
Chief Complaint: Left upper and lower eyelid swelling
History of Present Illness: The patient is a 68-year-old male with a past medical history of type 2 diabetes who presented with a two-month history of left upper and lower lid swelling with intermittent redness, tearing, and “achy” pain. Additionally, he noted a mild difference in color vision between the right and left eyes. He denied diplopia or pain with eye movement. The right eye was unaffected.
He was initially seen by his general ophthalmologist who treated him with a course of oral antibiotics out of concern for preseptal cellulitis. After minimal improvement, he underwent a computed tomography (CT) scan which showed evidence of a pseudotumor (Figure 1). He was then treated with a course of oral prednisone which successfully reduced his eye pain but caused considerable rebound arthritis and affected his glycemic control.
After weaning off his steroids, he endorsed minimal pain but continued to have left side periocular swelling, ptosis, and a feeling of “pressure” intermittently. He was noted to have facial movement asymmetry at baseline. He denied recent traumas or thyroid abnormalities.
Past Ocular History:
Past Medical History:
Ocular Medications: None
Family History:
Social History:
Allergies: No known allergies to medications
Review of Systems: Negative except what is detailed in the history of present illness
OCULAR EXAMINATION
LABORATORY TESTING
| Laboratory Test | Patient Result | Reference Range |
|---|---|---|
| CBC w/diff | Normal | n/a |
| Creatinine | 0.9 | 0.6-1.2 mg/dL |
| EGFR (calculated) | 84 | >60 mL/min/1.73m2 |
| Thyroid-stimulating hormone (TSH) | 4.71 | 0.27-4.68 uIU/mL |
| Free T4 | 0.96 | 0.85-1.76 ng/dL |
| Thyroid-stimulating immunoglobulin (TSI) | 107 | ≤122% |
IMAGING
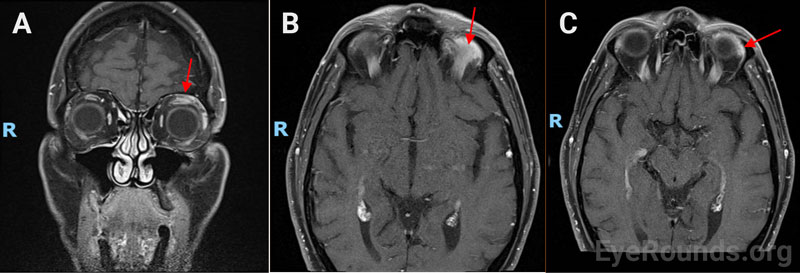
CT imaging was obtained at outside hospital before patient started treatment with prednisone. CT showed nonspecific enhancement and enlargement of the left superotemporal region of the orbit.
When patient first presented to our clinic, initial orbital ultrasound showed the left superior rectus inserting tendon and anterior portion of the muscle to be thicker and less reflective than the right superior rectus. Maximum thickness of the right and left superior recti insertion were 1.7mm and 4.2 mm respectively. All other extraocular muscles appeared symmetric and within the normal range of thickness and reflectivity. No other mass lesion was detected. Magnetic resonance imaging (MRI) demonstrated nonspecific enlargement of the left superior rectus, levator palpebrae superioris, and lacrimal gland (Figure 1).
Differential Diagnosis
CLINICAL COURSE
Given the patient’s findings on imaging and significant reduction of pain with steroid treatment, his clinical picture was most consistent with idiopathic orbital inflammation (IOI). He elected for observation rather than repeating another course of prednisone due to previous negative side effects. He returned for follow up after 3 months and noted his swelling had completely resolved. Given patient had complete resolution of his symptoms, biopsy and further workup were deferred. He denied pain or discomfort and was recommended to have routine follow up with his primary ophthalmologist.
