
Chief Complaint: 50-year-old male with penetrating globe injury OD
History of Present Illness: A 50-year-old Caucasian male sustained an injury to the right eye hours before presentation to the University of Iowa emergency department. He stated that he was sitting outside on his lawn while his son was mowing the grass. Suddenly, a hard object hit the patient's right eye at high velocity, knocking him out of his chair. He felt immediate pain that was 10/10 in severity and experienced loss of vision. The patient was not wearing safety glasses. He was seen at a local emergency room and then transferred to the University of Iowa for definitive care.
Past Ocular History: He denied previous trauma or ocular surgery. He had no prior refractive error and wore over-the-counter readers only. He had no history of contact lens use.
Medical History: Hypertension, cancer, hernia repair. He was currently being worked up for diabetes. He had stepped on a nail last year and received a Tetanus booster at that time.
Medications: Tylenol® (acetaminophen) as needed.
Family History: Unknown.
Social History: The patient was a retired truck-driver. He reported smoking 3-4 cigarettes a day, occasional alcohol use, and a history of cocaine abuse. He denied intravenous drug use and current illicit drug use. He had been a prisoner at a local correctional facility about 10 years ago.
 |
 |
 |
 |
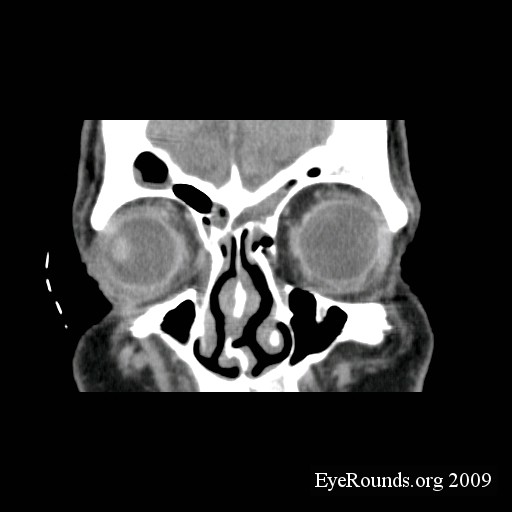
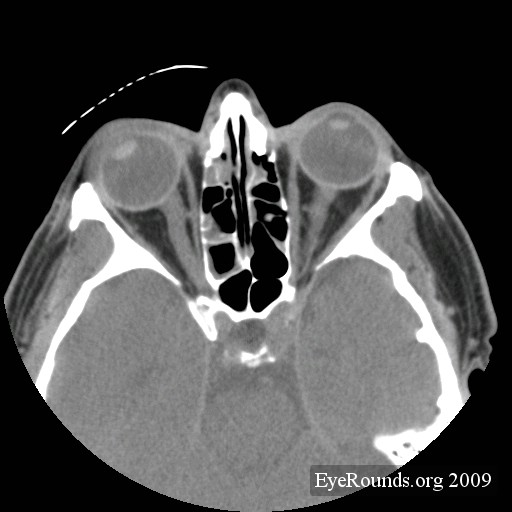
It was determined that the patient had a large corneoscleral laceration with uveal prolapse, necessitating repair and possible lensectomy. Orders were written for NPO status, elevation of the head, and a Fox shield to the right eye. Moxifloxacin 400mg IV was given and pain and nausea were controlled with intravenous morphine and ondansetron.
The exam findings, diagnosis and plan were communicated to the patient and he agreed to proceed with surgery. Informed consent was obtained and the patient was brought to the operating room. Prior to the administration of any sedation, the patient suddenly decided that he did not want to have surgery on his injured eye. During a long discussion, he was warned that he would likely lose his right eye and that he would be at risk for sympathetic ophthalmia if a surgery was not performed. All members of the treatment team were noted to be compassionate and professional during the encounter. He continued to insist on leaving without being treated. Since he was rational and not sedated the treatment team had no option other than to release him from the operating room.
