
INITIAL PRESENTATION
Chief Complaint: Worsening double vision
History of Present Illness:
A 62-year-old male presented to the eye clinic with worsening diplopia for the last 10 years, but more drastically in the last 2-3 years. The diplopia was oblique and binocular, present at distance and near. He reported a history of bilateral retinal detachments requiring pars plana vitrectomy (PPV) and lensectomy, and a history of scleral buckle placement on the right eye. Following these surgeries, he remained aphakic bilaterally and was managed with soft contact lenses.
Past Ocular History:
Past Medical History:
Medications:
Family History:
Social History:
OCULAR EXAMINATION
Visual acuity: by Snellen Chart (at distance with correction)
Pupils
Stereoacuity testing
Cycloplegic refraction (over soft contacts)
Contacts
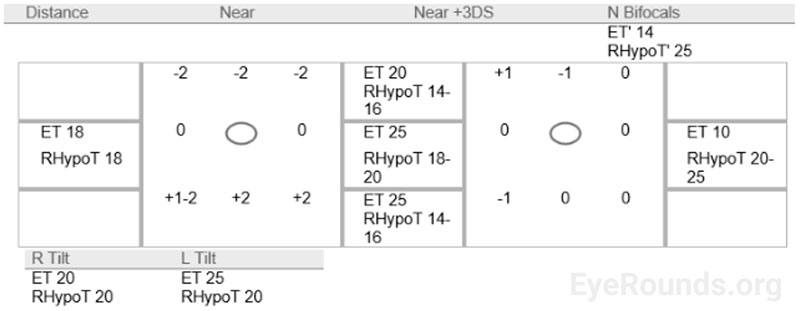
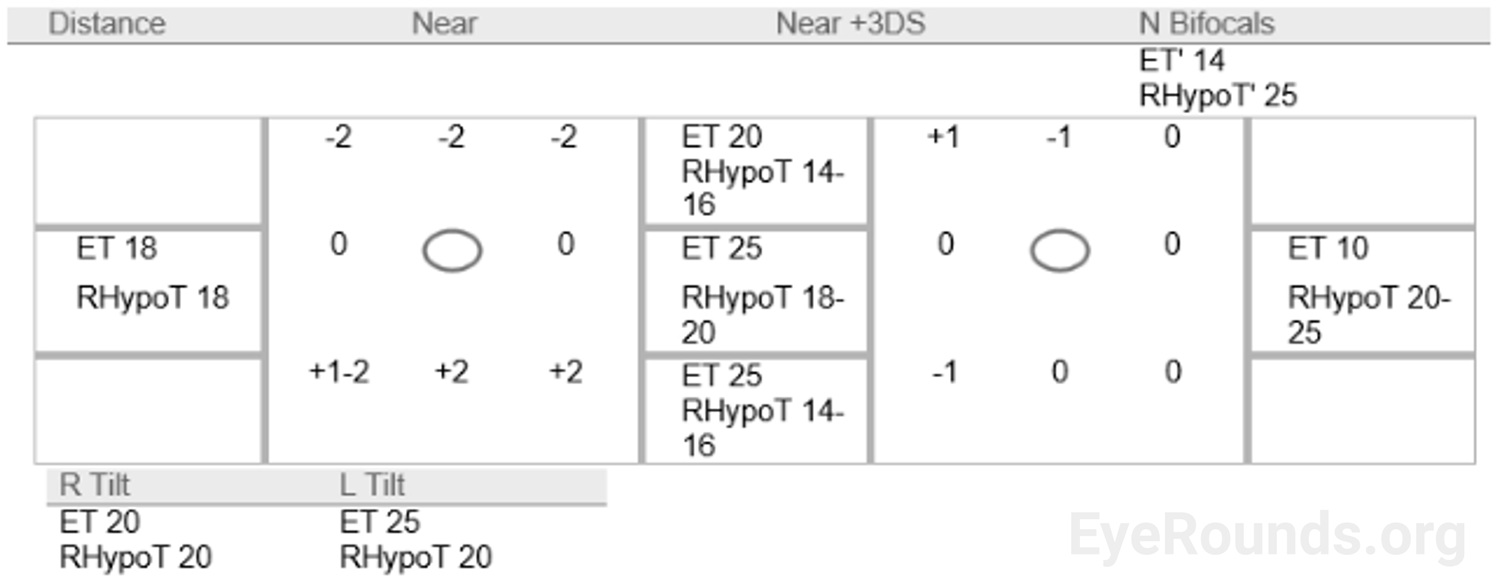
Strabismus Exam
Slit Lamp Exam
Posterior Segment Exam
DIAGNOSIS
Moderate angle alternating esotropia (intermittent suppression with low fusional amplitudes), large angle right hypotropia
CLINICAL COURSE
Given the patient's worsening diplopia, difficulty fusing, and limited improvement with prisms, he decided to proceed with strabismus surgery. He was also interested in secondary intraocular lens (IOL) placement, which was performed prior to strabismus surgery. Given his prior aphakia with lack of capsular support, anterior chamber IOLs were chosen. Following placement of anterior chamber IOLs OU, his uncorrected visual acuity was 20/25+2 OD and 20/25+1 OS.