DIAGNOSIS: Idiopathic orbital inflammation (IOI) Syndrome
DISCUSSION
Epidemiology/Etiology
Orbital inflammation refers to a broad group of conditions. Due to the heterogeneity in which orbital inflammation presents, it is often categorized by the anatomic site where the inflammation occurs and by the source of the inflammation.[1] Common causes of orbital inflammation include Graves’ ophthalmopathy (accounts for 60% of orbital inflammation cases in ages 21-60) and other systemic disease such as sarcoidosis, granulomatosis polyangiitis and IgG4 related disease.[1,2] When there is no identifiable local or systemic cause for orbital inflammation, it can be classified as idiopathic orbital inflammation syndrome (IOI) syndrome.[1]
IOI was initially characterized in 1905 by Birch-Hirschfeld as “orbital pseudotumor”, an inflammatory disease mimicking a neoplasm.[3,4] IOIS has been described by other terms, including non-specific orbital inflammation, nonspecific orbital granuloma, and idiopathic inflammatory orbital pseudotumor, and many others.[5,6] It is the third most common orbital disease, with nearly 10% of orbital disease attributable to IOIS.[7] However, as more etiologies for orbital inflammation are investigated, the number of IOIS cases are decreasing. In a recent retrospective review of 45 patients given a diagnosis of IOIS, additional immunohistochemical staining was performed on their biopsy, and 46.7% of patients were found to meet criteria for IgG4-related disease (official criterion established in 2014).[8]
While no singular etiology has been established, IOI is thought to be autoimmune in origin, triggered by environmental or genetic factors. IOI is a diagnosis of exclusion and is difficult to diagnose without additional workup.[7,9] Previously, a positive response to corticosteroid treatment in patients suspected to have IOIS due to a negative workup was enough for a diagnosis.10 This criterion for diagnosis is no longer sufficient as not all forms of IOIS respond to corticosteroids, and an orbital biopsy is necessary to confirm a suspected diagnosis. However, often times, physicians will defer a biopsy given its invasive nature and treat suspected IOIS without confirmation.[7,10]
Given its history as a largely descriptive term, IOIS is very heterogeneous and thus a unifying classification scheme has not been adopted. Blodi and Gass found 9 histological subtypes based on 140 orbital biopsies, citing formation of lymph follicles, diffuse lymphocytic infiltration, and lymphoid hyperplasia as the most common types.[11] Yuen and Rubin, in a retrospective, single-center review, found five subtypes based on anatomic involvement, including dacryoadenitis, myositis, the orbital apex, and elsewhere in the orbit.[12] In general, IOI can be grouped based on many factors, most commonly anatomic location or histopathology (Table 1).[5,7,9]
| Site of involvement: | Yuen and Rubin[12] | Swamy et al.[9] | Eshraghi et al.[7] | Young et al.[10] |
|---|---|---|---|---|
| Lacrimal gland | 21% | 54% | 38% | 32.9% |
| Extraocular muscle | 19% | 50% | 11% | 5.7% |
| Optic nerve | - | 21% | 2.6% | - |
| Orbital apex | 6% | - | 1.3% | - |
Table 1: Common sites of involvement of idiopathic orbital inflammation among four single-center, retrospective reviews.[7,9,10,12]
Pathophysiology:
While a clear pathophysiological pathway for IOI has yet to be defined, there is evidence that certain cytokines are upregulated in IOIS patients. When comparing orbital biopsy samples of patients with IOIS to control, Wladis et al. found interleukin-2, interleukin-8, interleukin-10, interleukin-12, gamma interferon, and tumor necrosis factor-α were significantly elevated, with gamma interferon and interleukin-12 found at concentrations 10 times higher in the IOI group compared to healthy controls.[13] Further work on the molecular biological basis of IOI is needed to elucidate potential targets for future treatments.[13]
Signs/Symptoms:
Symptoms of IOI vary, although most cases are unilateral, and a common site of involvement is the lacrimal gland.[7,12] Symptom onset can be acute, subacute, or chronic. The most common symptoms include periorbital pain and diplopia. Common signs include ptosis, periorbital edema, extraocular muscle limitation, red eye, proptosis, and chemosis. Rarely, optic neuropathy may occur.[7,10,14]
Testing/Laboratory workup:
As IOI is a diagnosis of exclusion, by definition, a systemic evaluation should be undertaken. However, there is no generally agreed-upon workup. A consensus panel was convened in 2017 to determine clinical, radiologic and histopathologic criteria in the diagnosis of IOIS, and is listed in Table 2.[15] Broadly, IOIS can be divided into two types myositic (involving one or more extraocular muscles) or nonmyositic (involving other structures such as the lacrimal gland or orbital fat). In general, workup should be tailored based on patient-specific risk factors and is at the discretion of the clinician.[15]
| Nonmyositic idiopathic orbital inflammation | Myositic idiopathic orbital inflammation |
|---|---|
Clinical/radiologic criteria:
|
Clinical/radiologic criteria:
|
Table 2: Consensus diagnostic criteria of idiopathic orbital inflammation listed from highest to lowest percent consensus. Bold indicates ≥70% mean rank, or higher percent consensus. Adapted from Mombaerts et al.[15]
Radiologic imaging is frequently obtained, and may help identify the extent of inflammatory spread.[12] In general, MRI is preferred over CT due to better soft tissue resolution. CT can show enlargement of extraocular muscles or hyperintensity suggesting inflammation of surrounding structures within the orbit. Features of orbital inflammation on MRI include a hypointense infiltrative mass on T2 with contrast enhancement and without diffusion restriction. A homogenously enhancing pattern may favor IOIS over tumor or infection, as the latter lesions are expected to be more necrotic and thus heterogenous. Ultrasound (B-scan) may also be obtained but has limited utility in evaluation of deep orbital tissues.[16]
Myositic inflammation generally responds well to corticosteroid treatment, thus further diagnostic workup may not be needed if the patient is responsive to a corticosteroid trial. In contrast, nonmyositic inflammation typically does not respond to corticosteroids, and diagnosis of nonmyositic orbital inflammation tends to require a tissue biopsy.
