
Chief Complaint: Pus, discharge, and blurry vision in the left eye.
History of Present Illness: A 72-year-old African-American female was referred by an outside ophthalmologist for a corneal perforation in the left eye. She had been followed for several months due to a purulent conjunctivitis of the left eye. She reported blurry vision in the left eye for one month. She denied ever having any pain. Three days prior to the referral, corneal thinning was noted and she was started on gatifloxacin 6 times daily. She perforated despite the antibiotics and was referred for evaluation and treatment.
Past Ocular History: No light perception (NLP) vision in the right eye (OD) secondary to sarcoidosis involving the optic nerve status post biopsy of the right optic nerve 28 years prior
Allergies: No known drug allergies
Family History: Non-contributory
Social History: Non-contributory
Review of Systems: Negative except for what is detailed in the history of present illness
Visual Acuity with correction (Snellen – Linear)
Ocular Motility: Full both eyes (OU)
Intraocular Pressure (IOP): Deferred due to the corneal perforation OS
Pupils:
External: Normal
Slit lamp exam:
Dilated fundus examination (DFE): Dilation was deferred due to corneal perforation on the left eye.
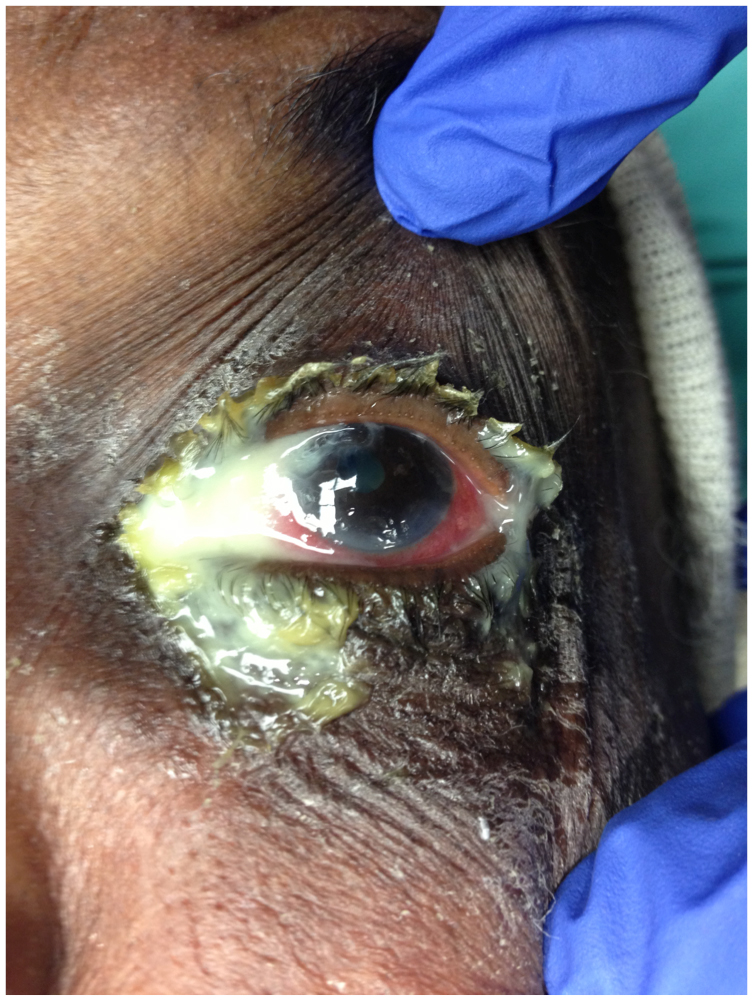
Figure 1. External photograph of the left eye showing copious mucopurulent discharge
Due to the large size of the corneal perforation and active presumed bacterial keratitis and conjunctivitis in a monocular patient, corneal cultures were obtained and an emergent mini-penetrating keratoplasty (PKP) was performed. The patient was concurrently placed on a medication regimen consisting of fortified vancomycin, levofloxacin, prednisolone acetate, atropine, and oral trimethoprim sulfamethoxazole. Oral steroids could not be used to control her sarcoidosis as she had previously developed severe psychosis and systemic infection on prednisone.
