INITIAL PRESENTATION
Chief Complaint: Blurry vision of the right eye
History of Present Illness
A 55-year-old immunocompetent man was referred for 11-months of progressive blurry vision, burning, and photophobia in the setting of corneal edema and epithelial erosions in his right eye. These findings had persisted with unclear etiology despite a trial of prednisolone, Muro 128 drops, and oral valacyclovir. Two weeks prior to presentation, his exam was notable for mild conjunctival injection, patchy epithelial basement membrane dystrophy, and central corneal edema in the right eye. The left eye was unaffected.
Past Ocular History
Past Medical History
Medications
Allergies
Family History
Social History
Review of Systems
OCULAR EXAMINATION
| OD | OS | |
|---|---|---|
| Lids/lashes | Very long lashes with corneal touch without staining at baseline | Very long lashes with corneal touch without staining at baseline; one distichiatic lash without cornea touch |
| Conjunctiva/sclera | Clear | Clear |
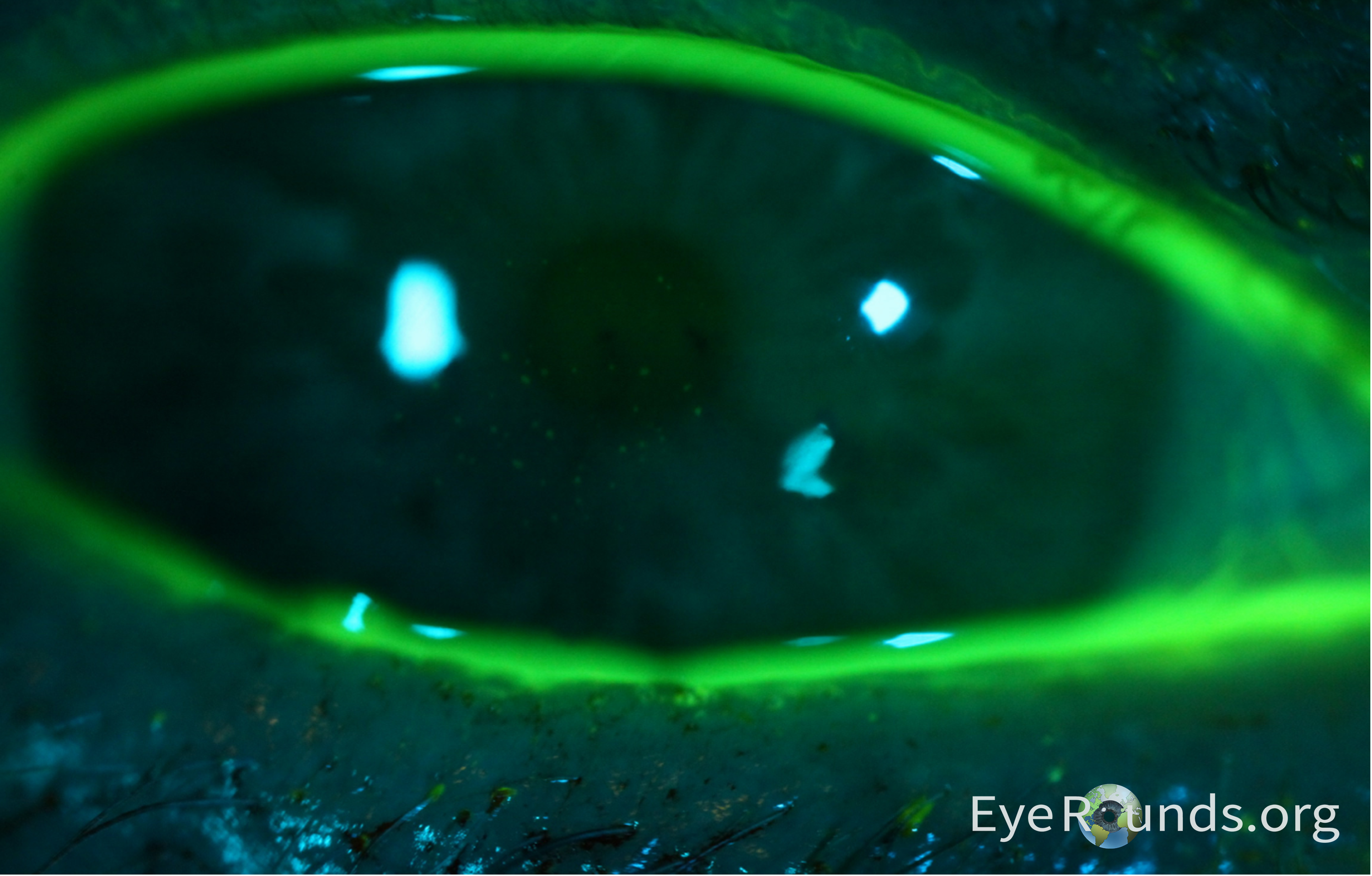
| Cornea | Bandage contact lens in place; epithelial multifocal punctate raised coarse lesions staining with fluorescein centrally; on sclerotic scatter, patch of edema centrally; no keratic precipitates | clear |
| Anterior Chamber | Deep and quiet | Deep and quiet |
| Iris | Normal architecture, no atrophy or transillumination defects | Normal architecture |
| Lens | Clear | Clear |
| Anterior Vitreous | No cell or flare | No cell or flare |
| OD | OS | |
|---|---|---|
| Disc | Normal | Normal |
| Macula | Normal | Normal |
| Vessels | Normal | Normal |
| Periphery | Normal | Normal |
DIFFERENTIAL DIAGNOSIS:
CLINICAL COURSE
This patient was initially evaluated in the cornea clinic as a referral from outside hospital with approximately 1 year of irritation and edema OD refractory to a completed trial of topical steroid treatment. Ocular exam was notable for diffuse conjunctival injection, corneal edema, borderline elevated intraocular pressure OD (22 mmHg), and patchy EBMD OD. Imaging obtained at initial evaluation, including OCT anterior segment imaging and corneal topography, confirmed stromal edema with EBMD and mild posterior flattening of the cornea. The patient had bandage contact lens placed OD and was prescribed moxifloxacin, artificial tear solution, and allergy drops QID, in addition to brimonidine. Prednisolone was held.
Approximately 2 weeks later, the patient returned to clinic for a corneal scraping OD. Repeat ocular examination was significant for decreased intraocular pressure OD of 13 mmHg compared to initial visit, in addition to the presence of staining central epithelial punctate lesions OD. Corneal scraping specimens were analyzed via potassium hydroxide preparation and aerobic culture, with no fungal elements observed and no organisms or PMNs, respectively. Differential diagnosis was updated to reflect high suspicion for microsporidia keratitis given the year-long chronic irritation refractory to initial treatment in an immunocompetent patient, stromal edema, and pattern of central punctate epithelial