Surgical planning for correction of his strabismus was complex with both moderate angle esotropia and large angle hypotropia in the setting of prior scleral buckle in the right eye, especially as the patient preferred fixation with his left eye. Given the large deviations on clinical exam, the surgical goal was to obtain enough correction to allow the patient to benefit from use of prism. Although several surgical approaches were considered, given the large deviations in multiple directions on exam, bilateral medial rectus recession (BMRc), a right inferior rectus recession (RIRc), and a left superior rectus recession (LSRc) were planned.
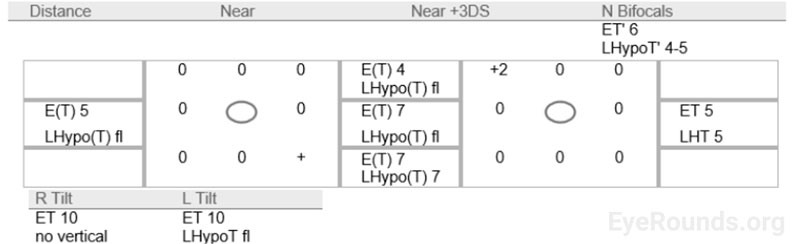
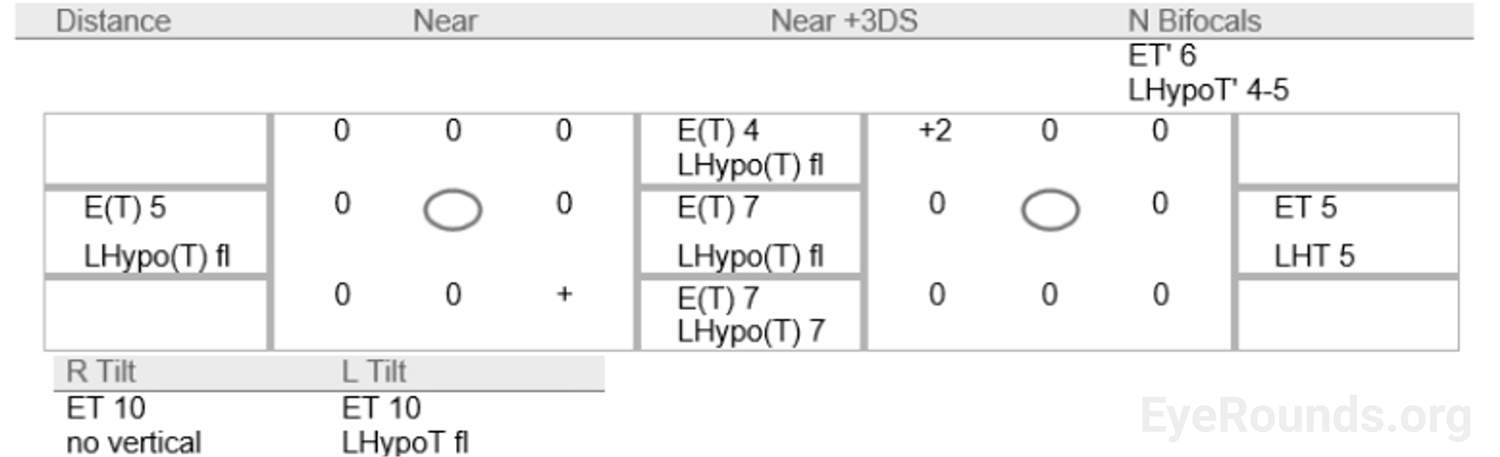
The patient underwent BMRc (4.0 mm OD, 7.5 mm OS) with adjustable suture (including adjustment two hours after the surgery, further recessing the left medial rectus from 4.0 mm to 7.5 mm), RIRc (8.5 mm) with adjustable suture (including adjustment from 3.5 mm to 8.5 mm in the same time frame) and LSRc (3.5 mm). The operation was notable for moderate scarring around the scleral buckle. The recovery period was unremarkable. At 7-week follow up, the patient reported good alignment with no diplopia at distance and only mild diplopia in downgaze at near. He was offered prism for his prescription but declined due to satisfactory subjective vision without.
Strabismus Exam
Etiology/Epidemiology
Strabismus in the setting of prior scleral buckle surgery represents a major source of post-operative morbidity. Transient strabismus following scleral buckling can occur in up to 50% of cases, and 5-25% of patients develop permanent strabismus following scleral buckle placement.[1,2] The etiology of such strabismus is often multifactorial, but includes restrictive adhesions, direct extraocular muscle injury, mechanical changes in extraocular muscle vector force, decompensation of childhood strabismus, and "sensory deviations" due to poor vision.