University of Iowa
Department of Ophthalmology and Visual Sciences
Posted April 3, 2024
Introduction
A combination of factors maintains the lower eyelid in proper height and position against the globe; therefore, management of lower eyelid malpositions such as ectropion, entropion, and retraction requires precise identification of the underlying cause. Ectropion is an outward turning of the eyelid, and can be categorized primarily as involutional, cicatricial, paralytic, or mechanical. In contrast, entropion occurs when the eyelid turns inward. Entropion can be involutional, cicatricial, spastic, or congenital. Lower eyelid retraction results when the lower eyelid margin is displaced inferiorly while still maintaining good apposition of the lid margin to the globe. The aim of the tutorial is to help readers identify the major types of lower eyelid ectropion, entropion, and retraction, and to develop an appropriate treatment plan based on the causative etiology. Where relevant, readers are directed to videos, case reports, and other articles published elsewhere on EyeRounds.org.
Ectropion
Involutional Ectropion
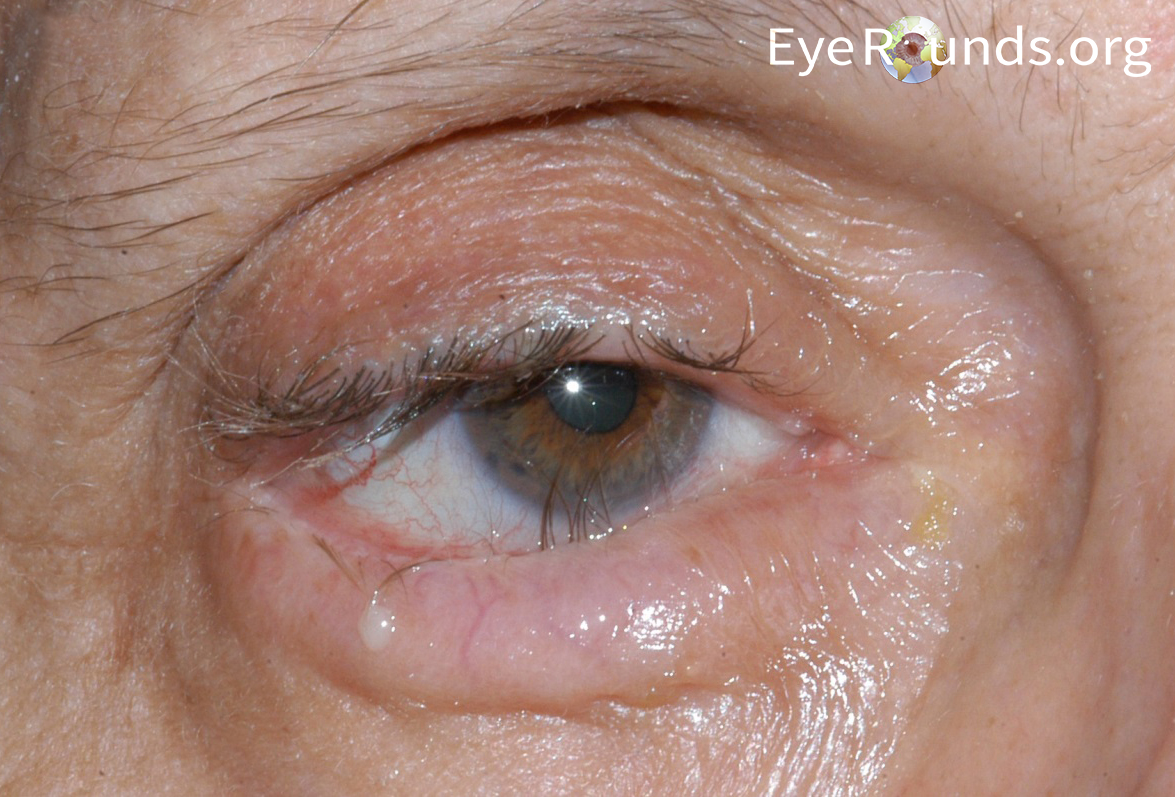
Involutional ectropion is the most commonly encountered type of ectropion, and classically occurs due to lid laxity among older patients (Figure 1) [1-3]. Involutional changes include distraction of the lower lid from the globe and retractor disinsertion. For additional discussion, please refer to this EyeRounds case report.
