INITIAL PRESENTATION
Chief Complaint: Redness, pain, and loss of vision in the left eye
History of Present Illness:
An 89-year-old gentleman was referred to the University of Iowa Health Care Medical Center Eye Clinic by an outside hospital. He originally presented to his local hospital three days prior with the chief complaint of a red, painful eye and was diagnosed with endogenous endophthalmitis. He was hospitalized, however, due to atrial fibrillation and pneumonia diagnosed at the same visit. There, he received an intravitreal tap of vancomycin and ceftazidime. He was started at the time on topical tobramycin and vancomycin every 2 hours and continued until presentation. On presentation to our clinic, the patient continued to endorse redness and “7 out of 10” pain.
Past Ocular History:
Past Medical History:
Medications:
Allergies:
Family History:
Social History:
Review of Systems:
OCULAR EXAMINATION
DIFFERENTIAL DIAGNOSIS:
CLINICAL COURSE
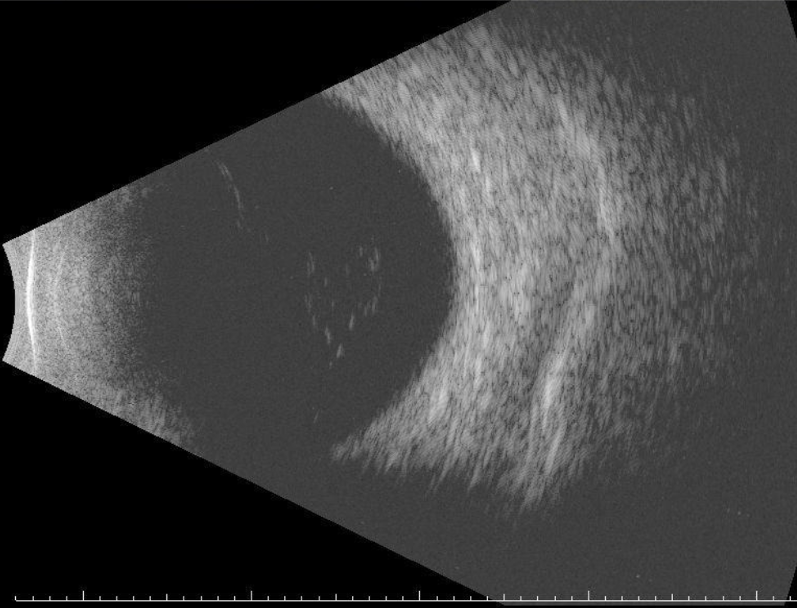
The patient was instructed to cease contact lens use at the outside hospital; this was reiterated at our initial evaluation. His history without recent trauma or procedure, coupled with unremarkable findings of ocular ultrasound and no growth on vitreous culture from outside hospital made our suspicion with endophthalmitis lower; attention was directed towards the keratitis. Corneal scrapings for culture (aerobic, anaerobic, fungal, viral, gram stain, mycobacteria and acanthamoeba) were collected, and the patient was started on topical tobramycin and vancomycin hourly while awake as well as every two hours at night. Cultures returned positive for Staphylococcus mitis and S. epidermidis with no evidence of amoebic infection.
