INITIAL PRESENTATION
Chief Complaint: Ache in the left eye
History of Present Illness:
An 86-year-old male presented to clinic with one week of pain in the left eye. The pain was described as a constant, aching, pressure-like sensation that radiated posteriorly and was rated 4/10. Pain worsened with eye movement, especially with left or right gaze. He tried acetaminophen and antihistamine drops, which did not help. He reported closing his eyes alleviated some of the pain temporarily. He also experienced a foreign body sensation, redness, and tearing of the left eye. Notably, he had a history of trauma to the left eye, leaving him no-light-perception (NLP) over 60 years ago. His right eye remained asymptomatic. He denied chills, malaise, new aches, or fatigue.
Past Ocular History:
Past Medical History:
Medications:
Allergies:
Family History:
Social History:
Review of Systems:
OCULAR EXAMINATION
DIFFERENTIAL DIAGNOSIS:
CLINICAL COURSE
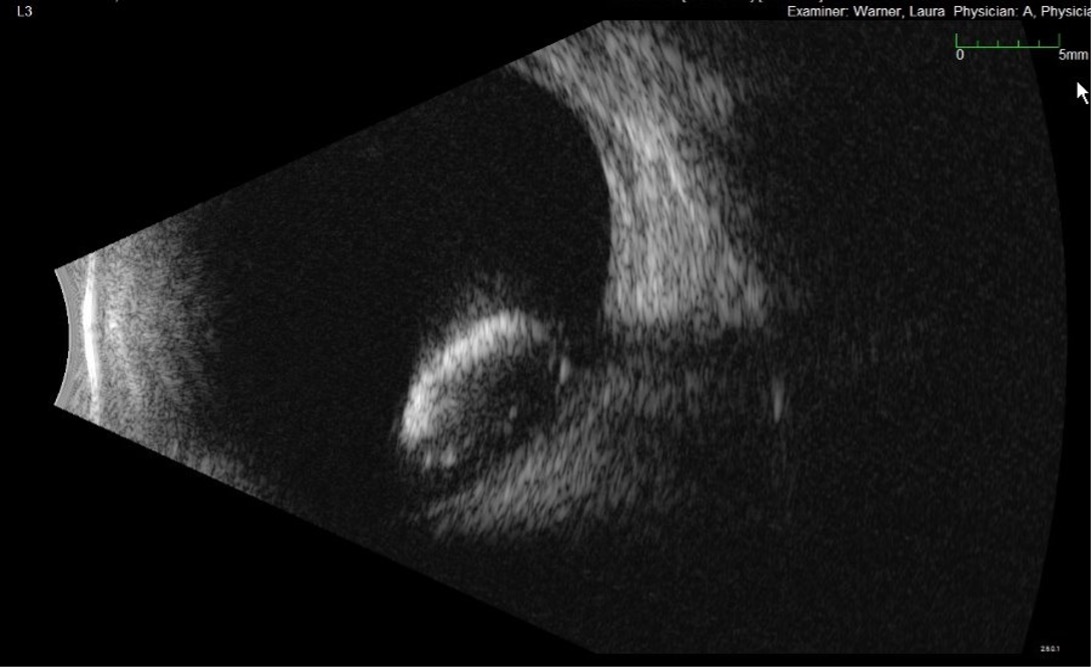
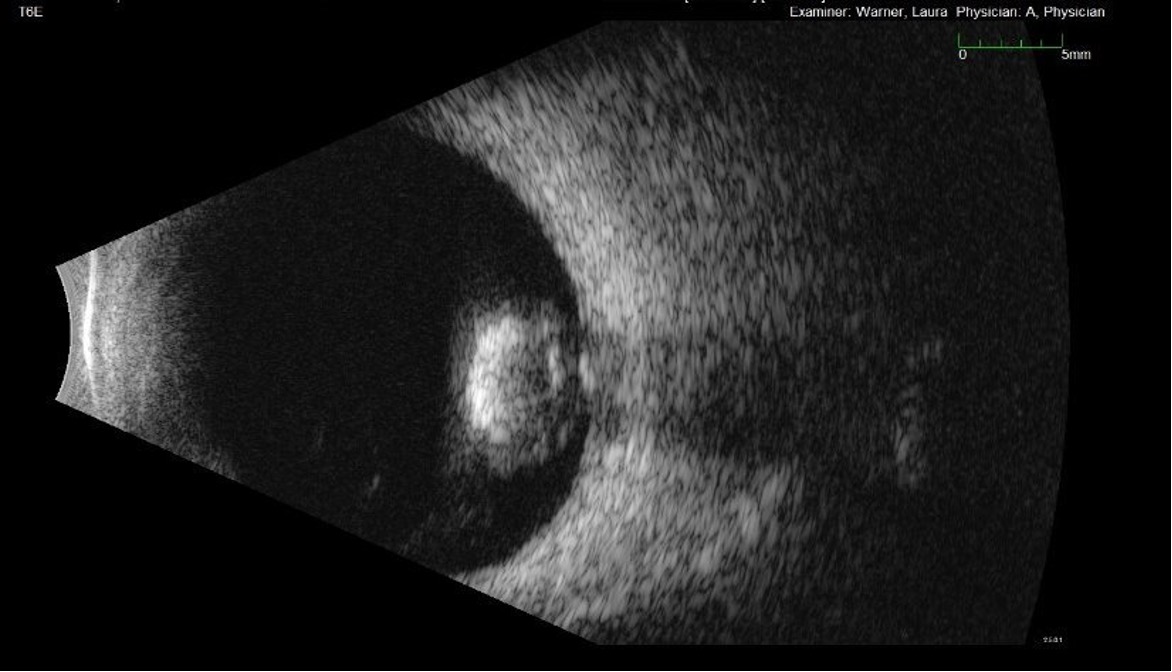
The patient was initially treated for possible stroke vs MS flare at the outside hosUltrasound of the orbit showed a lens material dislocated into the posterior segment with vitreous debris leaking protein, consistent with phacolytic glaucoma. The patient was placed on prednisolone 1% four times daily. Given the eye had no light perception at baseline, vitrectomy and/or cataract extraction were not indicated.