[3,4] Due to the variable configurations of scleral buckles to treat retinal pathology, the specific characteristics of strabismus in these patients are also variable. Understanding the time course of symptoms and its relationship to possible mechanisms of disease is crucial for treatment and operative planning. For instance, adhesions typically take months to years to form, but changes in extraocular muscle geometry can be appreciated immediately following buckling.
Epidemiologic data on the patterns of strabismus in post-retinal detachment surgery is sparse, but all types of strabismus have been described including esotropia, exotropia, hypotropia, hypertropia, and cyclodeviations. Some authors suggest that vertical and torsional etiologies are more common than horizontal deviations, and certain patterns can have specific anatomical correlates.[2] For example, incomitant horizontal deviations often result from violation of the medial fat pad leading to restriction of the medial rectus muscle, and hypotropia commonly occurs from violation of the inferior fat pad or presence of mass of the scleral buckle beneath the inferior rectus.[2] Therefore, preventive measures during retinal surgery are important, and include avoiding violating the sub-Tenon's fat pad, avoiding cryotherapy in muscles, and ensuring buckles do not include any oblique muscles. Despite these measures, the risk of strabismus cannot be avoided entirely.
Preoperative workup
In the work-up of patients with diplopia following retinal detachment, standard strabismus exam techniques should be used. Evaluating the potential for fusion, and quantifying primary and secondary deviations is crucial to elucidate possible mechanisms. Additionally, dragged-fovea diplopia syndrome must be considered, as it causes a diplopia not correctable by strabismus surgery.[5] In this condition, the fovea has reattached heterotopically, leading to a mismatch of central and peripheral fusion.
