
Chief Complaint: Irritation of the right eye
A 67-year-old male presents with irritation and "scratchiness" of the right eye. His symptoms have been present for the past 8 months and have been only partially relieved with artificial tears and lubricating ointment at night. He denies any change in visual acuity, purulent ocular discharge, or photophobia.
Past Ocular History: No ocular surgery or trauma
Allergies: Penicillin
Family History: No family history of thyroid eye disease or skin cancer
Review of Systems: Negative
Ocular Motility: Full OD and OS
Pupils: 5 mm in dark → 3 mm in light; brisk reaction to light with no relative afferent pupillary defect (RAPD) OD and OS
Confrontation visual fields: Full to counting fingers OD and OS
OD
OS
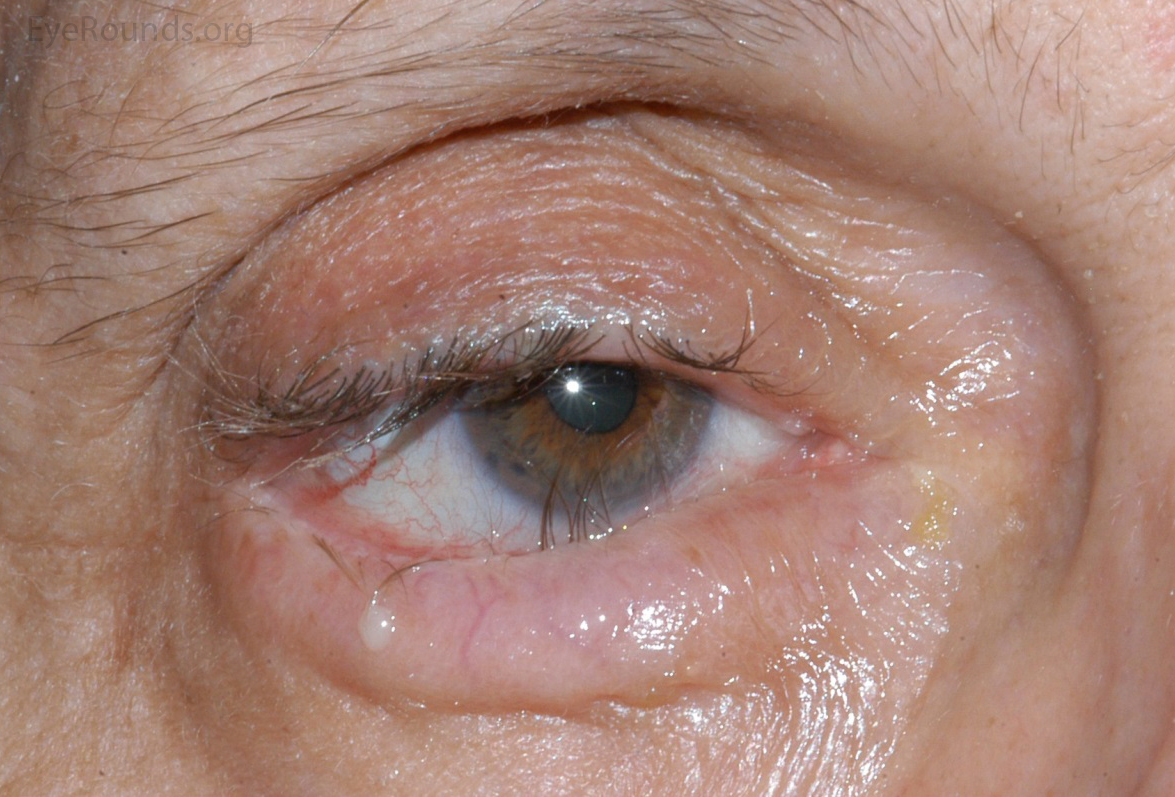
Figure 1: Appearance on presentation—note inward rotation of the lower eyelid margin with misdirected eyelashes abrading the cornea centrally. Also, note the "mounding" of the orbicularis oculi muscle indicative of an over-acting/over-riding muscle and the conjunctival injection
The patient underwent surgical repair consisting of lateral tarsal strip and retractor reinsertion procedures. At the one week post-operative visit, the eyelid margin was positioned appropriately, there was mild post-operative edema and erythema of the lower eyelid, and symptoms of ocular surface irritation were markedly improved. [Figure 2]
