
Chief Complaint: Orbital swelling and pain
A 52-year-old male with poorly-controlled type 2 diabetes presented to the emergency room with left eyelid swelling. Two days prior, the patient presented to an outside ophthalmologist because he believed the swelling was due to a stye. He was treated with oral antibiotics and warm compresses. Over 24 hours, the patient's condition progressed and he noted severe swelling that started the morning of presentation to the emergency room. Purulent drainage in the surrounding soft tissues was also noted by the patient. The patient felt severe, 8/10, sharp pain in the left eye and surrounding tissues that was exacerbated by palpation and movement of the eye. The patient also noted that he felt very warm earlier in the day, but he did not measure his temperature.
Past Ocular History: None
Medical History
Medications
Allergies
Family History: Non-contributory
Negative for chills, chest pain, neck stiffness, shortness of breath, abdominal pain, nausea, dysuria, diarrhea, and lower extremity edema. Positive for vomiting and increased thirst.
Right eye (OD): 20/40
Left eye (OS): 20/40
OD: 15 mmHg
OS: 57* mmHg
*Decreased to 34 mmHg after canthotomy/cantholysis
OD: 3 mm in dark, 2.5 mm in light, brisk, and no relative afferent pupillary defect (RAPD)
OS: 3 mm in dark, 3 mm in light, minimal reactivity, and 1+ RAPD*
*subjective dim vision OS compared to OD
OD: Full
OS: Full
OD: Full
OS: -3 in all gaze directions
Tense left upper and lower eyelids, warmth, erythema with purplish hue, and edema extending to the upper and lower eyelid margin (Figure 1). Few eschars on the left upper lid with purulent drainage. Left-sided proptosis. No hypoesthesia of the face, no black eschars of palate or nasal mucosa. Pain not out of proportion to exam. Moist pharynx without erythema or exudate. Very poor dentition with multiple dental caries.

Figure 1. Tense left upper and lower eyelids, warmth, erythema with purplish hue, and edema extending to the upper and lower eyelid margin. Few eschars with purulent drainage.
OD: Only remarkable for trace nuclear sclerosis.
OS: 360 degree hemorrhagic chemosis. Trace nuclear sclerosis.
Normal bilaterally
(Elevated abnormal values are HIGHLIGHTED in RED)
The otolaryngology and infectious disease teams were consulted due to the rapidity and severity of the patient's condition and the concern for necrotizing fasciitis. An emergent canthotomy/cantholysis was performed to reduce intraocular pressure; the pressure decreased from 57 mmHg to 34 mmHg immediately following the procedure. Cultures were obtained and sent from the purulence found on his eyelids. Imaging (CT) was obtained in the emergency center that showed a 1.4 x 0.9 cm cutaneous fluid collection in the left parietal region in addition to preseptal and orbital cellulitis with involvement of the superior rectus muscle (Figure 2). The patient was admitted for intravenous clindamycin 900 mg every 8 hours, vancomycin 1000 mg every 8 hours, and ertapenem 1,000 mg every 24 hours. He was placed on vision checks every 2 hours, continuous hot compresses, and head of bed elevation. He was kept nil per os (NPO) due to the possible need for urgent surgical intervention. After examining the patient, the otolaryngology service had low suspicion for invasive fungal sinusitis such as Mucor. The hospital's dentistry team did not believe the infection was of dental origin even though the patient had very poor dentition. Necrotizing fasciitis continued to be high on the differential. The patient was followed very closely and within 12 hours of starting IV antibiotics, the patient continued to decline clinically.

Figure 2. CT scan showing a 1.4 x 0.9 cm left parietal cutaneous fluid collection. Left pre and post septal orbital cellulitis with involvement of the superior rectus muscle.
The eyelid margin was noted to be of a deeper blue/purple hue compared to the time of admission. Due to concern for clinical progression despite IV antibiotics, the patient was taken to the operating room emergently for wound debridement of the left upper eyelid, tissue diagnosis and further cultures.
Intraoperatively, the eyelid skin and orbicularis were noted to be necrotic. The necrotic tissues were excised and sent to pathology for frozen section. The specimen returned with signs consistent with necrosis and acute inflammation. No fungal elements were noted. This confirmed the clinical suspicion for necrotizing fasciitis. Tissue was also sent to the microbiology lab for gram stain and anaerobic, aerobic, and fungal cultures. The tissue was debrided and noted to be dusky. Debridement continued until bleeding and normal tissue planes were appreciated. Once adequate bleeding was noted, saline soaked dressings were placed over the eyelid wound with a burn dressing.
