrosis of the vessel walls, loss of endothelium, and ensuing infarction with reactive gliosis.(18) These MRI imaging results can effectively rule out neoplastic infiltrative optic neuropathies since discrete areas of enhancement with expansion or T2 hyperintensity do not typically occur in these cases.(8)
Fluorescein angiography will show filling defects if swelling is present but normal if the optic nerve head appears normal.(10)
In classifying the disease's progression, a clinical grading scale of RION was recently proposed, though is not yet in widespread use, using optical coherence tomography angiography (OCT-A). Vessel area density (VAD) and vessel length fraction (VLF), both of which are decreased in RION, can be detected on OCT-A and used to classify RION into grades 0-4. The grading scale is based on the degree of radial peripapillary capillary plexus (RPCP) changes present throughout the four quadrants. OCT-A findings correlate with best corrected visual acuity measurement (ETDRS score) and may have utility for specialists in assessing the severity and progression of RION.(20)
Treatment/Management:
There is no current universally accepted treatment for RION. Therapeutic approaches, including corticosteroids, anticoagulation, anti-vascular endothelial growth factor (VEGF) antibody therapy, and hyperbaric oxygen (HBO) therapy, have aimed at addressing the inflammatory and vascular toxic mechanisms of RION.
Many of these therapeutic approaches have demonstrated limited to zero efficacy. Corticosteroids have been investigated for the purpose of decreasing edema and demyelination, though they have not been proven beneficial for RION.(21) Systemic anticoagulants have demonstrated beneficial effects in late radiation-induced nervous system injuries, including cranial nerve lesions, cortical lesions, myelopathies, and plexopathies. However, these benefits do not appear to translate to the visual pathways, due to evidence of RION development in patients taking therapeutic doses of warfarin.(21) Hyperbaric oxygen therapy is thought to support angiogenesis and decrease ischemic necrosis in patients with RION, though the current supporting literature is limited and controversial. Several studies support the use of HBO treatment for patients with recent onset of RION. However, the cost of this therapy, along with potential contraindications, complications, and regression of visual function following cessation of treatment may outweigh any potential benefit.(21)
One therapy that has demonstrated benefit for treatment of RION is systemic and intraocular bevacizumab, a monoclonal antibody directed against VEGF. Bevacizumab is thought to decrease capillary leakage and associated edema in RION. The data from current studies demonstrates the potential of bevacizumab to improve visual acuity in certain patients with RION.(21, 22) One case report demonstrated improved visual acuity from no light perception to 20/20, visual fields, and radiographic signs following systemic administration of bevacizumab.(21) In one clinical case series, patients exhibited decreased hemorrhage and optic disc edema, accompanied by some improvement in visual acuity, following intraocular administration of bevacizumab.(21) These case reports indicate the potential that bevacizumab has for the treatment of RION, though there is still a necessity for further research on its efficacy in this population.
EPIDEMIOLOGY OR ETIOLOGY
|
DIAGNOSIS
|
SYMPTOMS/SIGNS
|
TREATMENT/MANAGEMENT
|
Christensen Q, Grimes K, Chun LY, Shepard Z, Chung S, Linton EF. Radiation Optic Neuropathy. EyeRounds.org February 25, 2026. Available from https://EyeRounds.org/cases/374-radiation-optic-neuropathy.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links