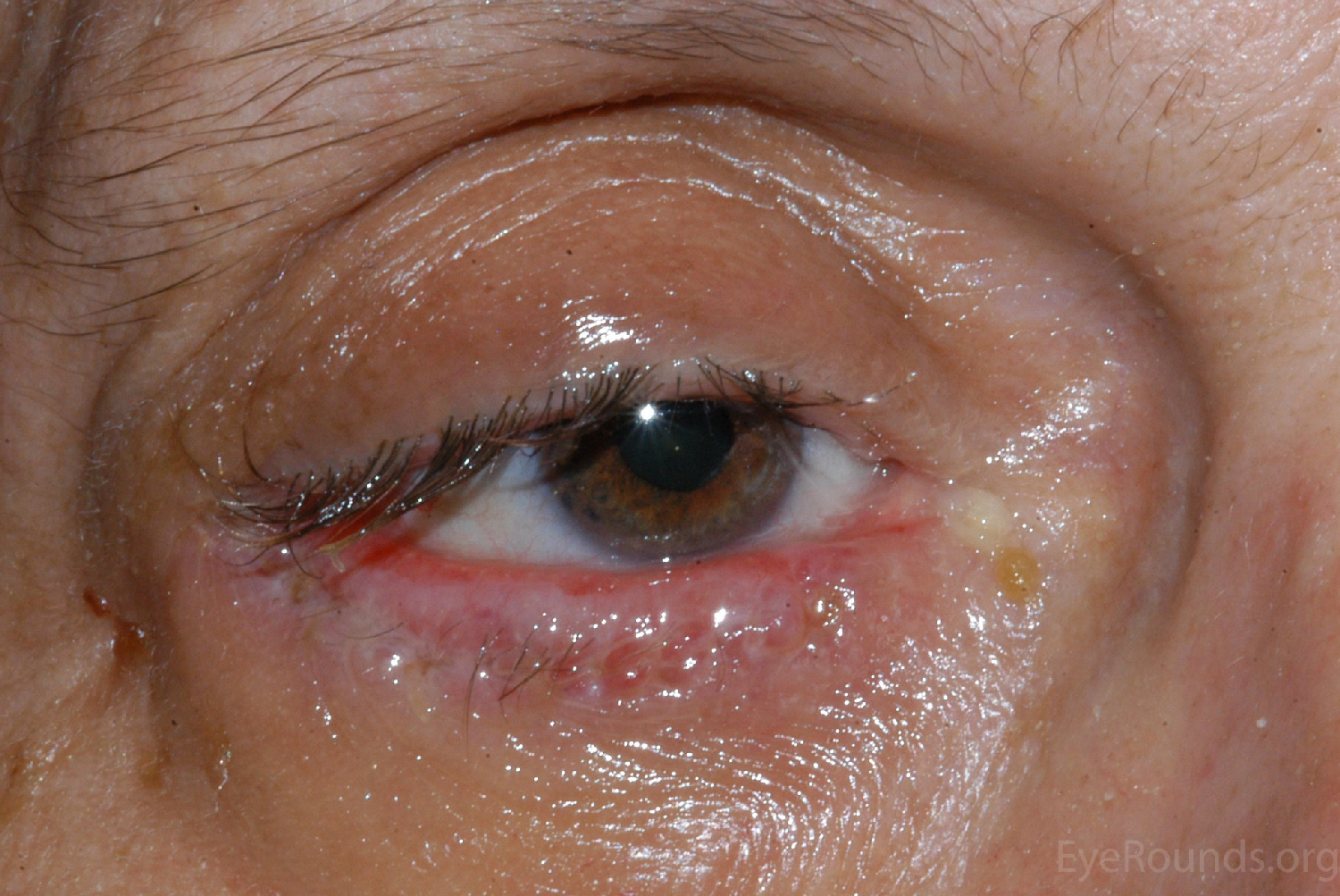
Figure 2: Appearance at the 1 week post-operative visit—note the improved position of the lower eyelid margin and the resulting rotation of the remaining lateral eyelashes. Of note, some medial eyelashes were excised during the retractor reinsertion (subciliary approach) procedure.
Entropion is as an eyelid malposition marked by an inward turning of the eyelid margin. Entropion is categorized based on etiology as involutional, cicatricial, or spastic, with involutional being the most common. The symptoms of entropion are related to abrasive contact between the keratinized skin of the inverted eyelid margin (and associated eyelashes) and the corneal and conjunctival surfaces. Additionally, ocular exposure due to lagophthalmos or incomplete blink can contribute. Patients commonly report ocular irritation, discharge, erythema, and tearing. Signs of ocular irritation are frequently seen on examination, including conjunctival injection, papillary conjunctival reaction, and linear or punctate epithelial erosions with frank corneal epitheliopathy and breakdown manifesting in severe cases.