Clinical signs of lower eyelid retractor disinsertion, such as:
Deep inferior fornix
“Shelf-like” appearance of the lower lid
Reduced or absent movement of the lower eyelid on downgaze
Disinserted edge of retractors seen through the conjunctiva
Physical Examination
Eyelid distraction test
Distraction of the lower lid > 5 mm from the globe is considered a positive finding for eyelid laxity.
Snapback test
Performed by pulling the lid outward and asking the patient not to blink
Amount of laxity is graded based on the time it takes for the lid to return to normal position [9]:
Grade 0 (Normal): returns to position immediately on release
Grade I: returns to position in 2 - 3 seconds
Grade II: returns to position in 4 - 5 seconds
Grade III: returns to position in greater than 5 seconds and/or with a blink
Grade IV: never returns to position
Treatment
Treatment of lower lid ectropion may include conservative and/or surgical options. Conservative medical therapy consists of aggressive lubrication with artificial tears and ointment, and may include the use of a topical steroid to quiet any conjunctival inflammation; however, surgery is the definitive treatment for involutional ectropion. Surgery typically involves horizontal tightening and vertical stabilization/rotation. Common horizontal tightening procedures include canthoplasty (i.e. lateral tarsal strip), canthopexy, and wedge resection. Popular vertical stabilization/rotational eyelid procedures include retractor reinsertion, medial spindle, and inverting sutures. The amount of laxity and etiology of the ectropion will help guide treatment plans. When available, the procedures are hyperlinked to Dr. Richard Allen’s instructional videos published elsewhere in EyeRounds.
Corrects horizontal laxity by shortening the horizontal length of the lower lid at the lateral canthus
A “tarsal strip” is created by separating the anterior and posterior lamellar and removing the lateral aspect of tarsus. The strip is shortened intraoperatively according to the degree of tightening needed and fixed to the lateral orbital rim, providing appropriate lid tension.
Often perfomed in conjunction with a medial spindle, retractor reinsertion, and/or inverting sutures depending on the degree of involutional ectropion
For patients with concurrent upper eyelid laxity with a high risk of eyelash imbrication, a lateral tarsal strip with a lateral mini-tarsorrhaphy may be performed as an alternative to lateral tarsal strip alone [10]
Lateral canthopexy
Typically utilizes a suture to tighten the lateral canthal tendon without opening the canthal angle [11]
Appropriate for treating mild degrees of eyelid laxity
Wedge resection
Utilizes lower eyelid wedge resection and reconstruction to tighten the lower eyelid
Care must be taken to precisely align the eyelid margin and avoid eyelid margin notching by slighting everting the eyelid margin during reconstruction [12].
Lazy-T is a variation that relies on a full-thickness wedge resection to correct horizontal eyelid laxity while simultaneously performing a diamond-shaped tarso-conjunctival resection below the punctum to correct vertical laxity, useful for correcting ectropion with punctal eversion [13].
Corrects vertical instability of the ectropic eyelid
Utilizing a transconjunctival approach, the lower lid retractors are identified and resecured to the inferior border of tarsus [6, 14]. The retractors can also be reinserted through a transcutaneous approach.
Often combined with a lateral tarsal strip to correct concurrent horizontal laxity of the lid
Medial spindle
Corrects punctal eversion in cases where lateral tarsal strip alone will not restore the punctum to its anatomical position
Conjunctiva inferior to the lower punctum is excised and the medial lower lid retractors are engaged with a suture and resuspended to the inferior aspect of the tarsal plate in the lower lid. The sutures are then externalized through the skin and tied to provide inverting mechanical force on the punctum [15].