lesions. The possibility of adenoviral keratitis was also considered. Brimonidine was stopped and the patient was restarted on prednisolone acetate taper, in addition to continuing moxifloxacin and artificial tears. The patient was also prescribed albendazole 400 mg PO BID, but the patient was not able to take this medication due to lack of insurance coverage. PCR was considered as a potential next step for formal diagnosis of microsporidia keratitis. Patient clinically improved on medication regimen over the next month with less tearing and irritation. Approximately six months after initial evaluation, the patient’s foreign body sensation with accompanying irritation had resolved with no superficial keratitis or edema visualized on exam.
DISCUSSION
Microsporidia species, recently classified as fungi, are a rare cause of infectious keratitis.(1) Despite this reclassification, microsporidia keratitis is a separate entity from fungal keratitis. Microsporidia are unicellular obligate parasites that have been implicated in various organ system infections with a predilection for the gastrointestinal system. The involvement of the eye was initially described in the early 1970s after exposure to goats, with spores observed in the deep stroma of the cornea on histopathology. Ocular infections did not gain widespread recognition among ophthalmologists until the 1990s, coinciding with infections observed in individuals with human immunodeficiency virus (HIV). However, an escalating incidence of microsporidiosis has been observed in immunocompetent patients since the beginning of the century.(2) While the global prevalence of microsporidia keratitis is not well described, a study of 4822 microbial keratitis cases in India found that 0.4% were confirmed to be due to microsporidia.(3) Some risk factors associated with the development of microsporidia keratitis include systemic immunosuppression, local immunosuppression, trauma, soil exposure, and contact lens usage.(4) Numerous outbreaks in various Asian countries have been linked to contaminated soil and water exposure with increased prevalence of infections during periods of heavy rain and floods.(4-8) A study in the United States corroborates these findings with over 50% of infected patients having a history of exposure to specific lakes or swamps.(9) These studies highlight the importance of geographic location and environmental factors in disease acquisition. Additionally, zoonotic transmission has been suggested as a possible cause for infection.(10)
Presentation
There are two main forms of microsporidia keratitis: keratoconjunctivitis, seen more commonly in the immunosuppressed, and stromal keratitis, which is predominant in the immunocompetent. Keratoconjunctivitis is more common; however, there has been an increase in confirmed cases of microsporidia stromal keratitis even in the United States.(11) Microsporidia keratitis presents non-specifically with injection, tearing, decreased visual acuity, pain, foreign body sensation, and photophobia. Patients may have a history of exposure to contaminated water or soil.