Surgical considerations
Compared to typical strabismus surgery, strabismus surgery with a scleral buckle in situ has multiple challenges. First, in addition to adhesions caused by prior surgery, the mechanical obstruction from a scleral buckle underneath rectus muscles can make surgical exposure difficult. Second, the mechanical changes of muscle vectors due to an underlying buckle can complicate operative planning and prognostication. For these reasons, many studies have investigated the benefits of scleral buckle removal for patients undergoing this procedure.[6] However, with the advent of improved surgical techniques, the need for buckle removal has been reduced, and recent studies have found no difference between buckle explant vs. retaining the buckle in strabismus surgery.[7] In addition, removal of the buckle poses an ~8% risk of retinal re-detachment, which underscores the benefit of leaving the buckle in place.[8]
A notable alternative to strabismus surgery in such patients is botulinum toxin injection. Multiple case series have described an improvement in symptoms following botulinum toxin injections for post-buckling strabismus patients, with success rates between 15-85%.[9,10] However, this treatment appears less effective for restrictive/mechanical strabismus, which comprises a large portion of post-buckling strabismus patients. Additionally, a recent Cochrane review could not determine the effectiveness of this treatment in the general strabismus patient population due to small sample sizes in the available studies, which is true in the post-buckle subpopulation as well.[11] Given this uncertain evidence, along with the difficulty of injecting particular muscles in the clinic, botulinum toxin treatment should only be used in limited situations.
Surgical Technique
In patients requiring operative treatment of strabismus, there are clear advantages for retaining the scleral buckle whenever possible. However, given the mechanical changes discussed above, a modified surgical technique in the setting of a scleral buckle is required. Namely, given the difficulty in predicting post-operative motility due to changes in extraocular muscle geometry, as well as the unpredictable effect of scar tissue lysis and re-formation, adjustable suture techniques are needed for a good surgical outcome. In the above case, the patient's longer axial eye length (as evidenced by relatively low hyperopia even when aphakic) necessitated larger surgical doses than expected.
When surgically approaching the muscles after a scleral buckle has been placed, the surgeon should expect a significant amount of scarring of the conjunctiva and the muscle itself. It is often the case that a rectus muscle may have developed a new insertion point just posterior to the buckle, with atrophy of the area overlying the buckle. For this reason, it is often necessary to hook the muscle more posteriorly than one would expect. Dissection of scar tissue must be performed carefully, and preferably by a surgeon with experience in re-operated and scarred muscles. When re-attaching the muscle, scleral passes may be placed anterior to the buckle and the muscle hung back posterior to or overlying the buckle. If needed, needle passes may be placed on the buckle itself. In the situation of an oblique muscle being caught in or scarred to the buckle, careful dissection may be possible.
Recent studies of patients receiving strabismus surgery without buckle explantation have found 94% of patients demonstrate an improvement in diplopia, and 74% have a good final motor outcome.[12] However, given this procedure often requires lysis of adhesions due to scar tissue or muscle fibrosis, further scar tissue may develop complicating recovery.[13] A separate study found that first surgery success was best predicted by a horizontal deviation less than 10 diopters and minimal restriction with forced ductions.[14] Patients with more severe pathology should be counselled on the possible need for additional surgery to obtain an adequate outcome. Complications are similar to standard strabismus surgery, including unsatisfactory eye alignment, induced astigmatism, and granuloma or conjunctival inclusion cyst development.[15] Anterior segment ischemia can be a particular concern, as the risk increases with surgery on multiple muscles in the same eye as is often the case in these patients, as well as when vertical rectus muscles are operated on.[16,17] However, as above, outcomes are typically quite good for these patients, and they benefit greatly from improvements in their diplopia.
Strabismus Surgery in Setting of Scleral Buckle from University of Iowa Ophthalmology on Vimeo.
SUMMARY
Scleral Buckle-associated Strabismus
EPIDEMIOLOGY
|
SIGNS
|
Symptoms
|
Management
|
Gundlach B, Strampe M, Stiff H, Kemp P. Strabismus Surgery in Setting of Scleral Buckle. EyeRounds.org. June 21, 2022. Available from https://EyeRounds.org/cases/325-strabismus-surgery-scleral-buckle.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links

{kind=link}
{kind=link}