
INITIAL PRESENTATION
Chief Complaint: Photophobia, blurred vision, and painful left eye
History of Present Illness:
A 30-year-old African American male presented with a one week history of redness, pain, and photophobia of his left eye (OS). He had had 3-4 similar episodes in the past year in only the left eye. He was seen by a local eye provider who diagnosed iridocyclitis and prescribed prednisolone 1% and cyclopentolate eye drops. At presentation, he was using prednisolone drops twice daily in his left eye.
During the episodes, he experienced visual “fogginess” and distortion. He denied systemic symptoms, including abdominal pain, diarrhea, hematochezia, dry eyes/mouth, photosensitivity, exertional chest pain, shortness of breath, swollen or painful joints, back pain, rash, or stiffness. He had discontinued contact lens use since his symptoms began. He had no history of recent travel, animal exposures, or personal or family history of autoimmune disease.
Past Ocular History: Recurrent iridocyclitis in the left eye only (3-4 total episodes over the last year)
Medical History: None
Medications:
Allergies: None
Family History: No family history of ocular or rheumatologic disease
Social History: 5 year history of few cigarettes a day (approximately 1 pack-year). No alcohol or drug use.
Review of Systems: Negative except for what is detailed in the history of present illness
OCULAR EXAMINATION
|
Right Eye |
Left Eye |
|
|
Lids/lashes |
Normal |
Normal |
|
Conjunctiva/sclera |
Clear and quiet |
2+ diffuse bulbar injection |
|
Cornea |
Clear |
Inferior stellate keratic precipitates, few clumps of endothelial pigment |
|
Anterior Chamber |
Deep & quiet |
3+ cell, 2+ flare, no hypopyon |
|
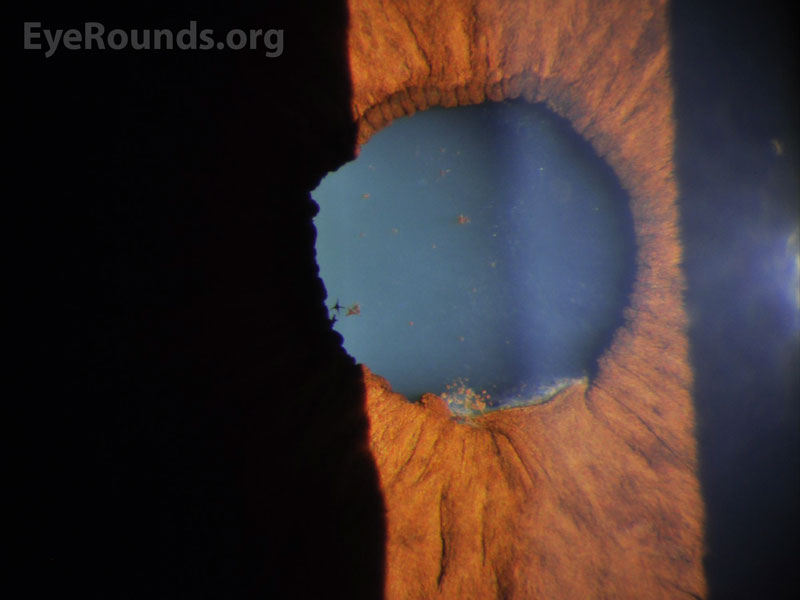
Iris |
Normal architecture; no nodules or transillumination defects (TIDs) |
Posterior synechiae at 6 o’clock, no nodules or TIDs (Figure 1) |
|
Lens |
Clear |
Trace nuclear sclerosis, superocentral pigment on anterior capsule |
Differential diagnosis:
General differential for nongranulomatous uveitis:
General differential for granulomatous uveitis:
CLINICAL COURSE
Due to recurrent episodes of anterior uveitis, laboratory workup was initiated.
|
ANA |
Positive at 1:1280, nuclear homogenous pattern |
|
ANCA |
Positive at 1:640 in cytoplasmic pattern (C-ANCA) |
|
HLA-B27 typing |
Positive |
|
Erythrocyte sedimentation rate (ESR) |
Negative |
|
C-Reactive Protein (CRP) |
Negative |
|
PR3 antibody |
Positive at 4.7 (normal 0-0.3) |
|
RNP antibody |
Positive at 7.5 (normal 0-0.9) |
|
UC-ANCA antibody |
Negative |
|
Lyme disease antibody (IgG/IgM) |
Negative |
|
MPO IgG |
Negative |
Further testing obtained included anti-Saccharomyces cerevisiae antibodies (ASCA) and a pelvic X-ray, which were both unremarkable. Physical examination by rheumatology was within normal limits. Several months later, the patient developed hematochezia, anemia, and acute unprovoked pulmonary embolism (PE). Colonoscopy revealed inflammation from the rectum to the cecum. Biopsies were consistent with a diagnosis of ulcerative colitis (UC). He was started on mesalamine with resolution of his hematochezia and completed a 6-month course of apixaban for PE prophylaxis.