On post-operative day (POD) #1, the corneal perforation appeared to be secure after the mini-PKP and was Seidel negative, however a purulent discharge persisted from the nasolacrimal system. At that point, the oculoplastics service was consulted. On exam, the puncta were not inflamed, and there appeared to be no reflux of material or firmness on compression of the canaliculi. Copious discharge was noted with compression of the nasolacrimal sac, so dacryocystitis secondary to nasolacrimal duct obstruction (NLDO) was suspected. A dacryocystorhinostomy (DCR) was scheduled in one week in order to allow time for the cornea to heal and for targeted systemic antibiotics to decrease the bacterial load.
In the week preceding the DCR, a culture obtained from the cornea grew coagulase-negative staphylococcus. Cultures from the punctal discharge grew Provotella, an anaerobe, for which metronidazole was added to her systemic antibiotic regimen.
On POD #6 after the mini-PKP, it was noted that the graft had several loose sutures and was bulging forward. An exam under anesthesia (EUA) was performed at the time of the DCR, and the graft was resutured prior to proceeding with the lacrimal surgery.
During the patient’s DCR, the lacrimal sac was noted to be fibrotic, thickened and surrounded by tissue appearing to be significantly inflamed. Intraoperative frozen sections of the lacrimal sac were sent to pathology and found to be consistent with chronic granulomatous and fibrotic inflammation. Upon further evaluation, the nasal septum was noted to be eroded and necrotic. The surgical plan was reevaluated and discussed with otolaryngology. Rather than forming a traditional ostium for the DCR, a stent was placed just through the nasolacrimal duct in order to dilate the lacrimal system while minimizing manipulation of the nasal mucosa and maintaining more of a barrier between the orbit and necrotic nasal cavity.
