
Facial droop and slurred speech
A 68-year-old man presented to the eye clinic with five days of right-sided facial droop, which was associated with the inability to fully close the right eye and slurred speech. Approximately two to three days before the onset of the facial droop, he noted a sharp, severe, retroauricular pain with intermittent radiation into the right side of his face. He also noted altered and diminished taste on the right side of his tongue. He denied any other proceeding symptoms. He was evaluated at an outside hospital, where a head computed tomography (CT) was negative. He was then transferred to the University of Iowa Hospitals and Clinics (UIHC) with concern for acute cerebrovascular accident. Upon evaluation in the UIHC Emergency Department, an isolated facial nerve palsy was identified. He was diagnosed with Bell's palsy and started on oral prednisone (60 mg daily), lubricating eye drops, and ophthalmic ointment with a plan for outpatient follow-up with Ophthalmology and Otolaryngology.
Upon evaluation in the Oculoplastics clinic, he reported using tape to keep his right eye closed. He denied eye pain or diplopia but stated that the vision in his right eye was slightly blurred.

Figure 1. External photo demonstrates right-sided facial droop, brow ptosis, and lower eyelid ectropion.
Upon evaluation in the Oculoplastics clinic, a video demonstrating the complete nature of the patient's facial nerve dysfunction was sent to the Otolaryngology resident on-call. The Otolaryngology team asked to see the patient immediately and electroneuronography (ENoG) and electromyography (EMG) were ordered to evaluate candidacy for surgical decompression of the facial nerve. ENoG revealed 100% loss of facial nerve function and EMG showed absent motor unit potential of the orbicularis oris and orbicularis oculi despite maximal effort. Right facial nerve decompression via a middle cranial fossa (MCF) approach was performed 12 days after the onset of symptoms. Following decompression, the facial nerve was found to be anatomically intact but it did not respond to electrical stimulation.
The patient continued to experience a significant degree of lagophthalmos and had to continue eyelid taping. He remained incapable of producing a complete blink or fully closing his right eye. Lower eyelid ectropion secondary to laxity was also present. Despite significant lagophthalmos, only minimal exposure keratopathy was present. At this point, the patient chose to defer placement of an eyelid weight so an external, stick-on weight was ordered instead.

Figure 2. External photo at 3 month post-operative visit showing right brow ptosis and lower eyelid ectropion.

Figure 3. Lateral view of right eyelid with BlinkEze® eyelid weight in place.
When evaluated six months post-operatively, the patient had discontinued use of the weight as he felt his eyelid function had improved significantly. He also noted that he had begun to experience epiphora. On physical exam, lagophthalmos and ectropion were present but improved compared to his one month post-operative visit. No exposure keratopathy was present. The continued use of preservative-free artificial tears and lubricating eye gel at night was recommended.

Figure 4. External photo at 6 month post-operative visit showing improved right brow ptosis and lower eyelid ectropion.
When asked, the patient was able to fully close the right eye, but he continued to have an incomplete reflexive blink. Lower eyelid laxity, ectropion, and epiphora were still present. No exposure keratopathy was noted.

Figure 5. External photo at 10 month post-operative visit showing mild residual right brow ptosis and lower eyelid ectropion.
The patient continued to experience epiphora. He demonstrated a full reflexive blink with good orbicularis oculi tone. There was only mild eyelid laxity remaining, with a high tear lake and no ectropion. No keratopathy was noted.

