Chief Complaint: Referred for unequal vision
A 5-year-old male was referred by his local optometrist for suspected decreased vision in his left eye found on a screening exam. His mother had not noticed any vision problems. He has had normal growth and development.
Past Ocular History: None
Past Medical and Surgical History: None
Medications: None
Family History: No history of amblyopia or strabismus
Social History: Lives at home with mother and father
Review of Systems: All systems negative
Pupils: No relative afferent pupillary defect OU
Extraocular motility: Normal versions, flick of exophoria in primary position at distance and near
Confrontation visual fields: No deficits OU by toys
Intraocular pressure: Soft on palpation OU
External exam: Normal
CLINICAL COURSE: The patient was given his cycloplegic refraction minus 0.75 D to encourage compliance and followed at three-month intervals (see exams below).
OD: OS: |
+0.75 +0.50 x 090 +2.75 +1.75 x 105 |
-0.75D → -0.75D → |
Prescribed refraction plano +0.50 x 090 +2.00 +1.75 x 105 |
In the first year of treatment, his vision improved to 20/30 with glasses alone and his stereoacuity was almost full. Vision and stereoacuity remained stable at yearly exams over the next 2 years (until age 8) at which point the patient's mother discontinued the glasses on her own. At age 9, his vision was found to have slipped a line and he had a slight decrease in stereoacuity consistent with discontinuation of glasses. The patient's mother declined a trial of patching, and his full correction was resumed.
Worth 4 Dot Test: Fusion at near
Causes of Amblyopia (in order of frequency): Strabismus, anisometropia, high bilateral ametropia, stimulus deprivation (e.g. congenital cataract)
Amblyopia is a major cause of preventable vision loss. A Pediatric Eye Disease Investigator Group (PEDIG) study showed that anisometropia was a contributing factor in 61% of patients presenting for initial evaluation of amblyopia (PEDIG 2002). It was the only identifiable amblyogenic factor in 37%. It is believed that unequal refractive error results in amblyopia due to a combination of chronic image blur and central inhibition of the visual signal originating from the affected eye. In the present case, the patient had significant anisometropia with differences in the hyperopic and astigmatism correction between the two eyes (amblyopia is clinically defined by a difference in vision of =2 lines between the eyes). Hyperopic anisometropia is more amblyogenic and more common than myopic and astigmatic anisometropia in children (Kutschke 1991). In this case, he had hyperopic anisometropia as well as astigmatism contributing to his anisometropia. The American Academy of Ophthalmology has consensus guidelines for prescribing optical correction to children with anisometropia that are based on the type of refractive error (see table 1).
AAO Consensus Guidelines for Prescribing Eyeglasses in Anisometropia by Age |
|||
|
0-1 years |
1-2 years |
>3 years |
Myopia |
≥ -2.50 |
≥ -2.50 |
≥ -2.00 |
Hyperopia |
≥ +2.50 |
≥ +2.00 |
≥ +1.50 |
Astigmatism |
≥ 2.50 |
≥ 2.00 |
≥ 2.00 |
Anisometropic amblyopia has been reported to occur with as little as one diopter difference between the two eyes (Kutschke 1991). In recent years, therapy with glasses alone has become more acceptable and has been shown to improve vision ≥ 2 lines in 77-93% of patients with complete resolution of amblyopia in 27-45% (PEDIG 2006, Chen 2007). Treatment effect appears to plateau around 2 months. If severe amblyopia is present at presentation (defined by the Amblyopia Treatment Study Group as visual acuity 20/100 20/400), patching or pharmacological penalization may be added. However, patching or atropine must be considered in addition to optical management if patients show no improvement with glasses alone after 3-5 months.
It has been thought that visual maturity occurs between the ages of 6 and 9 years (Scott 1988). However, a growing number of studies are showing a response to amblyopia treatment in older patients (Menon 2008). In 2005, PEDIG reported that amblyopia improved with optical correction alone in about one fourth of patients aged 7 to 17 years, with 15% of patients improving when first treated in their teens (Scheiman 2005). This supports the need for treatment through the first decade of life and possibly into the second decade of life.
Patient compliance with glasses wear is a frequent challenge in the treatment of anisometropic amblyopia. It is especially difficult in very young patients as they are often unable to notice a subjective improvement in their vision with the glasses on. Discussion with the parents about the need for continued glasses wear and the risk of recurrence is important to successful treatment as can be demonstrated by the slip in visual acuity in our patient. It is important for parents to understand that continued spectacle correction is critical until visual maturity even when apparent stability has been achieved.
