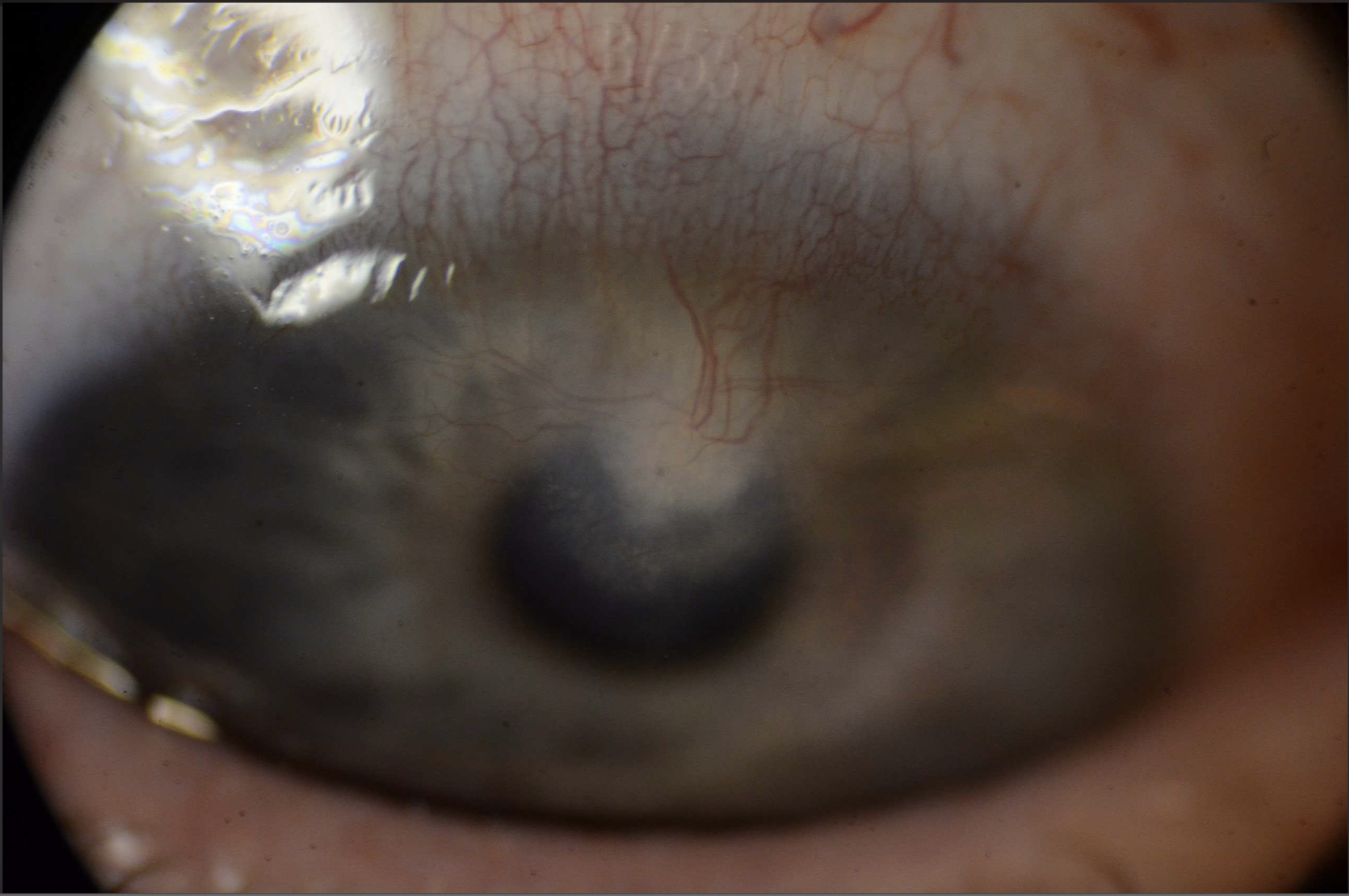
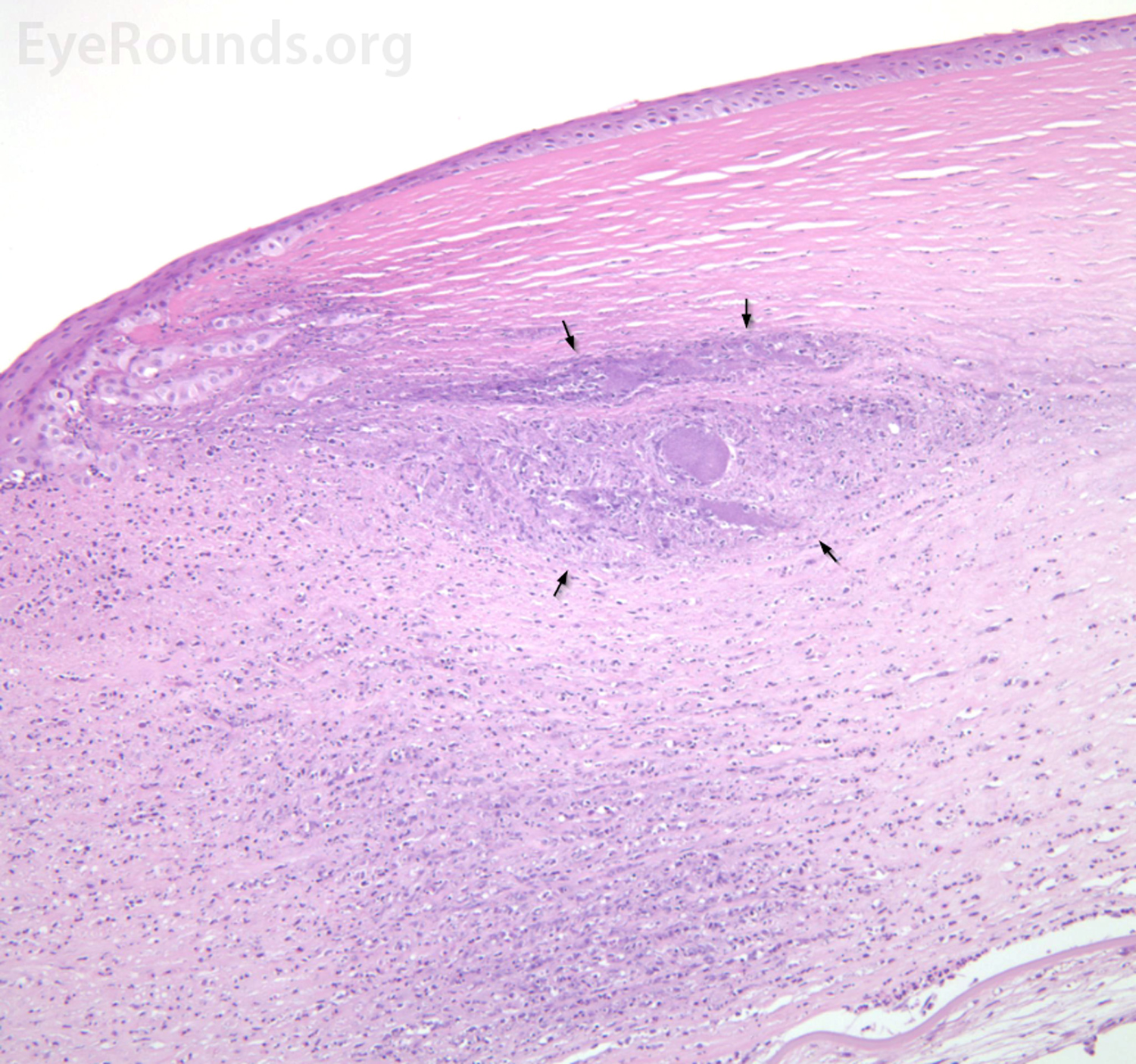
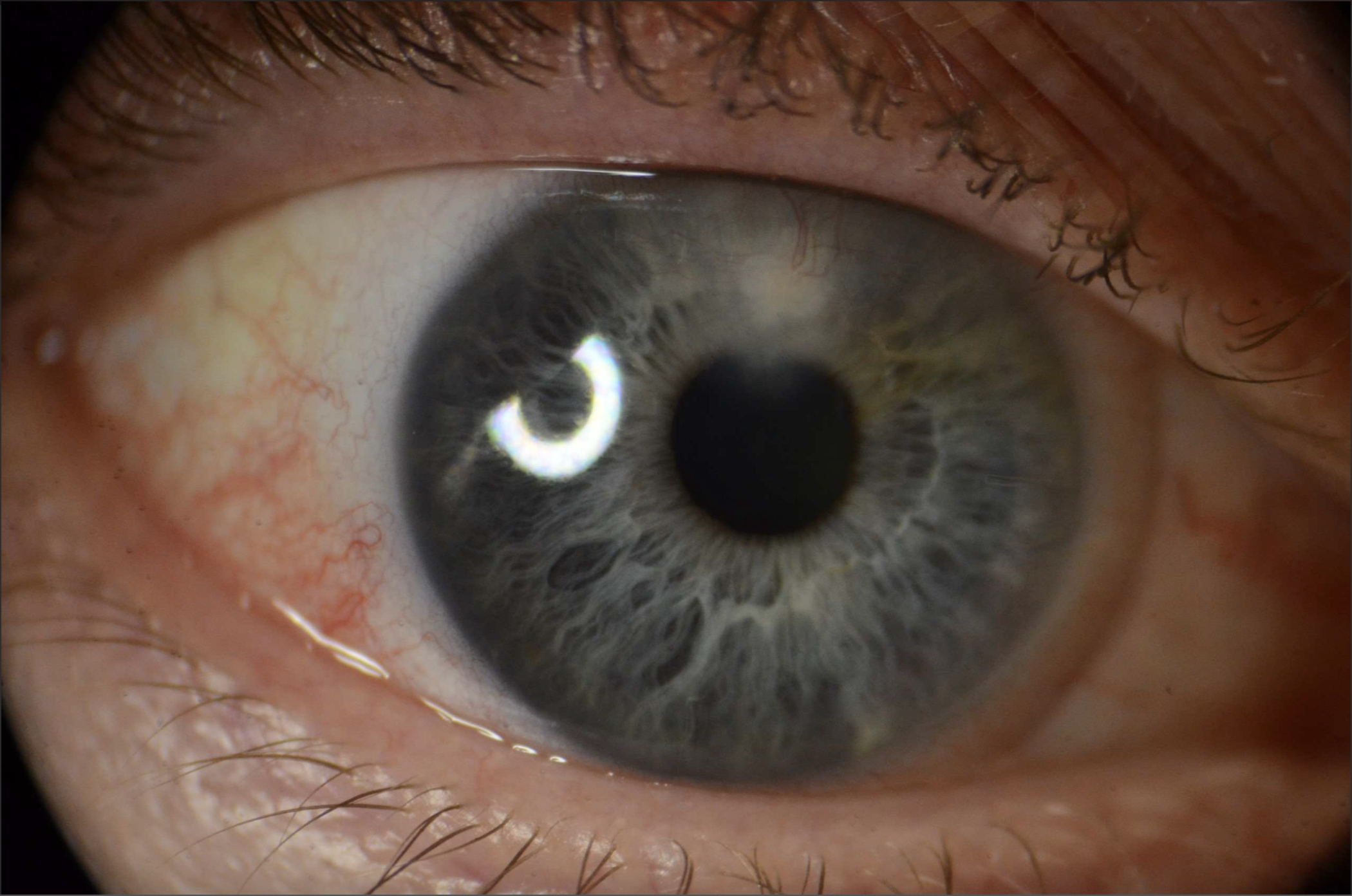
This 73-year-old male patient presented to the Cornea service with a one-week history of right eye redness and pain. He had a remote history of open globe with multiple subsequent penetrating keratoplasties and a recent macula-involving retinal detachment all in the right eye with resulting hand motions vision. He was diagnosed with suture-related infectious crystalline keratopathy with associated epithelialized stromal melt. The dense crystals seen within the deep stroma represent arborizing aggregates of an infectious agent, often alpha-hemolytic streptococcus or Candida albicans, and often originating from a suture track. Microbial colonies proliferate within stromal lamellar spaces and are shielded by a biofilm [1]. Corneal cultures are often negative. Lack of host inflammatory response may be due to chronic immunosuppression, tear film irregularity, or suture [2].