One week after prednisolone therapy, the pain resolved. Slit lamp exam revealed 1+ cell with flare, improved from 2-3+ cell and flare on initial presentation. Intraocular pressure was 14 mmHg. Risk for sympathetic ophthalmia was determined to be low given that the eye/ lens capsule had not been violated. Utilizing shared decision-making with the patient, we decided to continue watchful waiting given that the eye was painless. We discussed red flag signs and symptoms for pressure spikes in case the patient had a steroid response. We were less concerned for asymptomatic high pressures given that this was an NLP eye. We also broached the topic of enucleation in the future if the eye became painful.
The patient was seen again at week 3 and found to have complete resolution of all anterior chamber and anterior vitreous inflammation and pressure had elevated to 23 mmHg, but the patient denied any pain. The patient was continued on prednisolone 1% four times daily with a plan to taper if he starts to have symptomatically elevated pressures, and he will return in 6 months for check in.
DIAGNOSIS: Phacolytic glaucoma
DISCUSSION
Etiology/Epidemiology:
Phacolytic glaucoma is a secondary open-angle glaucoma in which leaked lens proteins from a hypermature cataract induce an inflammatory reaction in the anterior chamber, disrupting aqueous humor outflow(1). Most patients are over the age of 60, given age is the strongest risk factor for hypermature cataract formation. There is a slightly higher predilection in females, with one study citing a 1.7:1 female to male in incidence. The diagnosis is more commonly seen in patients from resource-limited areas with barriers to healthcare or who have a contraindication to cataract extraction in the eye (ex. no light perception in our patient)(2).
Signs/Symptoms:
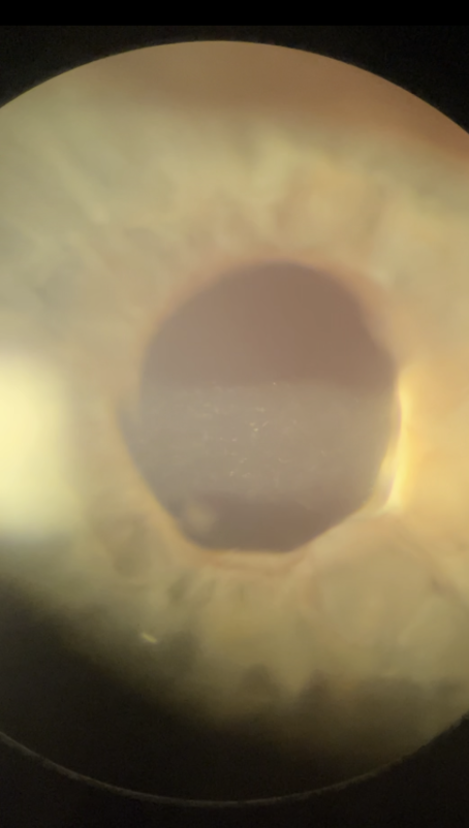
It is important to recognize that vision loss will likely not be the patient’s chief concern, given a hypermature cataract will have established chronic vision loss prior to any inflammatory reaction(3). Thus, most common chief concerns include pain, epiphora, or conjunctival injection. On slit lamp examination, lens cortical particulates may be visible in the anterior chamber. Signs that distinguish phacolytic from phacoantigenic glaucoma include the notable lack of keratic precipitates in phacolytic glaucoma(4). While increased intraocular pressure is a feature of most cases, it is not required. In our case, preexisting damage to the ciliary body resulted in comorbid reduced aqueous humor production and a low intraocular pressure despite the disruption in aqueous humor outflow.
Testing/Laboratory work-up:
Anterior chamber paracentesis can be performed to decrease intraocular pressure and collect fluid for cytopathology. Light microscopy shows activated epithelioid histiocytes containing lenticular material, but an absence of histiocytes does not rule out the diagnosis(5).
