
Chief Complaint: Hazy vision in the right eye following cataract surgery
History of Present Illness
A 72-year-old woman presents one month after cataract extraction (CE) with primary reverse optic capture (ROC) of the right eye (OD).
Her history is significant for significant negative dysphotopsia following cataract surgery in the left eye (OS). In the OS, she had a perfectly centered 3-piece TECNIS intraocular lens (IOL) placed in the capsular bag. This position (well-centered and in-the-bag) is the classic lens position described in the literature in which negative dysphotopsia occurs [1]. She had immediate resolution of her symptoms OS with a subsequent operation to place the optic anterior to the anterior capsule known as reverse optic capture (ROC) as described by Fram and Masket [2].
About a year later, she presented with cataract in the right eye (OD). Due to the history of negative dysphotopsia in her first eye resolved by ROC, primary ROC was performed in the OD with a near goal of –1.50 diopters.
She now presents one month after cataract extraction (CE) with primary reverse optic capture (ROC) of the right eye (OD). She is dissatisfied with her visual outcome and complains of “hazy vision.”
Past Ocular History
Past Medical History
Medications
Allergies
Family History: Non-contributory
Social History: Non-contributory
Review of Systems: Negative except for what is detailed in the history of present illness
OCULAR EXAMINATION
Differential Diagnosis
CLINICAL COURSE
The presence of fluid posterior to the IOL on examination was consistent with a diagnosis of early post-operative capsular block causing a myopic shift. The patient underwent a small Nd:YAG laser posterior capsulotomy (4 applications at 2.0mJ using Abraham YAG lens) to relieve capsular distension. A small amount of fluid was noted to extravasate posteriorly during the procedure. She returned to clinic two weeks later still with concerns of blurry vision. On examination, her vision was 20/40-2 without correction. The capsular distension had improved, and she refracted to 20/20. It was thought that she may need additional treatment with Nd:YAG laser but the decision was made to wait for the IOL to properly seat. She returned to clinic three months later still with concerns for blurriness in the temporal field of the OD. Her myopic shift had improved to -2.25 sphere (original goal –1.50), but she was able to tolerate the monovision and did not want glasses for distance vision. It was thought that her temporal blurriness may be due to temporal phimosis and additional YAG was deferred further. She returned six months later with stable vision and similar concerns for blurred vision temporally. This blurriness was present only upon waking in the morning and resolved after 30 minutes, so the patient elected to observe this rather than pursue additional treatment.
DIAGNOSIS: Early post-operative capsular block causing myopic shift
DISCUSSION
Etiology/Epidemiology
Capsular block syndrome (CBS) is caused by a blockage in the opening of the anterior capsule leading to fluid accumulation behind the intraocular lens (IOL) and subsequent distension of the capsular bag [3,4]. It is a rare but important complication of cataract surgery and has been reported in 0.73-1.0% of cases [5]. As in this case, the accumulation of fluid can lead to anterior displacement of the IOL. This anterior displacement shifts the optical zone forward leading to myopic shift. Increased intraocular pressure is another potential sequalae of this condition [3]. Clinically, this leads to significant post-operative myopic surprise. Sorenson and colleagues reported an average of -1.77 D of myopic surprise with a highest reported surprise of -3.92 D [6].
Risk Factors
In their systematic review, Kanclerz and Wang identified male sex, younger age, and the presence of subcapsular and mature cataracts as risk factors for developing CBS. They speculated that these differences may be due to larger capsular bags in these patients [5]. However, others have found there to be no significant difference in age, gender, or type of ophthalmic viscosurgical device (OVD) used. Axial length greater than 25.0 mm has been associated with a significantly greater risk of CBS [3]. Other risk factors include softer IOL haptics, larger haptic surface, biconvex design, and improper angulation. However, there is no evidence that any one IOL design has a significantly higher risk of CBS [5].