Commonly combined with other procedures to repair ectropion, such as lateral tarsal strip, depending on the severity of the eyelid malpositon
Corrects pronounced ectropion, such as tarsal ectropion, and vertical instability
Multiple transcutaneous inverting sutures are placed below the inferior border of the tarsus, with the goal of slight overcorrection. The looping passage of inverting sutures through the full thickness of the eyelid provides a vector force that pulls the tarsal plate downward and rotates the lid margin posteriorly. Additionally, the resulting inflammatory scar induced by the absorbable sutures helps keep the lid margin in anatomic position after absorption of the sutures [6, 14, 16].
Cicatricial Ectropion
Cicatricial ectropion is less common than involutional ectropion, and occurs due to shortening of the anterior lamella [17].
Etiology
Anterior lamella deficiency
Causes may include:
Sun damage, previous surgery, burns
Scarring resulting from blepharitis [18]
Ichthyosis
Contact dermatitis from over-the-counter cosmetics or topical eye drops, especially brimonidine, brinzolamide, and dorzolamide [19-21] (Figure 2)
Have the patient look up while opening his or her mouth. If moderate to severe anterior lamellar deficiency is present, the lower eyelid margin will often be pulled away from the globe.
Treatment
The goal in treating cicatricial ectropion is to lengthen the anterior lamella and stabilize the lid. In select cases, conservative or medical management may be sufficient. The best practice for managing drug-induced ectropion is to promptly withdraw the suspected offending agent and prescribe an alternative eye drop, if possible [20]. Steroid may be additionally needed to decrease inflammation.
Surgical management of cicatricial ectropion generally involves dissection and removal of any scar tissue to restore appropriate mobility to the lower lid anterior lamella. This naturally creates an anterior lamellar defect, which is reconstructed with a full-thickness skin graft. There is often a concurrent role for horizontal lid tightening procedures, such as a lateral tarsal strip or a lateral canthopexy [22], the details of which were discussed previously. In addition, some patients may benefit from cheek elevation or stabilization.
Donor skin graft site should be non-hair bearing with healthy, thin skin
An ideal donor site would be redundant upper eyelid skin obtained from a blepharoplasty, followed by the post-auricular, pre-auricular, or supraclavicular regions. Other sites include the inner upper arm, inguinal area, or the inframammary fold.
Once the lower lid cicatricial tissue is released and the size of the defect is measured, full thickness skin at the donor skin graft site is harvested down to the subcutaneous fat. The graft is thinned and trimmed as needed, and sewn into the lower lid defect.
Cheek elevation/stabilization
Relieves tension or weight from the lower lid
Exposure and elevation of the sub-orbicularis oculi fat (SOOF) by suture fixation to the orbital rim may be sufficient. In cases requiring more lift or stabilization, dissection along the anterior midface down to the periosteal or subperiosteal plane can be coupled with a fixating device (e.g., Endotine® midface B) or drill holes in the inferior orbital rim with suture fixation to elevate the cheek [23]. See the following EyeRounds videos on the various midface lift techniques: periosteal strip and mid-face lift, drill hole midface lift, and midface lift with Endotine midface B device.
