Chief Complaint: Watery, red, irritated eyes; left more than right
History of Present Illness: Adult patient presents with 6-day history of watery, irritated eyes noted that the left eye was tearing, slightly blurry, and starting to get red throughout prior to presentation. The eye gradually became increasingly red and irritated over the ensuing 2 days and the patient noted increased crusting in the mornings. There was a mild "scratchy" sensation noted then. Symptoms did not remit with antibiotic drops and eye continued to worsen, with early redness and watery sensation in the contralateral eye as well. Nne week prior to any ocular symptoms, patient had an upper respiratory infection which had subsided spontaneously .
PMH/FHx/POH: No previous ocular or health problems. No eye surgery, trauma, nor contact lens use.
EXAM OCULAR:
 |
|
|
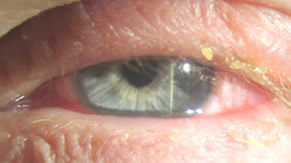
| Crusting on the lashes. | Conjunctival injection with a follicular conjunctivitis. |
|
|
 |
This patient presents with the classic signs and symptoms of conjunctivitis from Adenovirus. There are multiple serotypes of adenovirus, and viral infection has a variety of clinical effects throughout the body. Most commontly, adenovirus can cause a variety of respiratory infections from bronchitis, to croup, to pneumonia. In immunocompromised patients, the respiratory effects can be severe. During World War II, scores of soldiers in crowded environments and under stress developed acute respiratory disease (ARD), later found to be from adenovirus. Adenovirus infection is also responsible for diarrhea in children, acute hemorrhagic cystitis, rashes, and rarely meningoencephalitis. There are over 40 serotypes of adenovirus in subgroups A-F.
In the eye, adenovirus most commonly manifests as a follicular conjunctivitis. Though symptoms may range in severity, a common constellation of signs and symptoms is frequently manifest. Red and irritated conjunctiva is typical of the infection. This is seen clinically as conjunctival injection with folliculitis, especially on the inferior palpepral conjunctiva. Occasionally, pinpoint subconjunctival hemorrhages may develop.
Patients often complain of burning or gritty foreign body sensation. There is usually a watery, mucoid discharge—morning crusting is a common complaint. The lids may become red and edematous. Classically, preauricular lymphadenopathy can be palpated.
Symptoms usually begin and predominate in one eye, and within a few days, have spread to the contralateral eye. A history of antecedent upper respiratory tract infection or close contact with someone with a "red eye" is common.
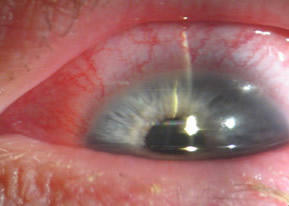
When adenoviral eye infections further involve the cornea, the term epidemic keratoconjunctivitis (EKC) is used. While some argue that this is on a spectrum with simple follicular conjunctivitis, most clinicians use the term EKC when pseudomembranes are present, supeithelial corneal infiltrates develop, or corneal erosions are evident. Patients with EKC may have photophobia and reduced vision long after resolution of the acute infection.
Pharyngoconjunctival fever describes adenoviral conjunctivitis with the additional systemic symptoms of fever, sore throat, and headache. Corneal infiltrates are very rare.
Adenovirus infection is quite contagious, as the virus is transmitted readily in respiratory or ocular secretions, contaminated fomites (including eye droppers and mascara bottles), and even contaminated swimming pools. Frequent handwashing is recommended and care must be taken to avoid contamination to others through towels, make-up, instruments, or other fomites.
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
|
Graff JM. Beaver HA. Adenoviral Conjunctivitis: 38-year-old white female with watery, red, irritated eyes; left more than right. EyeRounds.org. June 14, 2005; Available from: http://www.EyeRounds.org/cases/case28.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links