The patient then signed a statement reading: I, [name of patient], refuse surgery on my right eye. I recognize that this could cause blindness and that antibodies from this eye could destroy my left eye.
An attempt was made to schedule follow up for him, but he insisted that he did not want to return to the University. We asked if there was someone to whom we could forward his medical information should he decide to seek care locally. but he informed us that he had no plans to seek local care. Social services had been contacted while the patient was in the emergency room. They determined that he was concerned about his insurance status, but financing options had been offered to him.
This clinical encounter uncovered several real and potential ethical issues: 1) determining decision making capacity, 2) balancing respect for a patient's right to autonomy and refusal of treatment with the physician's obligation to provide the best standard of care (beneficence), and 3) termination of the physician-patient relationship in the setting of non-compliance.
Determining decision making capacity: Physicians are often called upon to assess a patient's ability to make medical decisions, especially when the decision made by the patient conflicts with the physician's recommendations. Decision-making capacity refers to a person's psychological and legal ability to make a specific medical decision. Competence, on the other hand, refers to a person's ability to make global health care decisions and is determined by a court of law [#Lo">Lo 1990].
There are no specific legal criteria to determine decision-making capacity [#Lo">Lo 1990]. However, it is generally accepted in the medical-legal community that a patient has decision-making capacity if he or she can:
The decision should also be consistent with his or her values and goals and not a result of delusions. For the physician who is not well acquainted with the patient, talking with family members or friends may be necessary. Several resources provide specific questions that one might ask to address the above criteria [#Tunzi">Tunzi 2001]. In general, these open-ended questions are designed to have patients explain in their own words what they believe about their medical condition, how the recommended treatment will affect their condition, and why they have made a particular decision. One may have to address anticipated barriers to decision making, such as whether or not the patient trusts the doctor enough to give honest answers. Although it is not generally required, one should avoid asking close-ended questions to which a patient may answer yes or no , because of the risk of misunderstanding.
Psychiatric consultation may be helpful at times, but the attending physician or primary physician in charge of any particular patient encounter is ultimately responsible for determining decision-making capacity. Because the level of patient understanding in determining capacity is subject to interpretation, some have recommended using a sliding scale that balances the risk of treatment versus no treatment to help decide to what degree a patient should exhibit understanding [#Lo">Lo 1990, #Tunzi">Tunzi 2001]. For example, if the procedure for which one is obtaining consent is life-saving and has very little risk, but the patient refuses, the physician would want to ensure that the patient has a relatively sophisticated level of understanding. On the other hand, if one is trying to diagnose dry eye by performing a Schirmer's test and the patient refuses, one might be satisfied with the patient having a very simple understanding of the procedure. If a person is determined to be a threat to him or herself or others, one may involuntarily commit a patient, but this does not give the physician permission to administer treatment. If the patient does not have decision making capacity, seek advanced directives or surrogate decision making.
In this case, the physician had a long discussion with the patient and documented a summary of the discussion as well as the summary statement signed by the patient.
Right to refusal of treatment: Western culture often regards patient autonomy as more important than a physician's duty to act with beneficence [#Lo">Lo 1990]. However, allowing the patient to refuse a physician's recommendations places both the patient and physician at considerable risk. While the patient may suffer from vision-, health- or life-threatening conditions because of the inability to diagnose or treat the disease, the physician is also at risk because they can be sued for failure to diagnose, treat, monitor, follow-up or adequately explain the risks of treatment refusal [Menke 2008]. The situation also compromises the patient-health provider relationship in that misunderstanding of motives and strong emotions on both sides may result in mutual mistrust and/or disrespect, whether intentional or not.
However, adult patients who are able to make medical decisions (see Determining Decision Making Capacity) have the right to refuse recommended care as long as they have enough information to make an informed decision. The burden of responsibility is on the physician to educate the patient and presume that the patient is ignorant until educated about their condition. If the patient's noncompliance contributes later to a poor outcome, a jury in a court of law will assign a patient part of the blame [Menke 2008].