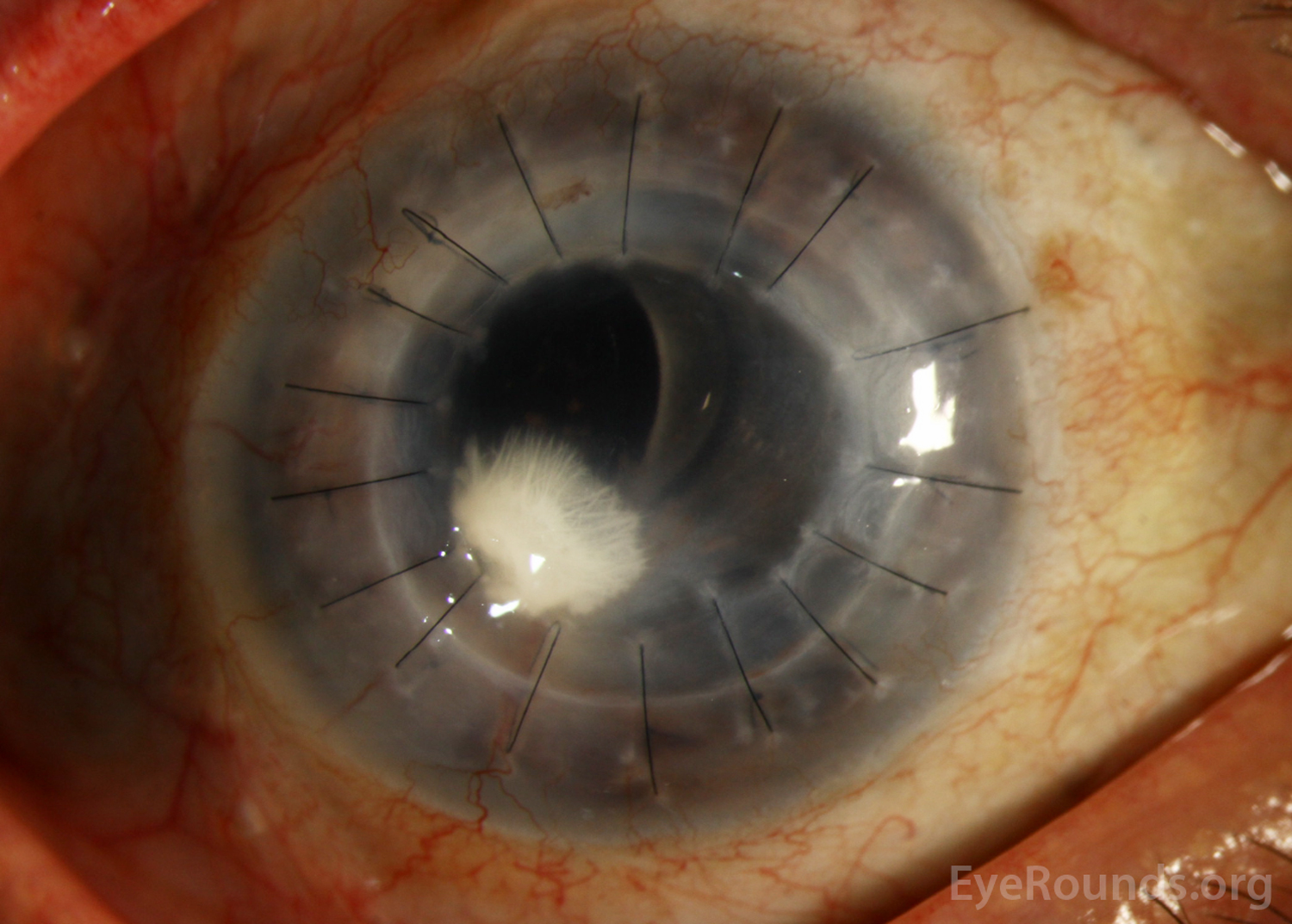

A 59-year-old male presented with pain, erythema, and photophobia in the right eye. He had a history of laser-assisted in situ keratomileusis (LASIK) and contact lens wear, including regularly sleeping in contact lenses. Prior to presentation, he had been treated with topical moxifloxacin, prednisolone, tobramycin-dexamethasone, and cyclopentolate. Despite these interventions, his symptoms persisted. His best corrected visual acuity was 20/30 in the right eye. Slit lamp examination revealed a 2 x 2 mm full thickness infiltrate with fluffy margins and minimal neovascularization. Empiric treatment for fungal keratitis was started with natamycin 6 times a day in the right eye. Symptoms improved, but at his next follow-up appointment two weeks later, the infiltrate remained and the right eye developed anterior cell. The patient underwent a LASIK flap lift and scrape of the right eye for polymerase chain reaction, slides, and culturing, as well as betadine wash and washout. Cultures grew Micrococcus luteus, a ubiquitous, gram-positive, obligate aerobe found in various aquatic and terrestrial environments.[1,2] Treatment with voriconazole, moxifloxacin, neomycin-bacitracin-polymyxin, and fluorometholone was added. At his follow-up appointment 11 days later, his best corrected visual acuity improved to 20/20 in the right eye. The patient developed a crystalline infiltrate at the superior hinge of the LASIK flap extending into the paracentral cornea with superficial and deep