Figure 6. External photo at 18 month post-operative visit showing resolution of right brow ptosis and lower eyelid ectropion, as well as an increased tear lake height
Bell's palsy, status post (s/p) facial nerve decompression. Complete facial nerve paralysis was present upon presentation that improved to House-Brackmann Grade II paralysis one year post-operatively.
For detailed information regarding the etiology and clinical features of Bell's palsy, please refer to the EyeRounds article Facial Nerve Palsy: Ocular Complications and Management [1].
Care should be taken to differentiate Bell's palsy from Ramsey Hunt syndrome, which is characterized by otalgia and the presence of a vesicular rash on the postauricular skin, ear canal, or tympanic membrane [2]. Ramsey Hunt syndrome may also involve other cranial nerves, particularly the auditory and vestibular nerves leading to acute, unilateral, sensorineural hearing loss or vertigo, respectively. The natural history of Ramsey Hunt syndrome is different from that of Bell's palsy and requires different management.
Patients with a history and physical exam highly suggestive of Bell's palsy may not always require magnetic resonance imaging (MRI) or computed tomography (CT). However, patients with otorrhea, vestibular complaints, or hearing loss should be evaluated with both MRI and high-resolution CT [2]. An atypical presentation, such as a slow onset of symptoms, recurrent episodes of acute paralysis, evidence of synkinesis, or a proceeding facial twitch should also prompt imaging studies, as these symptoms may suggest an alternative diagnosis (e.g. tumor) [3]. Planned surgical decompression or persistent, severe paralysis after 6 months are also indications for imaging [2].
Further steps should be taken during the initial evaluation depending upon individual patient characteristics. For patients living in areas endemic for Lyme disease, serologic testing (IgM, IgG) should be obtained [2]. Patients with vestibular complaints require evaluation with an electronystagmogram (ENG), and those with complete facial nerve paralysis require electrophysiologic testing (EMG, ENoG) in order to assess candidacy for facial nerve decompression. Further details regarding these tests are beyond the scope of this discussion.
The mainstay of acute treatment for Bell's palsy is early treatment with oral glucocorticoids for all patients [4-7]. Several double-blind, placebo-controlled, randomized trials support the effectiveness of early, short-term, oral glucocorticoid therapy for all patients within 3-7 days of symptom onset, demonstrating a quicker and more complete recovery of facial nerve function [8-13]. Patients in these trials were treated with 10-day courses of oral prednisone 50-80 mg daily, with or without a taper after day five of treatment. There is no evidence to support one particular steroid-dosing regimen over another. At our institution, patients who present within 7 days of symptom onset are treated with a 10-14-day course of 60-80 mg/day of oral prednisone.
Bell's palsy was first described as a facial nerve palsy without a known etiology [14]. However, recent studies indicate that herpes simplex virus (HSV) may play a role in the pathogenesis of Bell's palsy. Evidence of HSV type 1 (HSV-1) infection has been found in patients with Bell's palsy, [15-18] and HSV-1 inoculation has been shown to cause facial paralysis in mice [19 ,20]. Consequently, antiviral therapy has been proposed as one potential treatment for Bell's palsy.
Antiviral therapy may be used alone or in addition to glucocorticoid therapy. Data supporting the use of antiviral therapy are mixed. Two large clinical trials have been performed that randomized 496 and 829 patients, respectively, to receive placebo, steroids alone, antivirals alone (acyclovir or valacyclovir), or steroids and antivirals [11 ,12]. Both studies showed no significant difference in the recovery of facial nerve function between groups that received placebo or antivirals alone. Similarly, no difference was found between groups that received steroids alone or steroids and antivirals. However, both of these studies included patients with all degrees of facial weakness. It is known that patients with mild facial paresis have a high rate of recovery without treatment. Thus, any benefit of antiviral therapy for patients with more severe paresis or paralysis may have been masked by the subset of patients with mild degrees of weakness expected to demonstrate recovery even without treatment.
Several smaller trials have demonstrated a trend towards benefit with antiviral therapy [8 ,13], and one trial showed a benefit to receiving both antiviral (valacyclovir) and steroid therapy compared to steroids alone [9]. Furthermore, a 2015 Cochrane review that pooled results from 10 trials, including all of the studies mentioned above, found antiviral and steroid therapy to be superior to steroid therapy alone [21]. Importantly, no serious adverse effects have been documented in any study using antivirals for Bell's palsy to date. Patients who present to our institution within 7 days of symptom onset are treated with valacyclovir 500 mg orally 3 times per day for 10 days in addition to steroid therapy.
Physical therapy is another potential treatment for facial paresis that includes exercises, massage, electrical stimulation, acupuncture, and biofeedback. A recent Cochrane review found only twelve low to moderate quality studies that evaluated the efficacy of physical therapy for facial paresis due to Bell's palsy [22]. One of these studies showed that facial exercises reduce the rate of synkinesis (involuntary facial movement that occurs with voluntary movement of a different facial muscle group) at three months [23]. Another trial showed some benefit for facial exercises for patients that have had persistent nerve palsy for nine months or longer [24]. While physical therapy may provide some benefit for patients, the evidence supporting its use remains relatively weak, and it should only be considered as an adjuvant therapy. At our institution, practice patterns vary in term of the use of physical therapy. Electrical physical therapy is not used, as it may cause an increased rate of complications [22].