Cultures returned positive for Staphylococcus aureus and susceptibility testing confirmed Methicillin-resistant S. aureus (MRSA). Despite continuation of IV antibiotics and close monitoring, the patient's clinical course and vision continued to decline following surgery, progressing to no light perception (NLP) vision likely due to the compression of the optic nerve. A repeat MRI scan was performed and showed diffuse changes throughout the orbit with tenting of the globe (Figure 3). Due to the worsening clinical condition, exenteration was discussed with the patient, but he wished to continue the current management. Therefore, close observation and IV antibiotics were continued. After 36 hours of antibiotics, the patient clinically stabilized. The infectious disease service suggested the possibility of a synergistic polymicrobial infection (Staphylococcus and Streptococcus). It was felt there was no need to continue Gram negative coverage, but clindamycin was continued due to its ability to decrease toxin burden through the inhibition of bacterial protein synthesis at the level of the 50S ribosome (1).

Figure 3. MRI with contrast showing tenting of the globe
The patient was discharged with a peripherally inserted central catheter (PICC) line. He was treated with vancomycin 1750 mg every 12 hours IV and rifampin 500 mg twice daily orally for 27 days. Ophthalmic lubricating ointment was recommended to be placed over the left eye soft tissue wounds and wet-to-dry dressings to be covering the left eye at all times.
The patient reported for follow-up 8 days after debridement and his surgical incisions were healing well and showed adequate granulation tissue with no signs of infection (Figure 4). He reported no pain or discomfort, but did have discharge and tearing throughout the day. He continued to measure NLP vision in the left eye. Monocular precautions were discussed and polycarbonate lenses were prescribed.
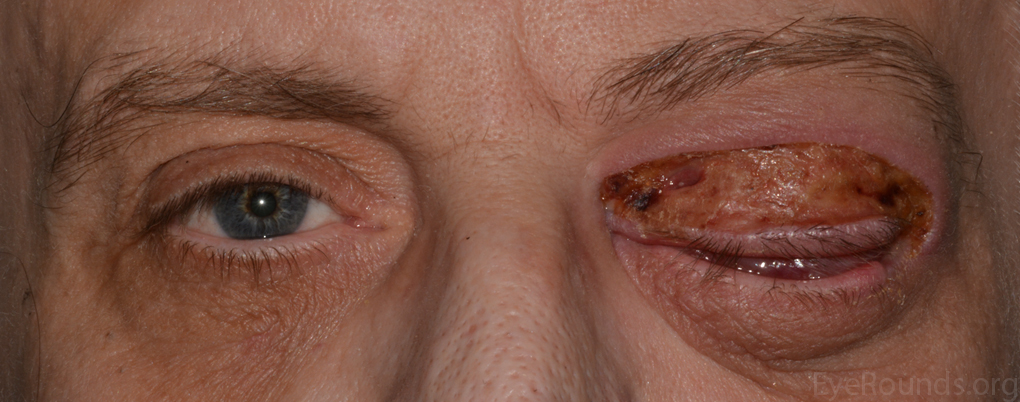
Figure 4. Post-operative appearance of the patient.
Periorbital necrotizing fasciitis
Necrotizing fasciitis is a rapidly progressive soft tissue infection with high morbidity and mortality rates. Recognition and early detection are the keys to treatment and survival. Untreated periorbital necrotizing fasciitis typically results in rapid tissue destruction and vision loss, usually within 2-4 days following initial infection (2). Initially the infection starts in the hypodermis or superficial fascia. The more superficial layers are not affected early in the disease course. Extension of the infection and necrosis is facilitated by the synergy between the bacteria, toxins, and the enzymes they produce. Necrosis of the hypodermis and superficial fascia is related primarily to the bacterial enzymes that destroy these tissues and secondarily to vascular compromise (3). Thrombosis of vessels is secondary to invasive bacteria located in the hypodermis and leads to tissue ischemia that is aggravated by the presence of edema. Tissue ischemia promotes infectious dissemination leading to further skin necrosis and provides an explanation to the intense pain phenomena that is usually involved, especially when the nerve branches are affected (3).
