
INITIAL PRESENTATION
Chief Complaint: Decreased vision in the right eye
History of Present Illness:
A 35-year-old male presented with decreased vision, redness, and pain in the right eye after accidentally hitting himself in the eye with his fist. He had consumed multiple alcoholic beverages and while he was getting into bed his knuckle accidentally hit his right eye. He experienced immediate severe pain and decreased vision in the right eye (OD) associated with nausea for which he sought care in the UIHC Emergency Department.
Past Ocular History:
Past Medical History: Seasonal allergies
Medications: Fexofenadine as needed
Allergies: No known allergies to medication
Family History: Age-related macular degeneration - Father
Social History: Non-smoker, intoxicated at time of presentation
Review of Systems: Negative except for what is detailed in the history of present illness.
OCULAR EXAMINATION
Differential Diagnosis:
CLINICAL COURSE
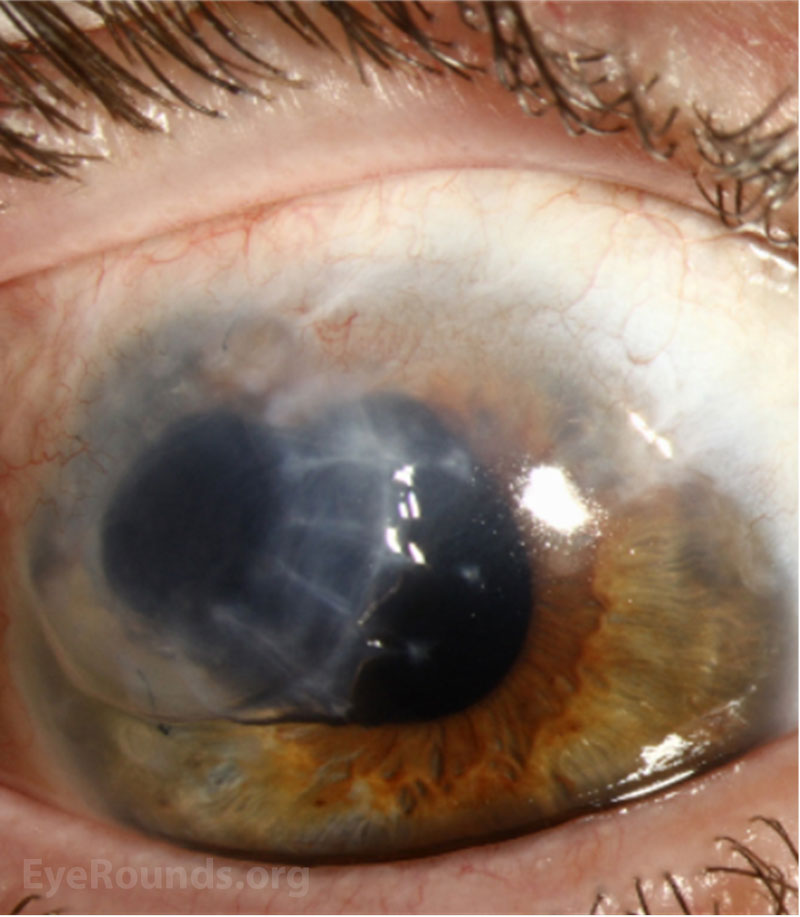
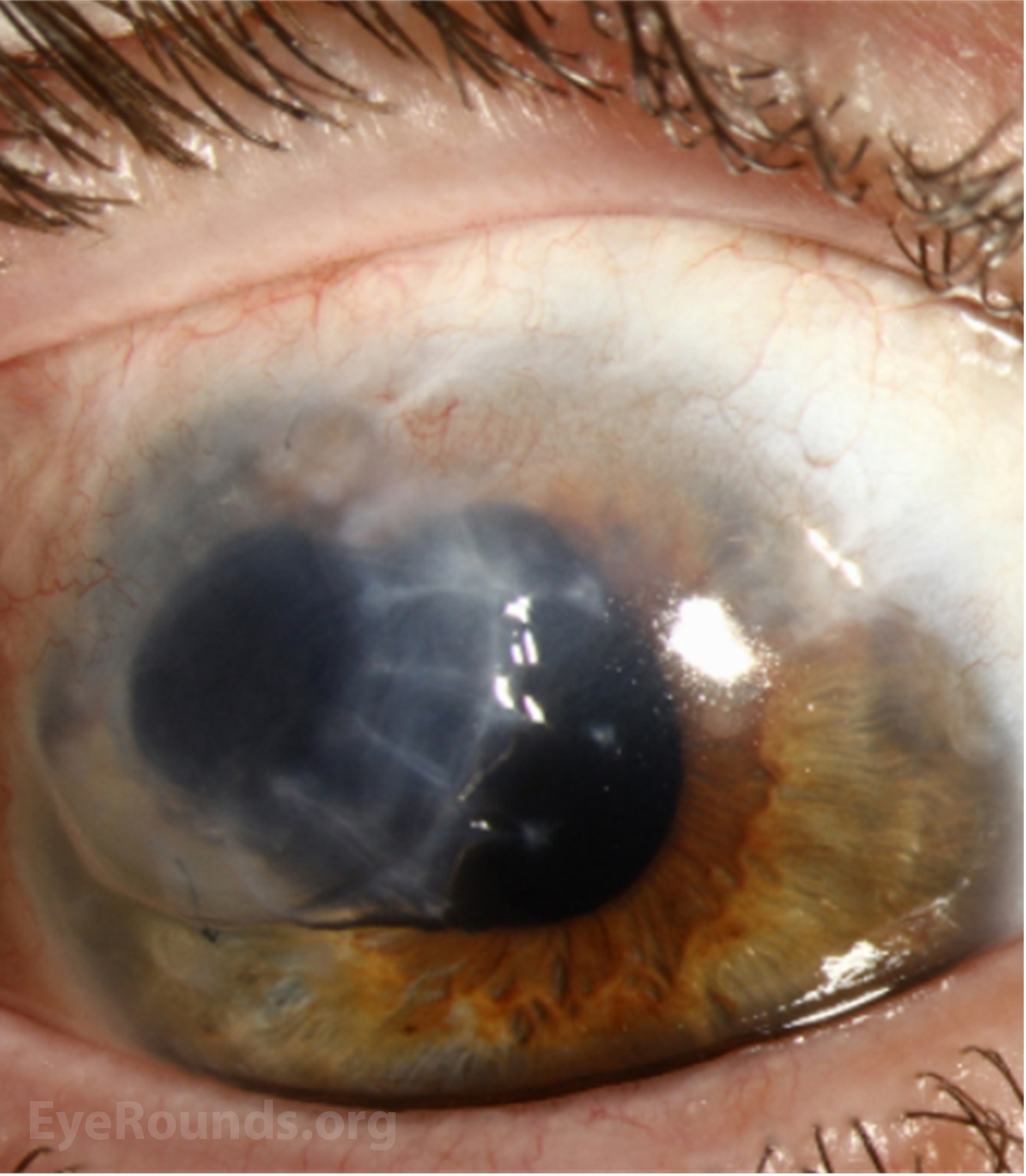
The patient underwent emergent exploration and repair of the ruptured globe with repositioning of prolapsed uveal tissue in the right eye with the Cornea service. Intraoperatively, he was found to have a stellate, full thickness 4-5 mm corneal laceration superior temporally with prolapsed iris tissue plugging the wound. The wound did not extend into sclera. Additionally, he was noted to have a nearly white cataract with a small anterior capsular tear but no visualized leakage of cortical material. The iris tissue was reposited and the corneal wound was closed with interrupted nylon sutures followed by cyanoacrylate glue due to pinpoint wound leakage.
The patient underwent emergent exploration and repair of the ruptured globe with repositioning of prolapsed uveal tissue in the right eye with the Cornea service. Intraoperatively, he was found to have a stellate, full thickness 4-5 mm corneal laceration superior temporally with prolapsed iris tissue plugging the wound. The wound did not extend into sclera. Additionally, he was noted to have a nearly white cataract with a small anterior capsular tear but no visualized leakage of cortical material. The iris tissue was reposited and the corneal wound was closed with interrupted nylon sutures followed by cyanoacrylate glue due to pinpoint wound leakage.