It is important to distinguish entropion from trichiasis as the treatment for these entities differs. Trichiasis is characterized by an inward rotation of the eyelashes in the setting of a normally-positioned eyelid margin, whereas entropion results in an inward rotation of the eyelashes secondary to an inward turning of the eyelid margin. Epiblepharon is an additional clinical entity that is occasionally confused with entropion. In epiblepharon, a condition most commonly seen in Asian and Native American children, the lower eyelid lashes assume a vertical orientation in the setting of a redundant superior band of orbicularis oculi muscle along the inferonasal portion of the lower eyelid. The posterior eyelid margin itself is in the normal anatomic alignment.
In order to better appreciate the mechanisms behind lower eyelid malposition and the treatments utilized in their correction, an understanding of the relevant anatomy is of benefit. The eyelids can be sub-divided into anterior, posterior, and middle lamellae. In the lower eyelid, above the inferior border of the tarsus, the anterior lamella consists of the skin (including the eyelashes) and orbicularis oculi muscle, whereas the posterior lamella consists of the conjunctiva and tarsus. Inferior to the tarsus, the anterior lamella continues as the skin and orbicularis oculi muscle, the posterior lamella continues as the conjunctiva, and a third lamellae (the "middle" lamella) emerges. The middle lamella consists of the lower eyelid retractors, orbital septum, and lower eyelid fat pads (medial, central, and lateral). When any of these lamellae become shortened or dissociated, eyelid malposition can occur.
Involutional entropion has classically been attributed to the triad of horizontal lower eyelid laxity, dehiscence of the lower eyelid retractors, and an over-riding orbicularis oculi muscle (1,2). Age-related enophthalmos has also been proposed as an etiologic factor although this association has been debated in the literature (3). Additionally, a decreased vertical height of the tarsus has been postulated to be a causal factor in the development of involutional entropion (4).
Horizontal eyelid laxity is caused by age-related stretching of the lateral canthal tendon, with or without involvement of the medial canthal tendon. Horizontal eyelid laxity can be detected by a positive distraction test and/or snap back test. To conduct the eyelid distraction test, the lower eyelid is displaced anteriorly from the globe. An eyelid with normal laxity will not distract more than 8 mm from the globe (5). The snap-back test is performed by displacing the lower eyelid inferiorly. A normal tension eyelid will immediately snap back to place, whereas an eyelid with increased laxity may require one or more blinks before the eyelid resumes its normal appositional location against the globe. Medial canthal tendon laxity can be detected by manual displacement of the inferior punctum laterally. A medial canthal tendon with normal laxity will not permit displacement of the punctum beyond the medial limbus. Disinsertion of the lower eyelid retractors from the inferior border of the tarsus results in vertical laxity, which allows the inferior border of the tarsus to displace anteriorly with a concomitant posterior displacement of the superior tarsus and inward rotation of the lower eyelid margin. Occasionally, a white line of "disinserted" lower eyelid retractors can be viewed through the palpebral conjunctiva. In some patients, the pre-tarsal orbicularis oculi muscle can be seen to roll upward, displacing the eyelid margin against the globe with blinking or forceful eyelid closure. The over-riding of the orbicularis oculi results from a relative imbalance between the strength of the contracting orbicularis oculi muscle and the stability of the tarsus, which depends upon appropriate horizontal tightness and lower eyelid retractor function.
Correction of involutional entropion is aimed at addressing the underlying factors responsible for the eyelid malposition (i.e. horizontal eyelid laxity, retractor disinsertion, over-riding orbicularis oculi muscle). The following procedures are described in more detail and accompanied by videos later in this article. Most frequently, a lateral tarsal strip procedure is utilized to address horizontal eyelid laxity (6). Horizontal eyelid tightening can also be achieved with a pentagonal wedge resection of the lateral lower eyelid (7). The most commonly utilized techniques to address retractor disinsertion and orbicularis oculi overaction are the retractor reinsertion procedure and rotational fornix-based, a.k.a. "Quickert", sutures (8,9). The retractor reinsertion procedure directly reattaches the disinserted lower eyelid retractors, and when a subciliary incision is utilized, the post-operative scarring/traction exerts a downward force which counteracts the over-riding pre-tarsal orbicularis oculi muscle (10). A subciliary approach also spares the conjunctiva, reducing the risk of post-operative scarring and shortening of the posterior lamella. Rotational fornix-based sutures, which are placed deep in the fornix, pass full-thickness through the eyelid, and emerge just inferior to the eyelashes, engaging and advancing the disinserted lower eyelid retractors in addition to rotating the over-riding orbicularis oculi muscle back into its normal anatomic position (10). The retractor reinsertion procedure has been criticized for its increased technical difficulty, time requirement, and potential risk of secondary ectropion and retraction, but it provides a direct view of the pathologic tissues and allows for removal of pre-tarsal orbicularis muscle and redundant skin (10). Multiple other procedures, and combinations thereof, have been described and continued debate regarding the optimal pairing of techniques exists (2). However, it has been shown that a combination of procedures that addresses all three underlying etiologic factors results in lower recurrence rates than techniques that address only one or two of the three (2,10).