His ocular manifestations throughout his course were limited to unilateral recurrent episodes of anterior uveitis. He was treated with prednisolone acetate 1% initially but required uptitration to difluprednate 0.05% during a flare that did not respond to prednisolone. He eventually developed elevated intraocular pressure in the treated eye, felt to be steroid-responsive ocular hypertension. This resolved when he was tapered off steroid drops and did not require further treatment.
DIAGNOSIS: Acute Anterior Uveitis Associated with HLA-B27 Positive Ulcerative Colitis
DISCUSSION
Etiology/Epidemiology
Recurrent inflammatory processes in the eye can be associated with systemic autoimmune or inflammatory syndromes. Uveitis is the most common form of intraocular inflammation, with up to 92% of uveitis being anterior uveitis, or inflammation of the iris and ciliary body [1]. HLA-B27-associated conditions are the most common underlying systemic diseases associated with anterior uveitis, representing up to 32% of acute anterior uveitis (AAU) cases [1,2]. These conditions include seronegative spondyloarthropathies, such as ankylosing spondylitis, reactive arthritis, psoriatic arthritis, and inflammatory bowel disease (IBD)-associated arthritis [3].
When a patient presents with uveitis, a thorough history and physical examination is warranted. A particular constellation of symptoms may suggest an underlying systemic illness and therefore may guide additional testing. IBD is a chronic, immune-mediated gastrointestinal disease that is divided into two major disorders: Ulcerative Colitis (UC) and Crohn’s disease (CD), with an annual incidence of 10.4 (UC) and 5.6 (CD) cases per 100,000 per year. Intestinal manifestations of IBD include inflammatory diarrhea, hematochezia, and abdominal pain. AAU is an extra-intestinal manifestation (EIM) of this systemic disease. In 10-20% of cases, EIMs represent the first sign of disease, as it was in the present case. Ocular complications of IBD occur in approximately 10% of cases [4].
HLA-B27 positivity in patients with IBD is associated with a higher incidence of ocular and other extra-intestinal involvement [4,5]. HLA-B27 prevalence varies among ethnic populations, with the highest positivity rates found among the Pawaia tribe of Papua New Guinea (53%). In the United States, roughly 7.5% of Caucasians are HLA-B27 positive, with about 2-4% African Americans having HLA-B27 positivity. Males are HLA-B27 positive 1.5-2.5 times more frequently than females [6].
Pathophysiology
The HLA-B27 genetic locus encodes the class I major histocompatibility complex (MHC) that enables antigen presenting cells (APCs) to present antigens to CD8+ T-cells and mount an immune response. Though the pathogenesis is poorly understood, some believe disease is caused by a dysfunctional immune response associated with recognition of the HLA-B27 epitope [7,8].
AAU is one of the most common extra-intestinal manifestations of IBD, but the connection between the two processes is not well understood. Gastroenterologists have begun to recognize multiple positive antibodies in patients with ulcerative colitis, with p-ANCA and ASCA being the best described. In IBD, it is hypothesized that regulatory B lymphocytes become dysfunctional, leading to changes in the population of memory B lymphocytes and plasmablasts with resultant hypergammaglobulinemia and presumably the formation of multiple autoantibodies [9]. The literature supporting this concept is small; descriptive as well as basic studies are needed. Specifically, antibodies to PR-3, although typically associated with granulomatosis with polyangiitis, have been recently described in people with UC, particularly with concurrent primary biliary cirrhosis and uveitis [10]. Therefore, it is important for non-gastroenterologists to recognize that multiple, seemingly unrelated auto-antibodies can suggest the diagnosis of ulcerative colitis.
Signs/Symptoms
The most common ocular manifestation of HLA-B27-associated disease is AAU. AAU typically presents as sudden onset ocular pain, redness, and photophobia. The typical age of presentation is in the second through fourth decades of life. It is generally recurrent, with 1-4 limited episodes occurring in a year. Signs of this condition are non-specific clinical signs of inflammation in the anterior segment, including anterior chamber cell and flare, keratic precipitates, synechiae, hypotony, and anterior vitreous cell. Severe inflammation can result in hypopyon and AC fibrin [11]. HLA-B27-associated uveitis usually follows a non-granulomatous pattern.
The classical clinical pattern of HLA-B27-associated AAU is severe, recurrent episodes of AAU that alternate between eyes or recur in the same eye but rarely involve both simultaneously [12]. Both persistent or chronic anterior uveitis and posterior segment involvement are uncommon in HLA-B27-associated AAU [13]. Inflammation in HLA-B27-associated AAU is typically non-granulomatous and can be severe enough to cause hypopyon or plasmoid aqueous. IOP is usually low during an acute attack due to decreased aqueous humor production secondary to ciliary body shutdown. However, secondary glaucoma due to mechanisms such as iris bombé, synechial angle closure, and steroid response can develop in the long term [14].