Necrotizing fasciitis occurs most frequently in the limbs or abdominal wall. Periorbital location is significantly less common, which is mostly attributable to the rich blood supply to the head and neck (4). The condition typically originates at sites of prior blunt or penetrating trauma though the preceding trauma is often minor and unrecognizable, such as an insect bite or abrasion (2). One report found preceding local blunt trauma in 17% of cases, penetrating injury in 22%, and facial surgery in 11%, but there was no identifiable cause in one-third of cases (5). Necrotizing fasciitis in the head and neck region can sometimes be traced from infections of dental or pharyngeal origin (6). Necrotizing fasciitis often occurs in settings of immunocompromise, including conditions of relative immunosuppression such as diabetes, alcoholism, malignancy, rheumatological disease, corticosteroid use, and chronic systemic disease, but about one-half of cases occur in individuals who were previously healthy (5).
Symptoms and signs may include localized pain, edema, erythema or violaceous coloration, crepitus, soft tissue necrosis, blistering, and findings consistent with systemic toxicity (5). Orbital signs such as proptosis, decreased vision, restricted ocular motility, and development of a relative afferent pupillary defect may occur with orbital involvement. If an orbital compartment syndrome develops, the intraocular pressure may become elevated. Non-necrotizing preseptal or orbital cellulitis may have similar signs and symptoms such as pain, periorbital edema, erythema, and fever. Because necrotizing fasciitis requires much more aggressive treatment, it is important to differentiate it from non-necrotizing infections. Initially, it may be difficult to discriminate between these conditions. Eventually, rapid progression and cyanosis of the involved tissue appearing as a dusky, violaceous discoloration, along with the formation of serous fluid-filled bullae are clues to differentiate necrotizing fasciitis from non-necrotizing preseptal and orbital cellulitis (5).
Tissue obtained during debridement may be analyzed by Gram stain and culture to aid in the diagnosis. Laboratory findings are also useful in the diagnosis of periorbital necrotizing fasciitis. A scoring system known has laboratory risk indicator for diagnosis of necrotizing fasciitis (LRINEC) is considered a robust risk indicator for the diagnosis of necrotizing fasciitis (7). The LRINEC includes total white blood cell count (WBC), c-reactive protein (CRP), hemoglobin level, serum sodium level, serum creatinine level, and the blood glucose level. The clinical score was developed on the basis of retrospective studies and has not been validated prospectively. In the case series performed by Tambe et al. (7), the scores did not correlate with the severity of the condition and the authors noted that it would be useful in the future to perform studies specific to periocular necrotizing fasciitis to determine an alternative indicator that is more sensitive for early detection than LRINEC (7).
Mortality is dependent on the location of infection with the orbital location carrying a better prognosis. The mortality observed with orbital necrotizing fasciitis is 10% (8) while the median mortality rate for all sites of infection together is 32.2% (3). The main risk factor for mortality was the organism type, since all reported cases of death in Lazzeri et al. were attributed to β-hemolytic Streptococcus alone or associated with other organisms (5).
Management of periorbital necrotizing fasciitis is centered on early recognition of clinical signs and symptoms mandating aggressive multidisciplinary treatment to avoid complications such as blindness, meningitis and other neurological disorders, and death (9). After the diagnosis is made, the mainstays of treatment are surgical debridement of the necrotic tissue and broad-spectrum intravenous antibiotics. An optimal antibiotic regimen for methicillin-susceptible S. aureus skin and soft tissue infection is oxacillin (1-2 gm intravenously, every 4 hours) with clindamycin (600 mg/kg intravenously, every 8 hours or 300-450 mg orally three times daily) (10). Lateral canthotomy and cantholysis may be required to reduce intraocular pressure if an orbital compartment syndrome develops. Hyperbaric oxygen therapy can reduce the extent of hypoxic leukocyte dysfunction occurring within an area of hypoxia and infection, and improved oxygenation to otherwise ischemic areas, thus blocking the progression of necrotizing fasciitis and perhaps saving more of the eyelid and orbital tissue (7).
Epidemiology (8,11)
|
Signs (8,12,13,14)
|
Symptoms (8)
|
Treatment (8,13,15,16)
|
Hall AJ, Baker M, Allen RC. Orbital necrotizing fasciitis. EyeRounds.org. posted January 4, 2016; Available from https://eyerounds.org/cases/227-orbital-necrotizing-fasciitis.htm<

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