The facial nerve enters the temporal bone through the internal acoustic meatus and travels through Fallopian canal of the temporal bone before exiting the skull via the stylomastoid foramen (Figure 7). The Fallopian canal contains labyrinthine, tympanic, and mastoidal segments. It is believed that Bell's palsy is related to neural edema and compression within the labyrinthine segment of the Fallopian canal. Thus, decompression of the labyrinthine and perigeniculate segments of the facial nerve has been proposed as one potential treatment for Bell's palsy (Figure 8).
![Route of the facial nerve as it enters the temporal bone through the internal acoustic meatus, travels through the Fallopian canal, and exits via the stylomastoid foramen. The Fallopian canal can be further divided into labyrinthine, tympanic, and mastoidal segments (not shown here). Image by Patrick J. Lynch, medical illustrator [CC BY 2.5 (http://creativecommons.org/licenses/by/2.5)], via Wikimedia Commons](../cases-i/case256/f7L-Cranial_nerve_VII.gif)
Figure 7. Route of the facial nerve as it enters the temporal bone through the internal acoustic meatus, travels through the Fallopian canal, and exits via the stylomastoid foramen. The Fallopian canal can be further divided into labyrinthine, tympanic, and mastoidal segments (not shown here). Image by Patrick J. Lynch, medical illustrator [CC BY 2.5 (creativecommons.org/licenses/by/2.5)], via Wikimedia Commons
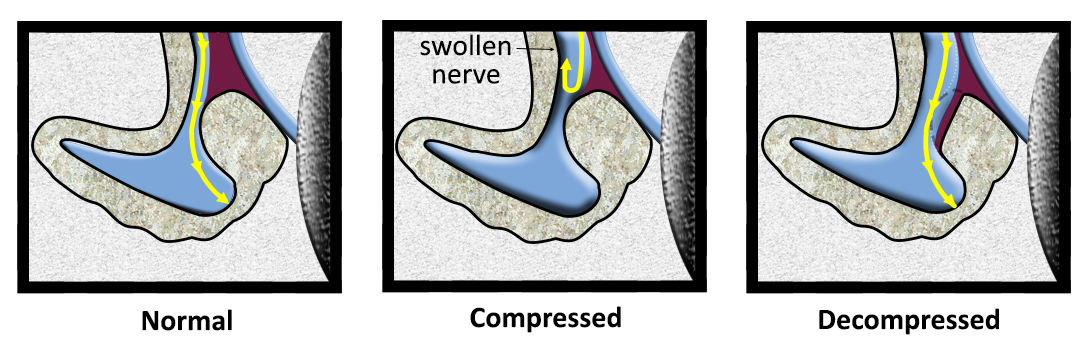
Figure 8. Schematic showing facial nerve decompression. Panel A shows a normal facial nerve within the Fallopian canal of the temporal bone. Panel B shows the facial nerve compressed within the labyrinthine segment of the Fallopian canal. Panel C shows the facial nerve after decompression of the labyrinthine segment of the Fallopian canal.
Controversy currently exists as to the role of surgical decompression due to good outcomes with observation alone in patients with incomplete paralysis, the lack of large trials, and the complications associated with surgical intervention [5]. Consequently, surgical therapy is not currently recommended for the majority of patients with Bell's palsy [5 ,25 ,26].
Surgical intervention is reserved for patients who have a poor prognosis with observation or medical therapy alone. One study found that patients with complete loss of facial nerve function, 90% or greater loss on ENoG testing, and absent volitional nerve activity on EMG have a 58% chance of a poor outcome (House-Brackmann III or IV [27]) at 7 months [28]. Several other studies have also supported the prognostic value of ENoG testing and the association of 90% or greater functional loss on ENoG testing with poor outcomes with medical management alone [29 ,30]. Surgical intervention may be beneficial for these patients in improving the likelihood of recovery of good facial nerve function.
Facial nerve decompression has been described via either a transmastoid or middle cranial fossa (MCF) approach. The MCF approach has demonstrated the greatest promise, [28] as it provides access for decompression of the labyrinthine segment of the facial nerve. Transmastoid approaches do not provide access to this region of the Fallopian canal and are not currently used for the treatment of Bell's palsy. One multi-center, case-control study demonstrated near complete recovery of facial nerve function (House-Brackmann I-II) for 31 of 34 (91%) patients treated with facial nerve decompression via an MCF approach as compared to 15 of 36 (42%) patients treated with steroids alone [28]. All patients who underwent surgery had >90% reduction in amplitude on ENoG, absent voluntary facial nerve activity, and were able to undergo surgery within 3-14 days of symptom onset. The efficacy of a MCF approach has also been validated by an additional report [31].
Awareness of the window of opportunity for facial nerve decompression is critical. Providers in primary care clinics, emergency departments, and eye clinics must recognize that patients with complete or near-complete facial nerve paralysis need urgent referral so that appropriate diagnostic testing (ENoG and EMG) may be attained and surgical intervention completed within 14 days of symptom onset [28].
All patients with complete facial nerve paralysis should be referred to a center with expertise in MCF surgery [2]. Identifying and maintaining appropriate referral pathways is important as the number of neuro-otologists who regularly perform procedures via the MCF approach remains limited [32]. Additionally, the MCF approach is a technically demanding procedure that can be associated with severe complications (e.g. cerebrospinal fluid leak, hearing loss, facial nerve injury) [33-35]. These factors should be considered and discussed when choosing to proceed with facial nerve decompression.
Epidemiology [36-28]
|
Signs and Symptoms of Bell's Palsy
|
Work-up for Facial Nerve ParalysisImaging (CT or MRI)
Electrophysiologic testing (ENG, EMG, or ENoG)
Serologic Lyme disease testing
|
Treatment Recommendations
|
Andresen NS, Clark TJE, Sun DQ, Hansen MR, Shriver EM. Bell's Palsy Treated With Facial Nerve Decompression, EyeRounds.org. posted August 1, 2017; Available from: https://eyerounds.org/cases/256-Bells-Palsy.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