Paralytic Ectropion
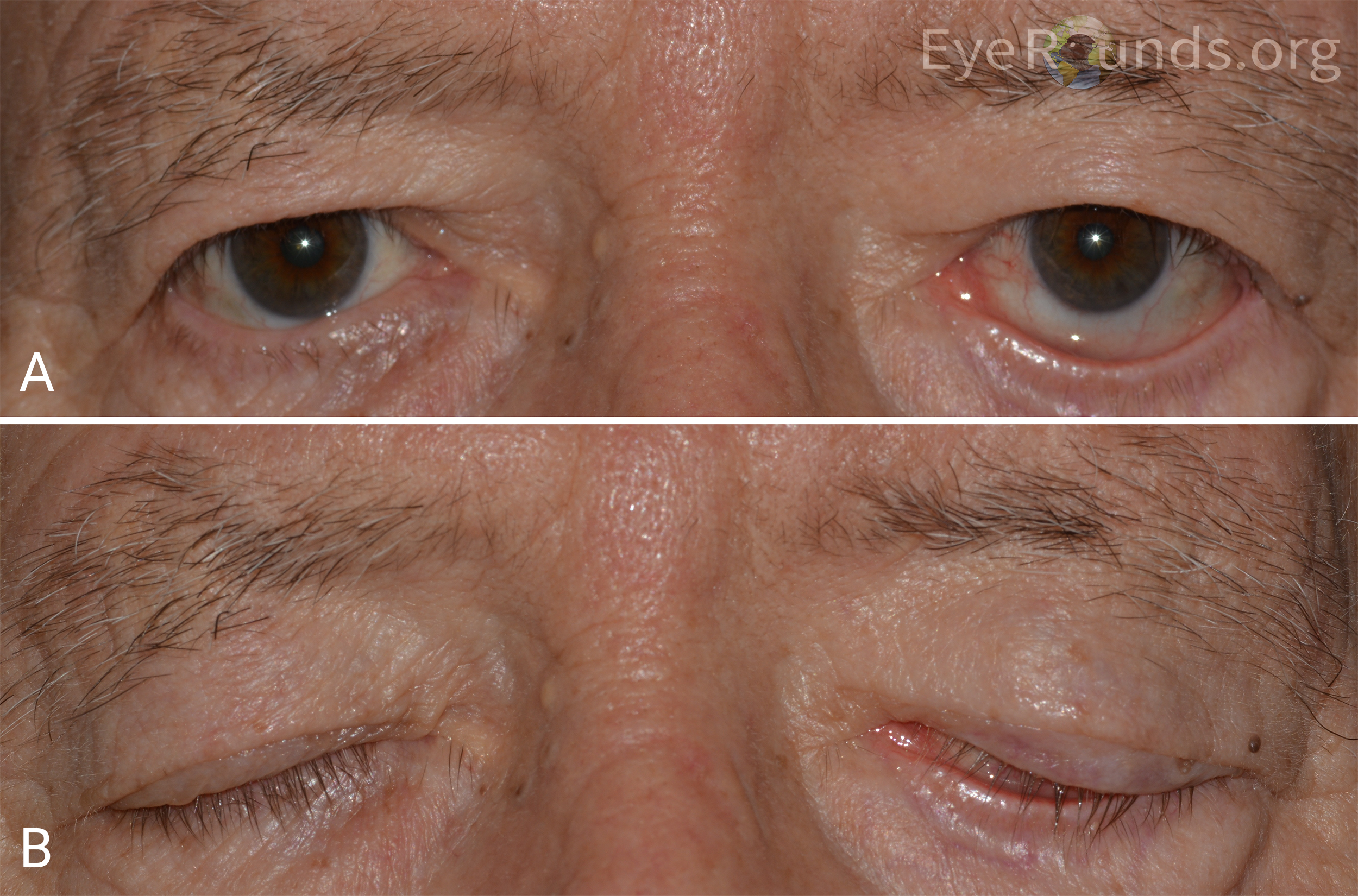
Paralytic ectropion most commonly occurs secondary to facial nerve palsy. This section discusses the etiology, clinical presentation, and treatments of paralytic ectropion. For additional discussion, please refer to this EyeRounds case report.