The role of biopsy in diagnosis of IOI is controversial. Some argue against biopsy as corticosteroid therapy is thought to be necessary regardless of histopathological findings;[7] others argue a biopsy is indicated unless specifically contraindicated.[10] Generally, in addition to cases of nonmyositic orbital inflammation, biopsy should also be considered if steroid therapy fail to resolve the condition; or if there is disease recurrence and no biopsy has been obtained previously. [7,10]
| Treatment options for IOI | |
|---|---|
| Corticosteroids |
|
| Steroid-sparing agents/immunomodulators |
|
| Biologic agents |
|
Table 3: Summary of most frequently used treatment options for IOI. Adapted from Carruth and Wladis [14].
Corticosteroids
Corticosteroids are generally considered first-line treatment. These can be administered orally, topically, or as an intraorbital injection. Oral steroids (prednisone) are delivered with a starting dose of 1 mg/kd/day for 2 to 4 months with a slow taper.[7,17] Pulsed intravenous methylprednisolone has been administered for fast symptom relief or in more severe cases of IOI, for acute symptom management.[5] While corticosteroids are the treatment of choice due to their low cost and easy administration, the recurrence rate is relatively high (31.4-52%) and not all forms of IOI respond well to corticosteroids.[10,17] Furthermore, long term oral corticosteroid use has various negative side effects, including adrenal insufficiency, osteoporosis, weight gain, diabetes, cataracts, gastrointestinal disorders, and hypertension.[17] Steroid injections of suspensions such as triamcinolone pose a risk of vascular occlusion.[18]
Biologic agents
Although the exact pathophysiology of IOIS is unknown, certain biologic therapies have been found to be effective. The most studied of these biologic agents is infliximab, a monoclonal IgG1k antibody and TNF-α (alpha) inhibitor. Several studies have demonstrated that the use of infliximab can reduce symptom burden and steroid dependence in IOIS patients. Infliximab is administered intravenously at 3-5 mg/k at week 0, 2, and 6 and every 4-8 weeks following. Despite its efficacy, infliximab is generally reserved for steroid-refractive cases or in cases where methotrexate has failed, as cost can be prohibitive. Adalimumab, another TNF-α inhibitor, has been used in two reported cases of IOI where it reduced swelling. Other biologic agents of interest such as etanercept, daclizumab, abatacept, and tocilizumab, have yet to be studied thoroughly.[14] Tocilizumab is being discussed as a treatment for IOI, as it has shown favorable results in several case reports of patients with refractory disease.[19,20]
Other therapy
Other treatment options for IOIS include radiotherapy and surgery. Surgery for IOIS management is only indicated in certain cases where there is a focal mass or fibrosing mass that could be debulked.[7] Radiotherapy is rarely administered on its own as a first line of defense. However, in cases of IOI with inadequate or no response to corticosteroids, use of radiotherapy has resulted in improved ocular motility, reduced inflammation, and increased visual acuity.[14,21]
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
Mani S, Ramirez DA, Vogelgesang SA, Shriver EM. Idiopathic Orbital Inflammation. EyeRounds.org. Posted July 10, 2023; Available from https://EyeRounds.org/cases/337-idiopathic-orbital-inflammation.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links

{kind=link}