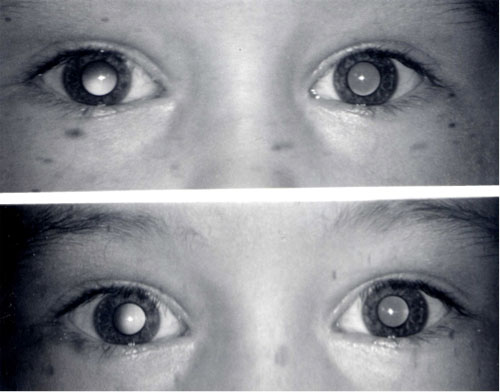
There are few life-altering diseases in medicine with a better cost/benefit ratio in terms of treatment. The challenge is to be able find the affected children. Effective screening and early diagnosis are key public health concerns in addressing anisometropic amblyopia as late diagnosis and poor initial acuity portend a poor response to treatment (Hussein 2004). Use of the Bruckner test is an easy and effective method for detecting anisometropia by pediatricians and other non-ophthalmic professionals (see below). This can be done quickly in the office and prompts a referral to an ophthalmologist or optometrist. Large-scale screening efforts such as the Iowa KidsSight program using instruments like the MTI photoscreener (Medical Technologies, Inc, see Figures 2 and 3) have been successful at identifying amblyopia risk factors for a large percentage of children (Longmuir 2010). This screener has a high positive predictive value for anisometropia (96%). Amblyopia continues to be a significant public health problem, affecting 2% to 5% of the population. When diagnosed and treated early in life, the visual loss may be reversed, which supports the need for early identification and treatment of anisometropia.
|
|
|
|
EPIDEMIOLOGY:
|
SIGNS:
|
SYMPTOMS:
|
TREATMENT:
|
"Amblyopia." Preferred Practice Patterns : American Academy of Ophthalmology. Available at http://one.aao.org/CE/PracticeGuidelines/PPP_Content.aspx?cid=930d01f2-740b-433e-a973-cf68565bd27b%3E
Astle WF, Rahmat J, Ingram AD, Huang PT. Laser-assisted subepithelial keratectomy for anisometropic amblyopia in children: outcomes at 1 year. J Cataract Refract Surg 2007; 33: 2028-2034.
Birch E, Holmes J. The clinical profile of amblyopia in children younger than 3 years of age. J AAPOS 2010; 14: 494-497.
Chen P, et al. Anisometropic amblyopia treated with spectacle correction alone: possible factors predicting success and time to start patching. Am. J. Ophthalmol 2007; 143: 54-60.
Donahue SP. The relationship between anisometropia, patient age, and the development of amblyopia. Trans Am Ophthalmol Soc 2005; 103: 313-336.
Friedman DS, et al. Prevalence of amblyopia and strabismus in white and African American children aged 6 through 71 months: the Baltimore Pediatric Eye Disease Study. Ophthalmology 2009; 116: 2128-2134.
Hussein MAW, Coats DK, Muthialu A, Cohe, E, Paysse EA. Risk factors for treatment failure of anisometropic amblyopia. J AAPOS 2004; 8: 429-434.
Kutschke PJ, Scott WE, Keech RV. Anisometropic amblyopia. Ophthalmology 1991; 98:258-263.
Lin X, et al. Long-term efficacy of excimer laser in situ keratomileusis in the management of children with high anisometropic amblyopia. Chin. Med. J 2009; 122:813-817.
Longmuir SQ, et al. Nine-year results of a volunteer lay network photoscreening program of 147809 children using a photoscreener in Iowa. Ophthalmology 2010; 117: 1869-1875 .
Menon,V. Shailesh G, Sharma P, Saxena R. Clinical trial of patching versus atropine penalization for the treatment of anisometropic amblyopia in older children. J AAPOS 2008; 12:493-497.
Pai A, Mitchell P. Prevalence of Amblyopia and Strabismus. Ophthalmology 2010; 117:2043-2044.
Paysse EA, Williams GC, Coats DK, Williams EA. Detection of Red Reflex Asymmetry by Pediatric Residents Using the Bruckner Reflex Versus the MTI Photoscreener. Pediatrics 2001; 108:e74.
PEDIG: Pediatric Eye Disease Investigator Group. The clinical profile of moderate amblyopia in children younger than 7 years. Arch. Ophthalmol 2002; 120:281-287.
Pirouzia, Ip KC. Refractive surgery in the pediatric population. Arch. Ophthalmol 2010;128: 1380-1381; author reply 1381-1382.
Scheiman MM, et al. Randomized trial of treatment of amblyopia in children aged 7 to 17 years. Arch. Ophthalmol 2005; 123:437-447.
Scott WE, Flabetich Dickey C. Stability of visual acuity in amblyopic patients after visual maturity. Graefe's Arch Clin Exp Ophthalmol 1988; 226:154-157.
Steele AL, et al. Successful treatment of anisometropic amblyopia with spectacles alone. J AAPOS 2006; 10: 37-43.
Utine C, Cakir H, Egemenoglu A, Perente I. LASIK in children with hyperopic anisometropic amblyopia. J Refract Surg 2008; 24:464-472.
Ward M, Pfeifer WL, Longmuir SQ. Anisometropic Amblyopia: 5-year-old male with unequal vision. EyeRounds.org. July 1, 2011. Available from: https://eyerounds.org/cases/134-anisometropic-amblyopia.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links