Etiology
Decreased orbicularis oculi muscle tone
Exacerbates any pre-existing horizontal eyelid laxity and can lead to ectropion, retraction of the lower lid, and lagophthalmos [24]
Most commonly due to facial nerve palsy, which may arise from:
Idiopathic Bell’s palsy [25]
Infection
Trauma including iatrogenic causes
Tumor
Infection (e.g., Lyme disease)
Inflammation (e.g., Ramsay-Hunt syndrome) [7]
Clinical Presentation
Symptoms
Ocular irritation
Dry eye
Epiphora (secondary to reflex tearing from exposure keratopathy as well as impaired drainage with ectropion and punctal eversion)
Signs
Lagophthalmos
Lower lid retraction
Exposure keratopathy
Physical Examination
Orbicularis oculi muscle tone evaluation in forced eyelid closure
Patient is asked to forcibly close the eyelids, and the extent to which the eyelashes are buried is noted [26].
Grading of ocular involvement in facial nerve palsy using the adapted House-Brackman guide [26, 27]:
Grade I: Normal blink and eyelid closure
Grade II: Full eyelid closure with minimal effort
Grade III: Full eyelid closure with maximal effort
Grade IV: Incomplete closure with normal facial symmetry
Grade V: Incomplete closure with facial asymmetry
Grade VI: No eyelid movement
Treatment
To treat paralytic ectropion, the underlying cause of the facial weakness must be addressed when possible. Conservative measures may be appropriate to temporize or treat mild cases of paralytic lower lid ectropion.
The primary aim of conservative therapy for paralytic ectropion is to protect the cornea. Mild paralytic ectropion may be managed with frequent doses of artificial tears and lubricating ointments. Transient interventions, such as botulinum toxin injection into the levator and/or placement of a temporary tarsorrhaphy, may be performed to induce protective ptosis when necessary [28].
However, if the paralysis does not improve for more than six months or is causing vision-threatening ocular surface issues, surgical management of paralytic ectropion may be pursued [29]. A lateral tarsal strip, possibly coupled with a medial spindle operation, can alleviate epiphora and exposure-related conjunctival inflammation. Yet, poor orbicularis muscle contraction compromises the lacrimal pump function, leading to epiphora that, unfortunately, can persist even after correction of the lower eyelid malposition [30]. Moreover, these initial surgical managements of paralytic ectropion may be insufficient to support the weight of the sagging lower eyelid and midface. In these cases, a SOOF or midface lift and/or medial and lateral tarsorrhaphies may be warranted.
Lower eyelid malposition in facial nerve palsy often needs to be treated more aggressively than simple ectropion and when severe can be thought of as lower eyelid retraction [26]. A combination of lower lid spacer grafting, lateral canthoplasty, and midface suspension can be effective in treating lagophthalmos and keratopathy associated with paralytic ectropion [31]. Techniques to elevate the retracted lower eyelid are discussed in detail in the Lower Eyelid Retraction section of this tutorial.
Mechanical Ectropion
Mechanical ectropion occurs due to the effect of gravity from a large lesion of the eyelid or cheek, edema, or mechanical weight from significant facial ptosis. Mechanical ectropion is treated by addressing the underlying cause. Additional treatments and/or surgical interventions are considered to correct any remaining involutional or cicatricial changes [29].
Entropion
Involutional Entropion
Involutional entropion is the most commonly encountered type of entropion in the elderly population, and classically shares many of the anatomic characteristics as involutional ectropion (Figure 3) [2]. However, the symptoms of involutional entropion are typically more severe and less well tolerated by patients than those of involutional ectropion. The abrasive contact between the keratinized skin of the inverted eyelid margin and eyelashes with the corneal and conjunctival surfaces is highly irritating. For additional discussion, please refer to this EyeRounds case report.
Important pathogenic factor for both involutional ectropion and entropion
May be be secondary to retractor dehiscence [33]
Retractor dehiscence
Destabilizes the tarsal plate, rendering it susceptible to the superiorly and anteriorly directed push of an overriding orbicularis oculi muscle and protruding fat pads
Spastic component
More commonly occurs in eyelids that are already predisposed to involutional entropion [24]
Patients treated for spastic entropion are likely to develop involutional entropion later, due to underlying eyelid laxity.