For patients with severe symptoms, temporizing measures can be of benefit while awaiting surgical intervention. Botulinum toxin injected into the over-riding orbicularis oculi muscle has been used to provide transient relief (11). In addition, placing a ½ inch wide strip of paper tape such that it engages the lateral skin of the lateral lower eyelid and exerts downward tension can temporarily realign the lower eyelid margin and help mitigate symptoms. A bandage contact lens is also a viable short-term option for symptom mitigation.
Spastic entropion occurs when forceful eyelid closure results in inward rotation of the eyelid margin. The impetus for the forceful eyelid closure is commonly ocular irritation and/or inflammation, which in turn is exacerbated by the entropion, leading to a vicious cycle. Successful treatment of the source of ocular irritation would theoretically eliminate the entropion, but in reality this is infrequently achieved. There is thought that spastic entropion occurs in eyelids that are predisposed to malposition due to increased eyelid laxity. Thus, surgical intervention is typically targeted at stabilization of the lower eyelid through tightening procedures, such as those used in the treatment of involutional entropion. Of note, "Quickert" sutures are of particular utility in the treatment of spastic entropion, especially in poor surgical candidates unable to undergo more extensive procedures, although the recurrence rate of entropion is substantially higher if horizontal eyelid laxity and the over-riding orbicularis oculi muscle are not addressed. Additionally, this particular subset of patients also derives benefit from the use of temporizing measures such as eyelid taping and botulinum toxin injection.
Cicatricial entropion is caused by shortening of the posterior lamella. This is most commonly a result of conjunctival scarring. Once the diagnosis of cicatricial entropion is made, the underlying etiology should be determined. Frequent causes include: trauma, chemical burns, surgery, ocular cicatricial pemphigoid, Stevens-Johnson syndrome, recurrent chalazia or blepharitis, and post-infectious (e.g. trachoma).
In some patients, differentiating between cicatricial and involutional entropion is difficult. A helpful examination technique is to attempt to manually place the lower eyelid in its normal anatomic position. In the case of cicatricial entropion, this will not be able to be performed, whereas in involutional entropion a normal anatomic position will be attainable.
A subtle form of cicatricial entropion, termed "marginal" entropion, is characterized by a rounding of the posterior eyelid margin and anterior migration of the mucocutaneous junction. Marginal entropion is typically a result of long-standing posterior blepharitis.
Treatment of cicatricial entropion is based on lengthening of the posterior lamella, in addition to correcting other underlying factors (e.g. horizontal eyelid laxity). The procedure selected is based on the amount of lengthening required. For mild to moderate cases (including marginal entropion), a tarsotomy procedure with everting sutures (with or without a lateral tarsal strip procedure) works well. For moderate to severe cases, an anterior lamellar recession is often utilized (12-14). This procedure shortens the anterior lamella without altering the posterior lamella, which may be advantageous in cases where the surgeon wishes to avoid stimulating additional conjunctival scarring (e.g. in ocular cicatricial pemphigoid). Of note, by recessing the anterior lamella, some eyelid retraction is caused. For the most severe cases, mucous membrane grafting is performed following lysis of the scarred conjunctiva. Multiple potential donor sites (e.g. buccal mucosa, lower labial mucosa, nasal mucosa, etc.) are available, each with inherent advantages and disadvantages. Other materials such as amniotic membrane, tarsus, hard palate grafts, and synthetic materials such as ENDURAGen® can also be utilized. Similar to the surgical treatment of involutional entropion, combinations of procedures are frequently utilized in the management of cicatricial entropion with treatment aimed at correcting all underlying etiologic factors (15).
-Performed and narrated by Dr. Richard C Allen
If video fails to load, use this link: http://vimeo.com/123354779
*Note: this patient also had a medial spindle procedure performed.
If video fails to load, use this link
If video fails to load, use this link
If video fails to load, use this link: https://vimeo.com/132969590/.
If video fails to load, use this link: https://vimeo.com/123338538
Entropion is a commonly encountered ophthalmologic problem and is categorized as involutional, spastic, or cicatricial. There are multiple surgical options available for the repair of entropion and procedure selection and combination is based on the type and severity of entropion.
ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
|
Clark TJE, Lenci LT, Allen RC, Shriver EM. Involutional entropion: options for surgical management of entropion. EyeRounds.org. posted Sept 14, 2015; Available from: http://www.EyeRounds.org/cases/220-Involutional-entropion.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