Classification and Management of Capsular Block Syndrome
Most often, CBS is classified according to the scheme presented by Miyake and colleagues. In this classification, CBS is divided into intraoperative CBS, early postoperative CBS, and late postoperative CBS:
While the Miyake classification is conventionally used to classify CBS, alternative classifications have also been proposed. Kim and Shin suggested a classification based on pathophysiology, separating CBS into categories of noncellular, inflammatory, and fibrotic. Noncellular CBS describes the accumulation of clear fluid within one day of surgery that leads to anterior displacement of the IOL. Inflammatory CBS presents several days after surgery with an exudative inflammatory reaction around the pupil and can be treated with topical steroids. Lastly, fibrotic CBS describes late postoperative fibrosis of the capsulorhexis opening and accompanying posterior capsule opacity [3].
Differential Diagnosis of Induced Myopia After Cataract Surgery
While the patient in this case had early postoperative CBS, several other etiologies should be considered in the differential diagnosis for a myopic surprise after cataract surgery. The underlying principle of each of these etiologies is the implantation of an incorrectly powered IOL or the unintentional anterior displacement of the IOL leading to an induced myopia.
One possible cause is the incorrect calculation of IOL power. This is most commonly due to error or inconsistency in predicting the postoperative position of the IOL. An analysis by Norrby found that errors in predicting postoperative IOL position, post-operative refraction, and imprecise axial eye length measurements account for 80% of IOL power calculation errors. Imprecise keratometry data also have been shown to contribute to the incorrect calculation of IOL power [9].
Additionally, inadvertent implantation of the wrong IOL can lead to a myopic surprise postoperatively. Due to the large number of different IOL types and powers, cataract surgery carries a greater risk of implanting the wrong device than any other procedure. The true incidence of this error is not known, however most cases (90.4.% in one study) are not recognized until after surgery when the patient presents with a refractive surprise [10]. Given that wrong IOL implantation is the most common preventable error in ophthalmic surgery, verification of the IOL during the operative site “time out” is now a required practice at institutions such as the Iowa City VA (http://www.EyeRounds.org/cases/72-IntraocularLensTimeOutSystemsBased.htm.). Analysis of wrong IOL implantations in the United Kingdom found human factors to be the main cause including misfiling data in the wrong patient file, selecting the IOL based on data from the wrong eye, and changing list order or operating room personnel [10,11].
Another possible cause of a myopic surprise after cataract surgery is the implantation of an upside down three-piece IOL. Normally, the haptics of a three-piece IOL are angled anteriorly with the optic slightly posterior to them. However, the upside-down implantation of a three-piece IOL leads to the posterior angulation of the haptics with the optic lying in a more anterior position than is intended (Figure 2). The incorrect anterior position of the lens leads to light focusing in front of the retina and a resulting myopic surprise. However, some have raised questions regarding the impact of this error. In a small case series of six patients, Halpern and Gallagher found that only two patients who had undergone upside-down three-piece IOL implantation had a refractive surprise greater than 0.15 D. Thus, they concluded that more research is needed regarding the refractive outcomes in patients with upside-down three-piece IOL implantation [13].