Three months after his initial injury he underwent superior temporal tectonic “mini” 7.0 mm penetrating keratoplasty with anterior vitrectomy and partial lensectomy in the right eye (Figure 2). A smaller graft was chosen over a full sized central penetrating keratoplasty to improve peripheral wound stability. Two weeks after his corneal transplant surgery he presented with an IOP of 31 mm Hg and increased anterior chamber inflammation in the right eye suggestive of acute phacoantigenic glaucoma. He was referred to the Retina service and underwent 23 gauge pars plana vitrectomy with lensectomy in the right eye, after which his intraocular pressure normalized and his anterior chamber inflammation resolved. He was left aphakic to allow additional time for corneal wound healing and suture removal prior to intraocular lens selection. With a custom fitted scleral contact lens his visual acuity improved to 20/20 in the right eye.
Four years after his tectonic penetrating keratoplasty, he presented with late endothelial cell failure of the mini-penetrating keratoplasty graft, thought to be due to a combination of prior intraocular inflammation and contact lens wear. Topical steroids failed to improve his corneal edema in the graft. He subsequently underwent repeat penetrating keratoplasty (8.25 mm) with secondary sutured intraocular lens and anterior synechiolysis in the right eye. An Alcon CZ70BD single-piece PMMA lens was sutured to sclera 2 mm posterior to the limbus with 8-0 Gore-Tex.
In the months following his repeat corneal transplant, he developed secondary glaucoma due to steroid response in the right eye. His IOP remained in the low 30s despite treatment with maximum topical glaucoma medications and oral acetazolamide. He underwent placement of an Ahmed tube