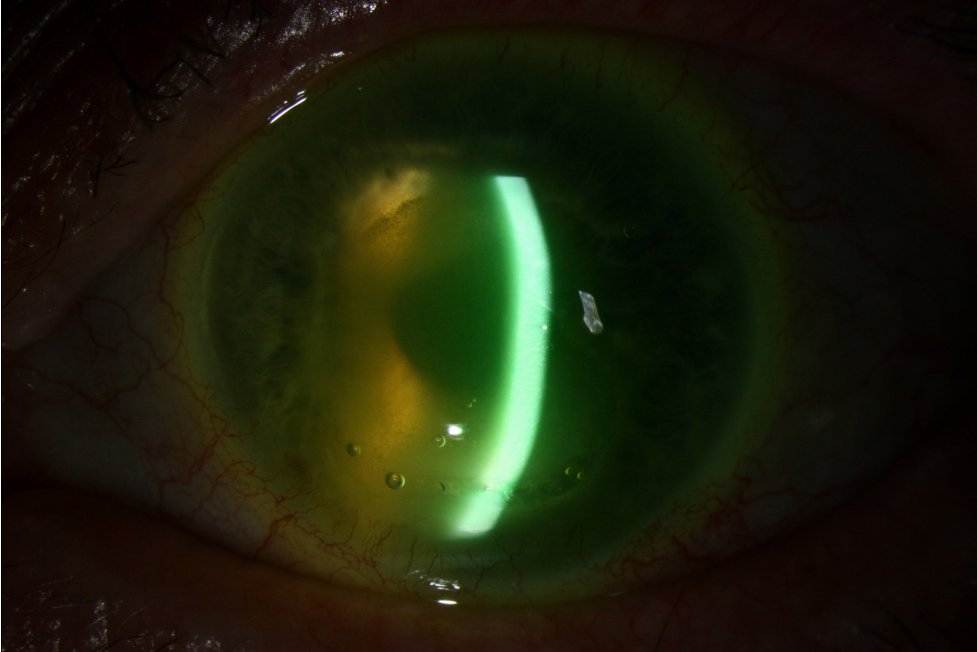
He was carefully followed with weekly visits. Three weeks after initial presentation his visual acuity improved to counting fingers at 1 foot. At this visit, the peripheral cornea was clearing while a geographic ulcer with ring infiltrates and inferior keratolysis remained (Figure 1, slit lamp photograph). Erythromycin ointment, oral doxycycline, and a bandage contact lens were added to assist in corneal healing.
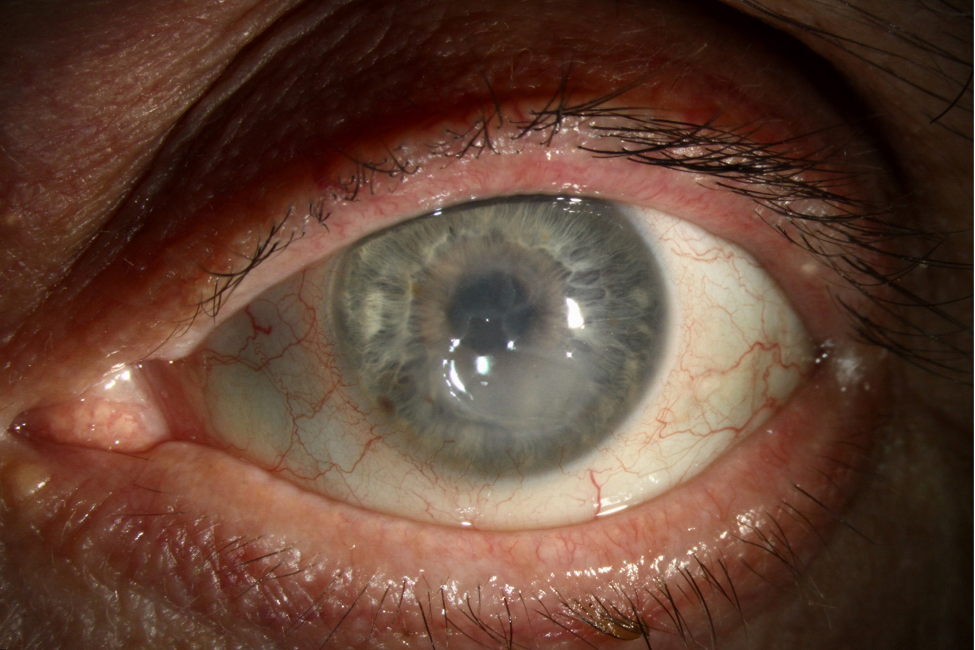
Two months after the initial presentation, the visual acuity in the left eye was 20/800 with correction. Slit lamp examination showed a nonhealing geographic epithelial defect (Figures 2 and 3, slit lamp photograph). Given that the presentation was of a non-healing ulcer with persistent epithelial defect and keratolysis while on topical antibiotics, there was suspicion for a more atypical microbe as the etiology behind his condition, such as a fungal or amoebic infection. Therefore, repeat corneal scraping for cultures were collected. Cultures were positive for the budding yeast Exophiala. Management was changed to topical amphotericin B hourly, with concurrent trimethoprim/polymyxin B (Polytrim) to cover the bacterial components of the infection identified on the first set of cultures. Further, the benzalkonium chloride preservative in Polytrim potentiates the effect of amphotericin B. Due to the patient’s comorbid cirrhosis as well as financial difficulties, oral antifungals were held. One week later, visual acuity was 20/250 with correction; on exam, the pigmented ring infiltrate had resolved, and the epithelial defect was 2 x 4 mm.