Given the monocular status of the patient and the fragility of her corneal graft, ameliorating the purulent dacryocystitis that was the etiology of her corneal perforation was thought to be crucial. The purulence persisted despite the nasolacrimal stenting [Figure 2], so a left dacryocystectomy with cauterization of the puncta and canaliculi were performed. The patient did well post-operatively with resolution of the discharge [Figure 3], no significant epiphora, and with stabilization of the graft [Figure 4] and visual acuity improving to 20/50 8 months post-operatively.
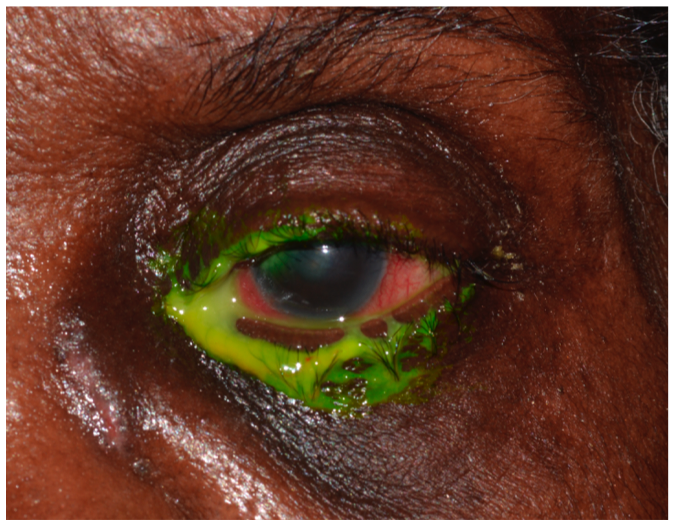
Figure 2: Pre-dacryocystectomy
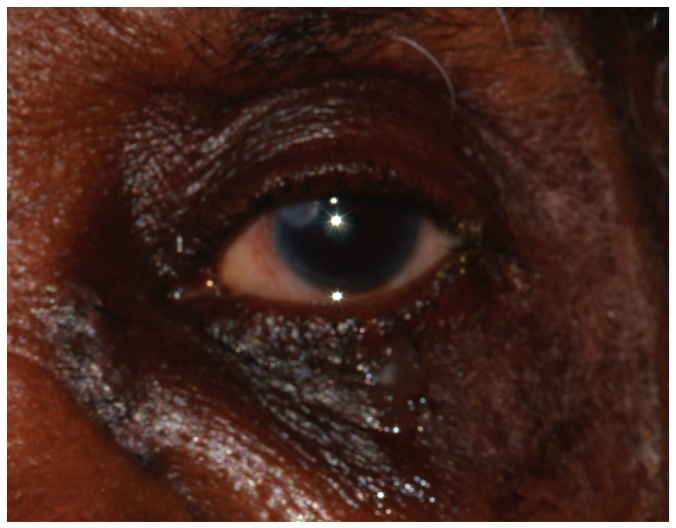
Figure 3: Post-dacryocystectomy
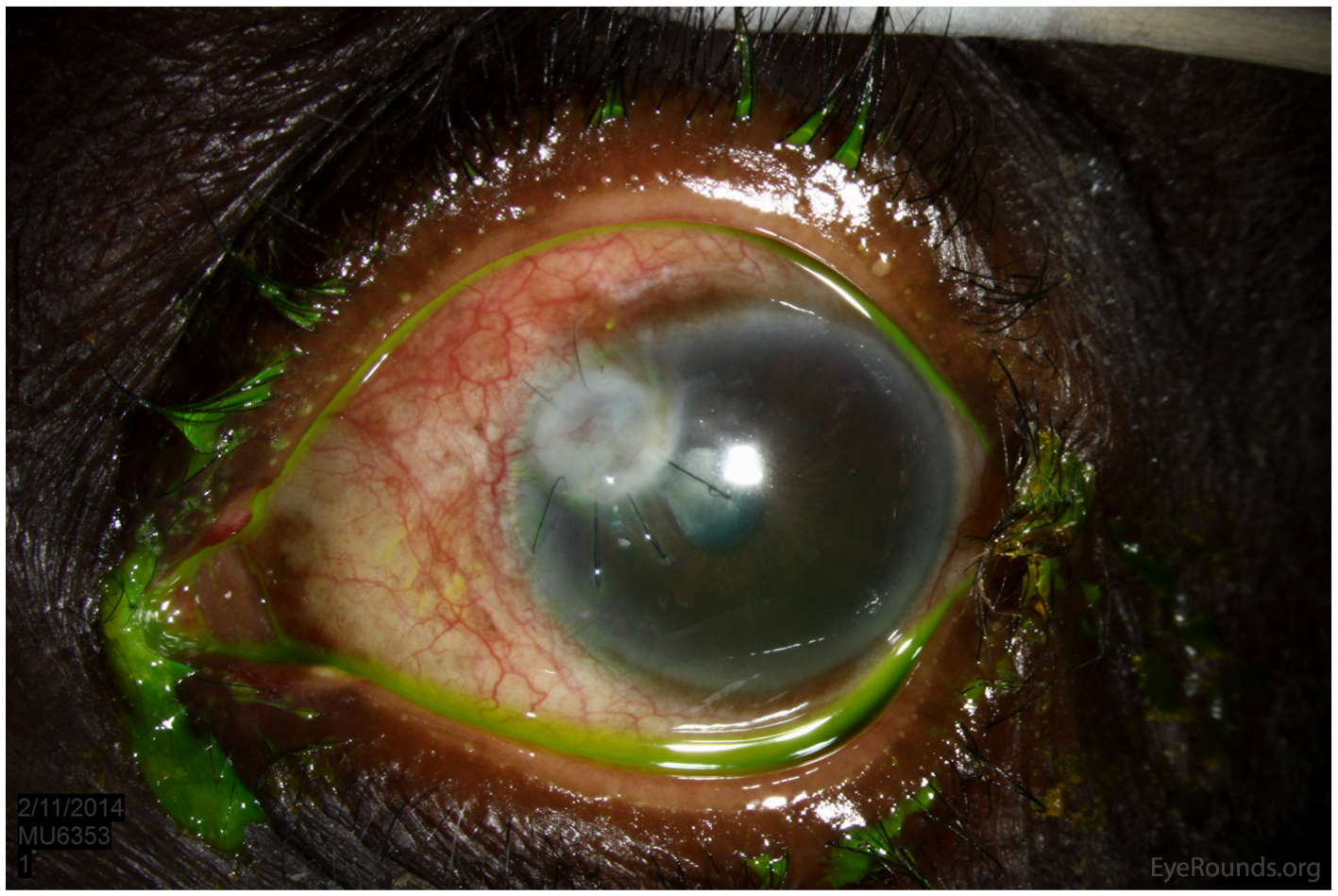
Figure 4: Mini penetrating keratoplasty
Corneal perforation and chronic dacryocystitis secondary to NLDO from sarcoidosis
Sarcoidosis is a multi-system inflammatory disease of unknown etiology characterized by non-caseating granulomas throughout the body. Orbital and adnexal manifestations of sarcoidosis include granulomatous inflammation causing microarchitectural distortion of the lacrimal gland (63%), eyelids (17%), orbit (13%) and the lacrimal sac (7%) (1). In fact, some studies report sarcoidosis involving the lacrimal sac is an infrequently reported problem, accounting for as little as 1-2% (2). For more information on sarcoidosis, please refer to the EyeRounds case Sarcoidosis affecting the lacrimal gland.