Testing/Laboratory work-up
Laboratory work-up should be guided by clinical suspicion based on the history and physical examination. Commonly obtained labs include inflammatory markers (ESR, CRP), HLA-B27 screening, and auto-antibody screening. Further imaging such as chest X-ray and a Ferguson view X-ray of the pelvis can also be obtained based on clinical suspicion for an underlying autoimmune disorder. In cases where there is a concern for inflammatory bowel disease, laboratory workup including perinuclear anti-neutrophil cytoplasm antibodies (p-ANCA) and ASCA can be obtained, and the patient may benefit from a referral to gastroenterology for further evaluation. In most cases of recurrent uveitis, it is important to rule out an underlying infectious etiology such as syphilis, sarcoidosis, and tuberculosis. Lastly, a referral to rheumatology can be considered to aid in co-management of these patients. See Table 2 below for a list of common rheumatologic diseases and their laboratory work up and history/exam.
The laboratory testing for this patient represents a unique and newly identified subset of UC-associated AAU. This patient tested negative for both p-ANCA and ASCA, which are typically associated with UC and Crohn’s disease, respectively. However, over the course of his disease, he developed auto-antibodies against various other self-antigens, including RNP and PR-3. Developing multiple, seemingly unrelated auto-antibodies is unusual, but has previously been reported in drug-induced autoimmunity (such as with hydralazine) and anecdotally in lymphomas [14].
|
Etiology |
Lab Testing |
History/Exam |
|
Spondyloarthropathies, Ankylosing spondylitis, Reactive Arthritis |
HLA-B27; Ferguson view X-ray of the pelvis |
Back pain and stiffness in the morning (>60 minutes) |
|
Juvenile Idiopathic Arthritis (JIA) |
ANA; Rheumatoid Factor and CCP antibodies typically negative |
Inflammatory arthritis in a young patient |
|
Behcet’s |
HLA-B51 |
Orogenital ulcerations |
|
Inflammatory Bowel Disease (Crohn’s Disease, Ulcerative Colitis) |
HLA-B27 |
Diarrhea with blood and mucous |
|
Sarcoidosis |
ACE, Chest X-ray, Chest CT, Non-caseating granulomas on tissue exam |
Lofgren’s syndrome (erythema nodosum, acute inflammatory arthritis, hilar adenopathy) |
|
Psoriasis |
Erythematous plaques with overlying scale |
|
|
Lupus |
ANA, antibodies to Smith (Sm), Ribonucleoprotein (RNP), Double-stranded DNA (DsDNA), SSA (Ro) and SSB (La) |
Arthritis, photosensitivity, oral ulcers |
|
Rheumatoid arthritis |
Rheumatoid Factor, CCP antibodies |
Joint swelling/pain; decreased joint range of motion |
|
TINU, Syphilis, Tuberculosis, HIV |
Syphilis antibodies, Quantiferon Gold, Urinalysis, Beta-2 microglobulin, HIV testing |
|
|
Celiac disease |
Antibodies to tissue transglutaminase and/or gliaden |
Diarrhea, malabsorption |
|
Sjogren’s syndrome |
ANA, antibodies to SSA (Ro), SSB (La), Salivary gland biopsy showing foci of lymphocytes |
Dry eyes/mouth |
Treatment/Management/Guidelines:
The mainstay of treatment for HLA-B27-associated AAU is topical corticosteroid drops titrated to the amount of ocular inflammation present. One common starting regimen is treatment with one drop of 1% prednisolone acetate every 1-2 hours while awake, which can be tapered over several weeks. Cycloplegia can be prescribed for comfort and to decrease the formation of posterior synechiae, with a typical regimen comprising one drop of cyclopentolate 1% twice daily in the affected eye. This regimen is sufficient for most cases but should be adjusted based on the patient’s disease course. Complex or recalcitrant cases may warrant referral to a uveitis specialist.
In the case of severe uveitis or posterior involvement, oral prednisone may be required. The initial dose can be as high as 1mg/kg and then is tapered over the course of several weeks. For patients with recalcitrant ocular inflammation or an inability to tolerate topical steroids, sub-Tenon’s triamcinolone or intravitreal steroids can be used instead. Patients with highly recurrent disease, vision-threatening flares, or underlying systemic disease often require systemic steroid-sparing immunosuppressive treatment. Inflammatory bowel disease may be initially treated with 5-aminosalicylic acid (5-ASA), sulfasalazine, or steroid-containing rectal preparations. Azathioprine, methotrexate, and TNF-alpha antagonists are also effective means of treating both HLA-B27-associated AAU and other systemic manifestations [14]. Other medications commonly used in the treatment of AAU are cyclosporine and mycophenolate mofetil. Adalimumab (Humira) is an FDA-approved therapy for intermediate, posterior, and panuveitis, and while not approved for use in AAU, it has proved effective [3,12]. All of the above immunosuppressive therapies are often prescribed and managed with the aid of a rheumatologist [3,12].
EPIDEMIOLOGY AND ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
References
Hendricks T, Obiano O, Warren A, Vogelgesang SA, Haugsdal JM. HLA-B27-associated Acute Anterior Uveitis. EyeRounds.org. September 27, 2022. Available from https://eyerounds.org/cases/334-HLA-B27-associated-Acute-Anterior-Uveitis.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links

{kind=link}