Imaging:
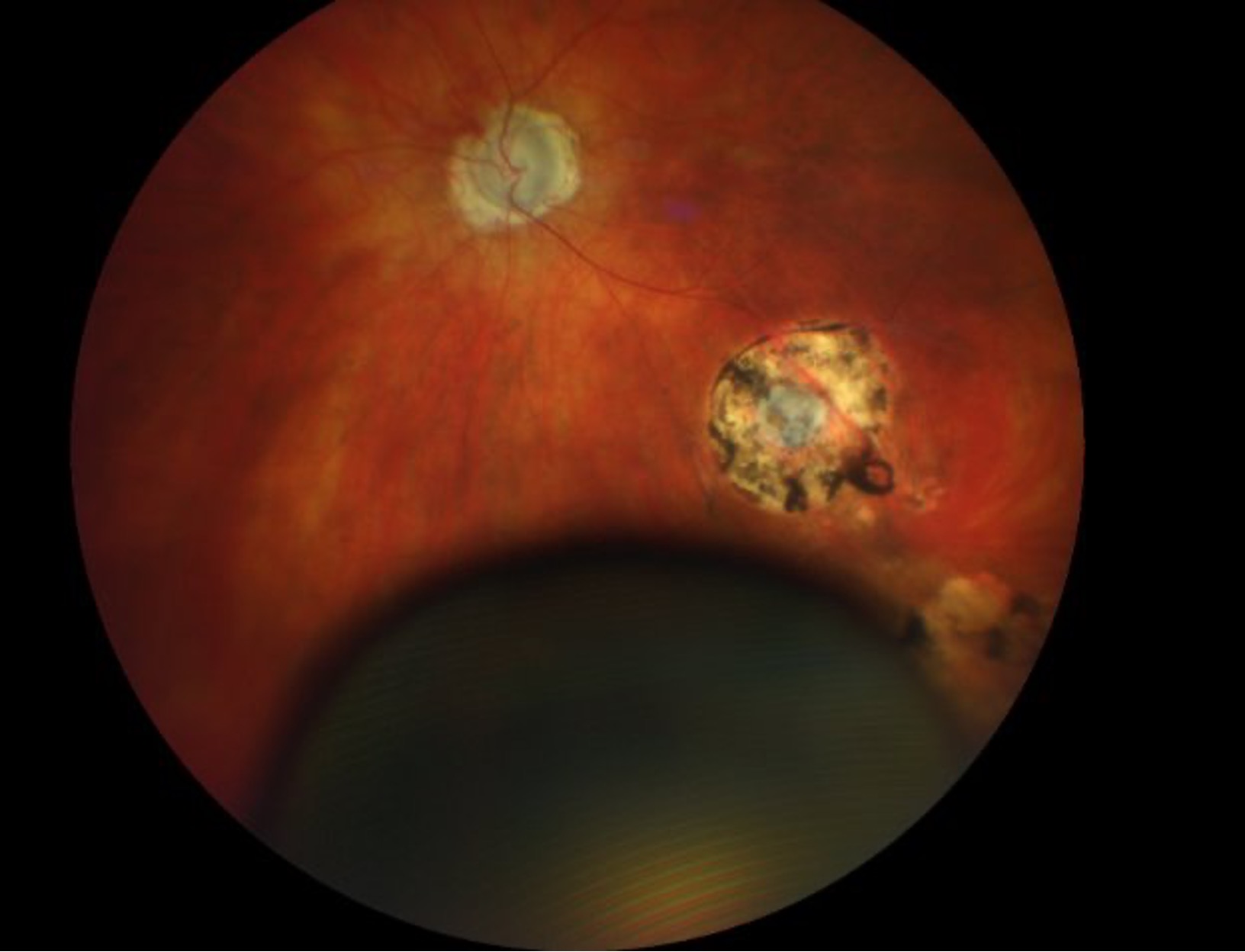
Posterior segment imaging is important to rule out differential diagnosis (ex. endophthalmitis)(6) and detect co-morbid posterior segment pathology prior to cataract extraction.
Treatment/Management/Guidelines
Early presentation is a crucial prognostic factor; one study of 50 patients with lens-induced glaucoma found that vision was preserved if medical and surgical management occurred within 2 weeks of symptom onset(7). Definitive treatment is cataract extraction(2). Concurrent trabeculectomy can be considered if the patient presents seven or more days after symptom onset, especially in settings where postoperative medical IOP management may be unavailable. In our case, cataract extraction was not a treatment option due to pre-existing no light perception in the affected eye.
Medical management includes cycloplegics for pain management, aggressive topical medications to lower IOP, and topical steroids to decrease inflammation. Patients should undergo postoperative dilated fundus examination and visual field testing to establish a new baseline and detect posterior pathology that was previously obscured by the hypermature cataract.
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
RELATED LINKS:
Al-Kaylani HM, Lovett Jr. EA, Oladele-Ajose A, Boese E. Phacolytic glaucoma in an eye with no light perception. EyeRounds.org February 24, 2026. Available from https://EyeRounds.org/cases/375-phacolytic-glaucoma.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links