Chronic inflammatory and granulomatous infiltration of the nasolacrimal duct mucosa can result in an acquired nasolacrimal duct obstruction (NLDO). NLDO can be classified into two groups: primary acquired nasolacrimal drainage obstruction (PANDO) and secondary acquired lacrimal drainage obstruction (SALDO).
Infectious
Inflammatory
Neoplasia
- Primary neoplasm (5):
- Primary epithelial tumors: papilloma, squamous cell carcinoma, and transitional cell carcinoma
- Primary non-epithelial tumors: fibrous histocytoma, malignant lymphoma, and malignant melanoma
- Secondary neoplasm: squamous cell carcinoma, basal cell carcinoma, adenoid cystic carcinoma, leukemia and lymphoma of adjacent tissues may extend and cause obstruction of the nasolacrimal system
- Metastasis: most commonly breast carcinoma; prostate carcinoma and malignant melanoma rarely metastasize to the lacrimal system
Trauma
- Iatrogenic traumas: secondary to probing, punctal plugs, and sinus surgery
- Accidental traumas: canalicular tears and lacerations, and naso-orbito-ethmoid bone fractures causing nasolacrimal entrapment and damage
Mechanical
- Mechanical NLDO are physical obstructions due to endogenous factors like dacryoliths and migrated punctal plugs or exogenous factors like caruncular masses and sinus mucoceles
Patients commonly present with epiphora (tearing), mucopurulent discharge, irritation, and blurry vision due to tear accumulation in the conjunctival cul-de-sac. NLDO can be associated with acute or chronic dacryocystitis, lacrimal mucocele, lacrimal abscess, orbital cellulitis, and orbital cellulitis leading to cavernous sinus thrombosis. Further evaluation may show tear meniscus height greater than 2 mm, punctal stenosis, canaliculitis, or reflux discharge from the punctum (3).
These tests help to determine the location of the obstruction.
The lacrimal apparatus consists of a secretory and drainage system that functions to provide lubrication of the cornea and conjunctiva. The tears secreted by the lacrimal gland spread over the corneal surface with the blinking motion. The tears may disappear due to evaporation or gather in the lacrimal lake near the medial canthus to be drained by the punctum. An obstruction of the drainage system causes tear stasis and an increased number of pathogens within the tears themselves. With an increased number of pathogens circulating in the tears, corneal ulcers are more likely to occur.
Small, retrospective case series have shown both external and endonasal dacryocystorhinostomy to be beneficial in NLDO secondary to sarcoidosis.
A retrospective case series (2) was performed to investigate the surgical outcomes of external dacryocystorhinostomy (EX-DCR) performed in patients with sarcoidosis. The study included 13 sides of 9 sarcoidosis patients. A subset of patients was also given intralesional triamcinolone. Initial EX-DCR was successful in 10 of 13 (87%) surgeries with an average follow up of 31 months. All the patients receiving intralesional triamcinolone had resolution of epiphora (5 surgeries, 4 patients). This success rate is compared to only 3 of 8 (38%) surgeries in the group without intralesional triamcinolone. The study concluded that EX-DCR surgery can successfully treat NLDO associated with sarcoidosis and that the use of intralesional triamcinolone may provide an added beneficial.
Endoscopic powered-type Endonasal DCR (EN-DCR) and non-endoscopic mechanical EN-DCR, alternative treatments to EX-DCR, has been shown to also be useful in NLDO secondary to sarcoidosis. The surgical outcomes of EN-DCR performed in 18 sides of 12 sarcoidosis patients were investigated retrospectively (7). The success rate was 100% after an average of 11.3 months follow up. While the results of the study are impressive, the low number of cases, short follow up, and variability in steroid and treatment regimen limited the study.
Additional studies comparing EX-DCR and EN-DCR, as well as the role of steroids are warranted.
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
Scott J., Beebe JM, Shriver EM. Detachment (PVD). EyeRounds.org. posted Oct 21, 2015; Available from: https://eyerounds.org/cases/222-NLDO.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