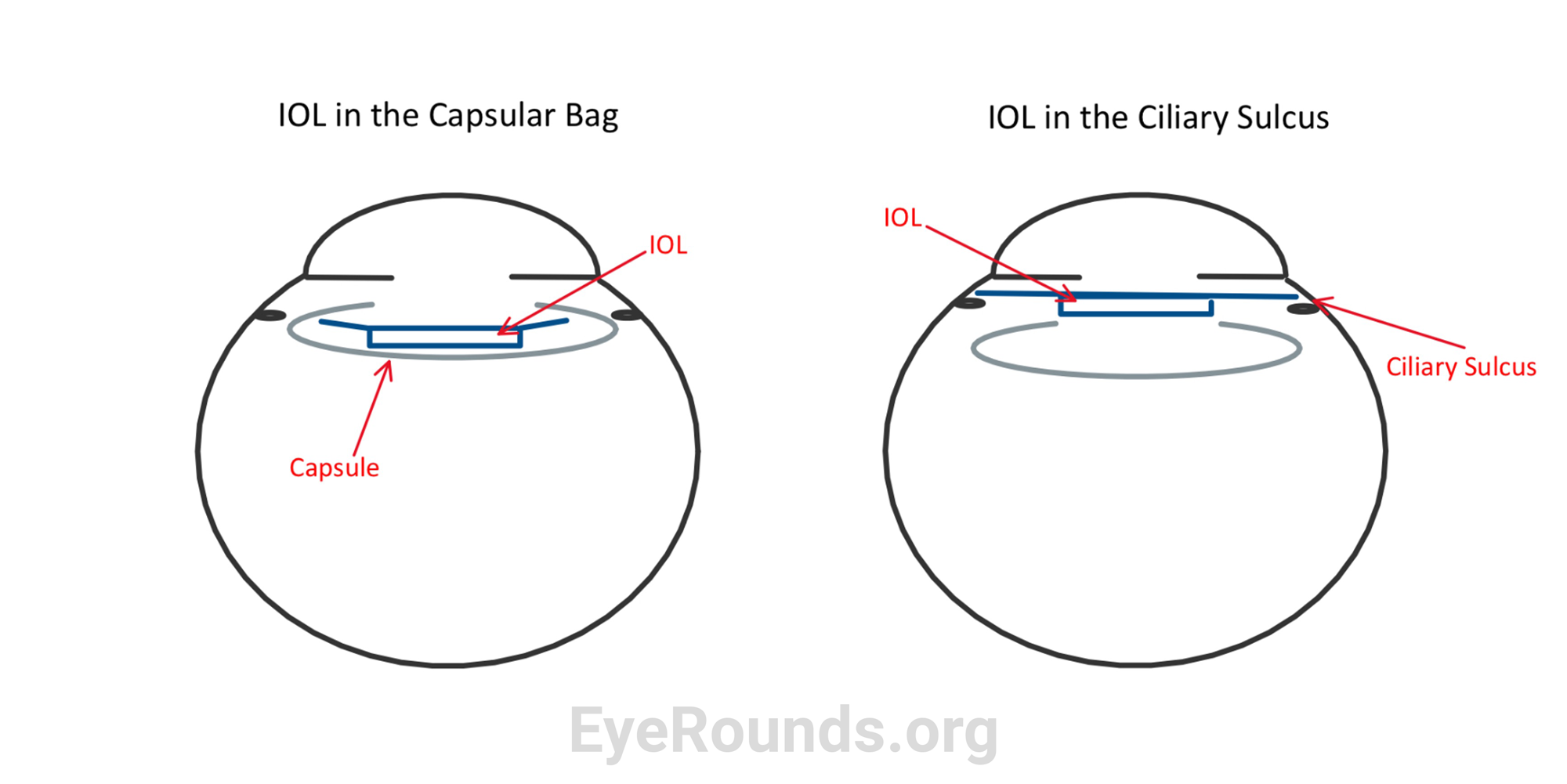
Lastly, incorrect implantation of the IOL into the ciliary sulcus can cause a myopic surprise following cataract surgery. Implantation of the IOL into the ciliary sulcus is sometimes done intentionally for eyes where implantation into the standard location in the capsule is not possible. This includes cases of zonular laxity, capsular contraction, or posterior capsule rupture [14,15]. However, unplanned implantation into the ciliary sulcus can lead to an IOL position that is too far anterior compared to what was planned preoperatively (Figure 3). This also leads to the focusing of light in front of the retina and leads to a myopic surprise. There are also other possible complications of placement of a single-piece IOL into the ciliary sulcus including chafing of the iris, recurrent iridocyclitis, and uveitis-glaucoma-hyphema syndrome [14,15].
EPIDEMIOLOGY OR ETIOLOGY
|
CLASSIFICATION [4]
|
TREATMENT/MANAGEMENT [4]
|
DIFFERENTIAL DIAGNOSIS OF MYOPIC SURPRISE
|
Kuziel JD, Hendricks TM, Oetting TA. Capsular Block Syndrome: A Discussion of Induced Myopia After Cataract Surgery. EyeRounds.org. Posted August 18, 2023; Available from https://EyeRounds.org/cases/347-capsular-block-syndrome.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links



{kind=link}