shunt with subsequent lowering of his intraocular pressure to the mid-teens. At his most recent visit, his vision was 20/40 in the right eye with spectacle correction. The graft was clear, and the intraocular pressure was normal. He wears full time eye protection, even while sleeping, due to the increased risk of corneal perforation with minimal trauma.
DIAGNOSIS: Terrien marginal degeneration
DISCUSSION
Introduction
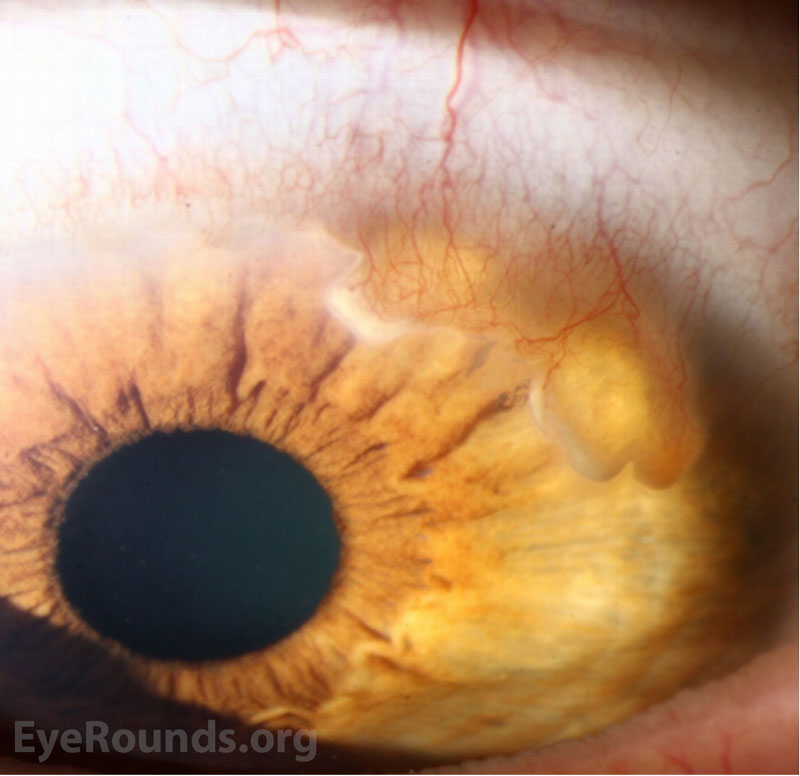
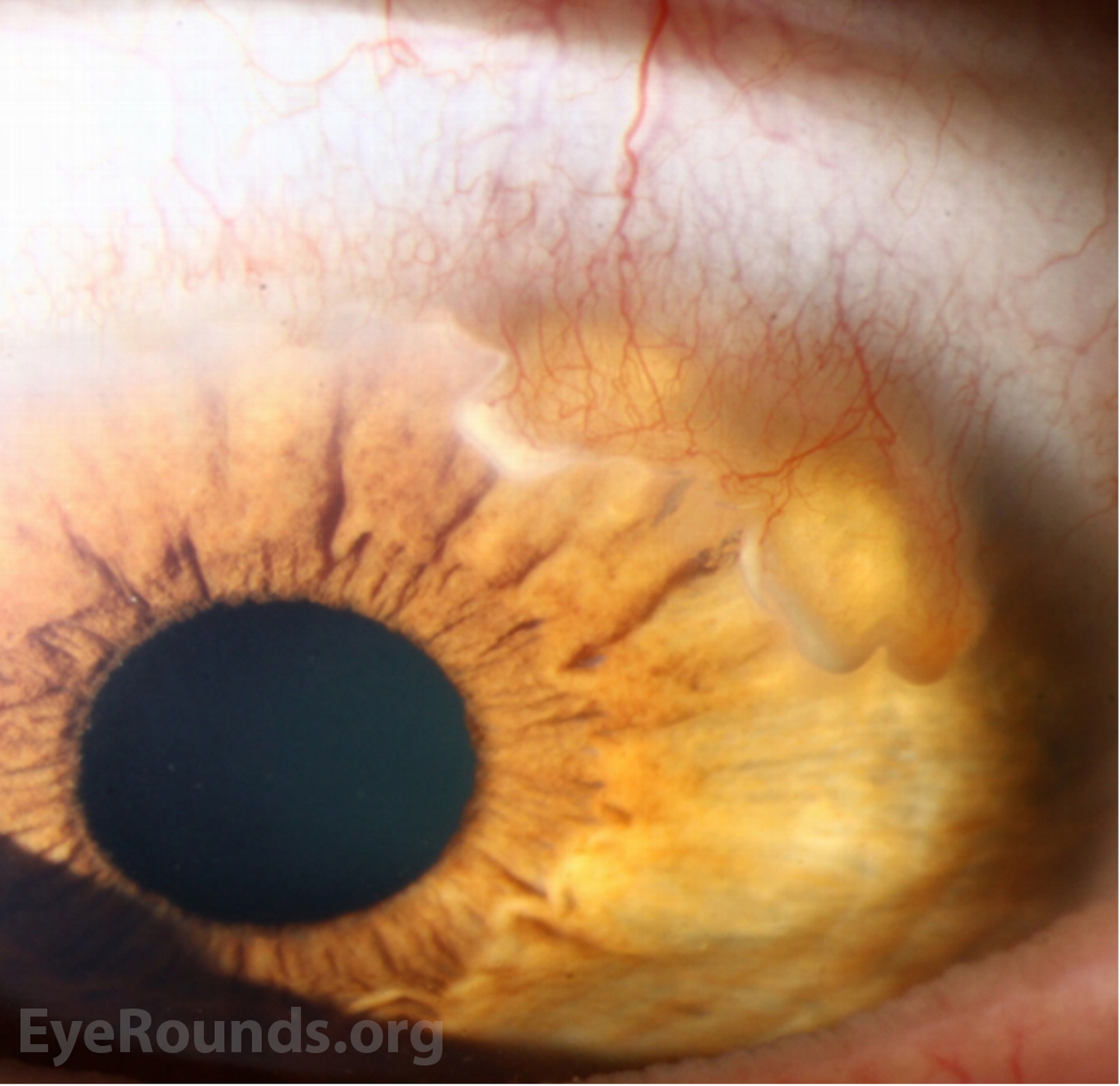
Terrien marginal degeneration is a rare disorder characterized by slowly progressive thinning of the peripheral cornea. This thinning most often begins superiorly, and patients may present with decreased vision due to worsening against-the-rule astigmatism. In severe cases, patients with Terrien marginal degeneration may present with corneal perforation following minimal trauma, or even spontaneously.
Etiology/Epidemiology
First described by Terrien in 1900, the condition is exceedingly rare, with no documented incidence or prevalence. While the disease is most commonly described in patients 20-40 years old, it may present at any age [1]. Men (54%) are typically affected more often than women (46%) [2].
Though the etiology is unknown, this disease is traditionally thought to be noninflammatory [1]. Some researchers have suggested that idiopathic tissue hypoxia may lead to fatty degeneration in the stromal lamella [3]. However, a subset of patients (typically men in their 20s-30s) who experience more symptomatic irritation seem to respond to topical steroids, suggesting the presence of a possible inflammatory variant. This is further supported by a study which described a subset of patients who experienced episodes of severe pain, episcleritis, or superficial scleritis [4].