In the keratoconjunctivitis form, ophthalmic examination will uncover conjunctival injection alongside multiple coarse corneal punctate lesions that stain with fluorescein and vary in size and distribution.(12, 13) These findings can look like adenovirus keratitis. In cases of stromal keratitis, examination reveals conjunctival injection accompanied by stromal edema and opaque mid to deep stromal infiltrates. Features of disciform keratitis can be seen as well. Disease progression can result in stromal thinning, vascularization, and scarring.(14, 15) Suppuration is not a feature of either form of microsporidia keratitis and should prompt consideration of alternative causes of keratitis. A study has reported interstitial keratitis thought to be due to an immune reaction to microsporidial antigens and presenting with nummular corneal lesions and stromal edema.(16)
Diagnosis
The small size of microsporidia poses a diagnostic challenge, yet various methods have proven successful at detecting spores. Visualization of polar tubules on tissue biopsy with transmission electron microscopy remains the gold standard for microbiological diagnosis and species identification, but this is expensive, time consuming, and not routinely available.(17) Notably, routine corneal cultures are often negative as microsporidia are obligate intracellular organisms. Corneal scrapings, however, can be analyzed with specialized stains under light microscopy, which reveal non-budding uniform oval spores. The modified trichome stains the spore’s cell wall pink, disclosing a horizontal stripe, depicting the polar tubule, within the spore’s interior. Other stains have been used with calcofluor white and modified Ziehl-Neelsen (1% H2SO4) among the more reliable options for corneal samples.(18, 19) Immunofluorescent assays directed against spore wall or polar tubes have been used to identify E. hellem from corneal tissues and conjunctival scrapings.(20) More recently, polymerase chain reaction assays targeting species-specific rRNA coding sequences have successfully identified several microsporidia species from corneal scrapings with approximately 80% sensitivity.(21) Non-invasive methods using anterior segment optical coherence tomography can assist in the diagnosis. Imaging typically shows hyper-reflective epithelial lesions, like those seen in adenoviral keratitis, though larger in size.(22) Continued efforts are being made to enhance detection of ocular microsporidia.
Treatment
While there are no established guidelines for the treatment of microsporidia, partly due to the lack of research comparing the efficacies of different regimens, various treatments have been described anecdotally. This is especially true with microsporidia keratoconjunctivitis. Systemic Albendazole 400 mg BID, an anti-helminthic that inhibits tubulin polymerization, demonstrated efficacy in the resolution of microsporidia keratoconjunctivitis.(12, 23, 24) Others have reported success with topical antibiotics: fumagillin and fluoroquinolones. Fumagillin inhibits an enzyme involved in post translation modification of proteins. It is mixed in a saline solution and well-tolerated. In one study, microsporidia keratitis completely resolved without symptom recurrence, while another study necessitated maintenance therapy due to recurrent symptoms.(25, 26) There was one case where topical fumagillin eradicated microsporidia in stromal keratitis; however, the patient ultimately underwent a penetrating keratoplasty due to the development of bacterial keratitis.(11) A retrospective study in Singapore showed that 101 of 102 patients with superficial keratitis were successfully treated with topical fluoroquinolone monotherapy with only three cases of recurrent infection.(4) The fluoroquinolones used include ciprofloxacin 0.3%, gatifloxacin 0.5%, levofloxacin 0.5%, moxifloxacin 0.5% or norfloxacin 0.3% and treatment duration was individually tailored to the clinical response of each patient. Topical antifungals, specifically voriconazole, also have a role in treatment. Application of 1-2% topical voriconazole every two hours over several weeks has treated several cases of microsporidia keratoconjunctivitis without recurrence or treatment complications.(9, 27)
In contrast to superficial infections, stromal keratitis has limited pharmacologic options. Few cases have been successfully treated with medication using some combination of oral albendazole, topical voriconazole, polyhexamethylene biguanide, and chlorhexidine. An overwhelming majority of patients with stromal keratitis required surgery.(11, 28, 29) Penetrating keratoplasty is the surgery of choice, as lamellar keratoplasty is ineffective at preventing recurrence.(30)
DIAGNOSIS: Microsporidia keratitis
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
MANAGEMENT
|
Related Tutorial: Cornea Culture
Hansen D, Jones MT, Donegan P, Matharu KS. Microsporidial Keratitis in an Immunocompromised Patient. EyeRounds.org. January 22, 2025. Available from https://EyeRounds.org/cases/362-microsporidial-keratitis.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links