neovascularization and was diagnosed with infectious crystalline keratopathy (ICK). ICK presents as needle-shaped opacities comprising the persistent colonization of an infectious organism that typically extends into the anterior stroma in a branching pattern. The development of ICK is often associated with localized immunosuppression (in this case, fluorometholone), which limits the inflammation that is typically associated with infection in the affected tissues.[3]
This 73-year-old male patient presented to the Cornea service with a one-week history of right eye redness and pain. He had a remote history of open globe with multiple subsequent penetrating keratoplasties and a recent macula-involving retinal detachment all in the right eye with resulting hand motions vision. He was diagnosed with suture-related infectious crystalline keratopathy with associated epithelialized stromal melt. The dense crystals seen within the deep stroma represent arborizing aggregates of an infectious agent, often alpha-hemolytic streptococcus or Candida albicans, and often originating from a suture track. Microbial colonies proliferate within stromal lamellar spaces and are shielded by a biofilm [1]. Corneal cultures are often negative. Lack of host inflammatory response may be due to chronic immunosuppression, tear film irregularity, or suture [2].
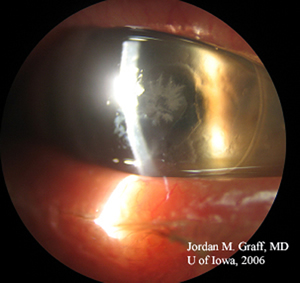
Infectious crystalline keratopathy in corneal transplant graft. Often strep viridans is the culprit.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links