When the physician and patient have an established relationship, one may choose to deal with compliance by continuing to follow the patient (meanwhile educating and mobilizing all members of the staff to be more careful about providing information to patients), or by terminating the therapeutic relationship.
The Ophthalmic Mutual Insurance Company (OMIC) provides two useful approaches for dealing with noncompliance.
ICEDD (Identify, Clarify, Educate, Decide, Document)
SIRAD (Schedule, Identify, Review, Act, Document) is a method for organizing and documenting scheduled visits, cancellations, and no shows. This approach is outlined in further detail at http://www.omic.com/resources/risk_man/recommend.cfm#noncompliance
Where does my responsibility end?
There is no clear cut answer to how much follow up is enough. It depends on the severity of the condition. For this patient, we attempted to make a follow up appointment and sent a certified letter to the patient's house. When he did not return for a follow up appointment, another phone call was made and another letter was sent. In general, the safest approach is to follow up on all missed appointments and schedule as many appointments as reasonably necessary to provide adequate care or to arrange for care elsewhere. Risk management often provides helpful advice and was also consulted in this situation.
Occasionally, a patient may be referred by another physician and never shows up to the appointment. In this situation, OMIC recommends notifying the referring physician that the patient did not show up for or cancelled the appointment. Clarify that the referring doctor will follow up with the patient. Send a fax to the referring physician confirming that he or she was notified of the no-show that the referring physician agreed to follow up with the patient. If the referring physician cannot be reached or the referring physician does not agree to follow up with the patient, send the patient a missed appointment or noncompliant letter [Menke 2008].
Document all calls with patients and other providers. Keep copies of letters sent to patients and other providers in the medical record.
Terminating the physician-patient relationship.
Although it may seem as though the little interaction between the physician and the patient in this case would be insufficient to establish a physician-patient relationship, legal precedence shows that even a phone conversation may be enough to do so. In O'Neill v. Montefiore Hospital, the court ruled that a physician who attempts to diagnose a patient's condition over the phone enters into a physician-patient relationship [Lo 1990, O'Neill v Montefiore Hospital, 202 NYS2d 436 (1960)].
Once a relationship between an ophthalmologist and patient has been established, the physician is obligated to treat the patient until the physician's services are no longer needed, the patient dismisses the physician, or the patient and physician mutually agree to terminate the relationship. Occasionally, the physician may decide to unilaterally terminate the relationship. However, he or she must provide reasonable notice supported by documentation and sufficient time for the patient to secure other care if desired, or the termination may be viewed as patient abandonment.
In this case, the patient effectively dismissed the physician's services, but it is conceivable that the patient could argue in the future that, while he refused the treatment, he actually wanted to continue the therapeutic relationship. To prevent any later misunderstanding, the ophthalmologist should send a letter to the patient confirming the termination of the relationship and, if possible, provide all pertinent medical information to the patient's subsequent physician. The letter should include as appropriate a statement advising the patient that he or she needs further care [sample letter available at OMIC site]. As long as the physician can demonstrate in the medical record that the patient had a clear record of refusing care or failure to keep or reschedule appointments, the patient generally cannot claim abandonment [Stromberg 1992]. In this situation, we offered to communicate with any future physician with whom he desired to establish care, but the patient declined.
In summary, interacting with non-compliant patients is a challenging situation that most physicians will face during their careers. Taking time to understand why a patient is making a particular decision and addressing their particular misconceptions or fears often helps to resolve the issue. However, occasionally, despite the most conscientious efforts, the patient may still choose to refuse recommended treatment. In our culture, we tend to allow the patient's choice to prevail. If there is an irresolvable disagreement between the patient and physician in how to proceed with management, the physician should carefully document all discussions and efforts to provide the best care reasonably possible.
>Tsui, J., Alward, W.L.M. Patient Non-Compliance: Physician responsibility. EyeRounds.org. January 24, 2010 Available from: http://www.EyeRounds.org/cases/106-Patient-Noncompliance.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