Four months after initial presentation, the epithelial defect had resolved, and anterior scarring and neovascularization were visible (Figure 3). The patient then chose to transfer care locally.
DIAGNOSIS: Fungal keratitis, Exophiala species
DISCUSSION
Etiology/Epidemiology:
Exophiala is a dematiaceous (brown-pigmented) yeast that is a rare cause of human disease. It most commonly infects skin and soft tissues, but has also been reported in cases of pneumonia, sinusitis, and endocarditis(1 ,2). Ophthalmic manifestations include endophthalmitis(3) and keratitis(4). Recent ocular surgery is a risk factor, with cases of Exophiala keratitis reported after laser-assisted in situ keratomileusis (LASIK), penetrating keratoplasty (PKP), Descemet membrane endothelial keratoplasty (DMEK), and cataract extraction and intraocular lens placement (5). Immunodeficient status, contact lens wear, topical steroid use, ocular trauma with vegetable matter, and chronic keratitis are other risk factors for Exophilia keratitis in particular and fungal keratitis in general (6). Interestingly, the most common sources of exposure in a household environment are dishwashers and restrooms (7).
Signs and Symptoms:
Patients most often present with blurry vision, pain, discharge, and redness, similar to our case. Like other yeasts, physical exam findings of Exophiala keratitis include a plaque-like central corneal ulcer with associated hypopyon and conjunctival injection.
Ring infiltrate is a circumferential stromal infiltrate that is sensitive, but not specific, for fungal keratitis because it is due to both infectious and non-infectious etiologies. It is most commonly associated with amoebic keratitis(8), so confirmation with culture and a low index of suspicion for an alternative etiology (for example, an inflammatory response such as a Wessley immune ring) is crucial (9).
Testing/Laboratory work-up:
Given the different treatment guidelines for amoebic versus fungal keratitis in the setting of a similar clinical presentation, laboratory workup is crucial. Exophiala has been cultured on blood, chocolate, and Sabouraud agar. Confocal microscopy of corneal scrapings reveals budding yeast forms and thin, filamentous structures, as published by Aggarwal and colleagues (4). Species identification can be identified on mass spectrometry(10). Antifungal susceptibility testing can be used to guide management (discussed below).
Based on clinical judgement, consider optical coherence tomography, ophthalmic ultrasound, or a computed tomography (CT) of the orbits to identify concurrent endophthalmitis, uveitis, retinitis, or orbital cellulitis.
Detailed, clear documentation of exam findings is crucial to allow serial measurements of ulcer characteristics. This flags clinicians to cases that do not follow an expected time course, such as this patient’s case, and initiates repeat testing. In our case, thorough documentation of ulcer characteristics over time drew attention towards persistent non-healing and thus initiated a repeat corneal culture, identifying Exophiala.
Treatment/Management/Guidelines:
Options for medical management include topical and oral antifungals; subconjunctival or intracameral antifungal injections have also been used(11). Geographic location and climate were historically used as predictors of the most likely causative organism in fungal keratitis; today, broad-spectrum antifungal treatment is started as soon as a mycotic origin is suspected (6). This is especially important given some fungi, including Exophiala species, may take up to two weeks to culture in a clinical laboratory(2). Options include topical natamycin, amphotericin B, and voriconazole among other azole agents. An in vitro susceptibility study found that Exophiala isolates were most susceptible to posaconazole, itraconazole, and micafungin (12), yet none of these are currently available as ophthalmic drops in the United States. In our case, the patient responded to topical amphotericin B. When identified, topical steroids should be discontinued because the anti-inflammatory effect allows for persistent fungal growth.
If the ulcer reaches sterility but results in corneal scarring in the visual axis, a penetrating keratoplasty (PKP) can be used to rehabilitate vision while a therapeutic PKP may also be pursued for non-resolving infections.
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
Al-Kaylani HM, McCarthy S, Garza Reyes A, Matharu KS, Kang T, Goins KM. Fungal Keratitis, Exophiala species. EyeRounds.org. February 23, 2026. Available from https://EyeRounds.org/cases/370-exophiala-keratitis.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links