Pathophysiology
While multiple hypotheses exist in the literature, Terrien marginal degeneration is most often thought to be a noninflammatory, degenerative condition in which thinning of the peripheral cornea spreads circumferentially [1]. This thinning results in a relative steepening of the perpendicular meridian, generating astigmatism. Given that this thinning and flattening most often occurs superiorly, this commonly induces against-the-rule astigmatism [5]. Thinning generally progresses slowly, but mean progression has been documented to be as high as 1.68 D of astigmatism over the 3 years following diagnosis [2]. As thinning progresses, it may ultimately result in corneal perforation, with an estimated perforation rate of 11.6 - 15% [2,4].
The most distinctive feature of Terrien marginal degeneration on light microscopy is a high number of intracellular and extracellular vacuoles [6]. On histopathologic examination the corneal epithelium may be normal, thickened, or thinned with pyknotic nuclei and dense cytoplasm. The basement membrane of the corneal epithelium is irregularly thickened, and Bowman’s layer is usually absent or fragmented. Descemet membrane may also be affected, with diffuse thinning and occasional fragmentation noted. The endothelium appears to be normal [1]. Analysis of the cornea with electron microscopy has further demonstrated phagocytosis of collagen fibrils, stromal ground substance, and lipids by highly lysosomal histiocytic cells [1,6].
Signs/Symptoms:
Initially, patients with Terrien marginal degeneration are asymptomatic or may report mild ocular irritation. Eventually, thinning-induced astigmatism may cause the patient to present with painless, progressive blurring of the vision. As in the above case, some patients with severe disease may present instead with perforation of the cornea following a mild trauma [1]. On exam, patients present with bilateral, small, yellowish-white stromal opacities which most often originate superior nasally and spread circumferentially. Terrien marginal degeneration may be differentiated from other causes of peripheral corneal thinning by a general lack of inflammation, the presence of superficial vascularization in a radial trajectory, a linear leading edge of lipid deposition, and a lack of epithelial defect [1,2]. In some circumstances, the patient may also present with a pseudo-pterygium with a flat, broad, leading edge of lipid originating in the oblique axis, which tends to manifest early in the course of disease [2].
Testing/Imagining/Laboratory work-up:
Terrien marginal degeneration is largely a clinical diagnosis. However, further testing with corneal topography may be helpful in quantifying the characteristic flattening, thinning, and steepening in the peripheral cornea [5]. Anterior segment optical coherence tomography (OCT), which provides a cross-sectional image of the cornea and pachymetry measurements, can depict morphological changes and help guide surgical treatment [7]. In vivo confocal microscopy may also provide important histological information [8]. Otherwise, no laboratory testing is necessary for diagnosis.
Treatment/Management/Guidelines:
Treatment of Terrien marginal degeneration is predominately guided by patient symptoms. At baseline, patients should be educated on important preventative measures given their heightened risk of corneal perforation. For instance, patients should be instructed to avoid rubbing their eyes. In those with higher risk of perforation, the use of protective eye wear is a cornerstone of management. For patients who experience visual disturbance secondary to high against-the-rule astigmatism, non-surgical management with spectacles, rigid gas permeable contact lenses, or scleral contact lenses is appropriate. In patients with vision-limiting astigmatism or those at risk for imminent perforation due to severe thinning, surgical management is indicated. This may include tectonic procedures such as conjunctival flaps or scleral grafting, which serve to prevent and repair perforation by restoring structural integrity of the eye. Vision-enhancing options may also be considered, with possible interventions including partial or total penetrating keratoplasty. In the most severe cases of 360° degeneration, annular lamellar keratoplasty graft may be required [1]. One case-study found that peripheral corneal cross-linking may provide a non-invasive approach to arresting progression of peripheral thinning in the disease [9].
EPIDEMIOLOGY & ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
References
Dangremond T, Hock LE, Shah TJ, Greiner MA. Terrien Marginal Degeneration. EyeRounds.org. July 12, 2022. Available from https://eyerounds.org/cases/329-terrien-marginal-degeneration.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links

{kind=link}
{kind=link}