Overriding of the preseptal over the pretarsal orbicularis oculi muscle
May be induced by retractor dehiscence or lamellar dissociation
Lamellar dissociation results from laxity in the connection between the preseptal orbicularis muscle and the orbital septum [7]. Regardless of the etiology, the migration of the preseptal orbicularis oculi muscle over the pretarsal portion rotates the eyelid margin against the globe, thereby forming entropion [7].
Clinical Presentation
Symptoms
Ocular irritation
Foreign body sensation
Signs
Corneal epitheliopathy
Alleviation of symptoms by manual eversion of eyelids [15]
Evaluation of orbicularis oculi muscle override in forceful eyelid closure
Ask the patient to forcefully close the eyelid and observe whether overriding of the preseptal orbicularis oculi muscle is induced [17].
Inspection of lower eyelid retractor dehiscence [34]
Overriding of the lower eyelid margin above the lower limbus is indicative of some laxity of the lower eyelid retractors.
Look for clinical signs of lower eyelid retractor disinsertion, such as the deep resting position of inferior fornix, reduced or absent movement of the lower eyelid on downgaze, and a white line of the disinserted lower lid retractors in the inferior fornix.
Treatment
The goal in treating involutional entropion is to address some or all of the three causative factors of involutional entropion: eyelid laxity, retractor disinsertion, and overriding preseptal orbicularis oculi muscle. Retractor reinsertion with a lateral tarsal strip is frequently the procedure of choice to treat involutional entropion. Quickert sutures may be used alternatively to treat involutional entropion, either by itself or in conjunction with a lateral tarsal strip, such as in the care of debilitated patients for whom a retractor reinsertion procedure is not viable [35]. Though not done frequently, one could also consider a partial orbicularis myectomy.
Lower eyelid retractors are identified and dissected free from the underlying conjunctiva posteriorly and reattached to the inferior tarsal margin. It is typical to perform the procedure in conjunction with a lateral tarsal strip (or pentagonal wedge) to further stabilize the lid by addressing lower lid laxity [34].
Tightens the lower eyelid retractors without any skin incisions
Useful for resolving spastic entropion or when retractor reinsertion is not viable
Double-armed everting sutures are placed medially, centrally, and laterally through the disinserted retractors and passed superiorly along the anterior-inferior border of the tarsus and then tied in a subciliary fashion to provide slight overcorrection of the lower eyelid margin. As the sutures dissolve over 7 – 10 days, they plicate and strengthen the retractors. Moreover, the resulting scar tissue helps mechanically tighten the lower eyelid retractors and prevents the overriding of orbicularis oculi muscle [34].
May be performed in conjunction with a lateral tarsal strip to achieve longer-lasting correction or to address more significant involutional entropion [35]
Cicatricial Entropion
Though less common than involutional entropion, cicatricial entropion is still widespread in parts of the world where trachoma is endemic [15]. It occurs due to shortening of the posterior lamella relative to the anterior lamella. Marginal entropion is a subtle form of cicatricial entropion, in which the posterior eyelid margin has a slightly rolled appearance and the mucocutaneous junction is more anterior than normal. Trichiasis – misdirected eyelashes – are a common result of marginal entropion [17].
Etiology
Ocular cicatricial pemphigoid
This inflammatory process requires immediate medical management, as surgical treatment in uncontrolled ocular cicatricial pemphigoid can worsen the cicatrizing process and potentially cause severe ankyloblepharon (24). For additional discussion, please refer to the EyeRounds case report and online atlas.
Stevens-Johnson syndrome
Trachoma
Trauma
Chemical injury
Recurrent chalazia or blepharitis
Clinical Presentation
Symptoms
Ocular irritation
May complain of increased tearing
• Signs
Contracture and/or scarring of the conjunctiva and the tarsal plate
Inability to evert the eyelid to relieve symptoms
Eyelid inversion
Physical Examination
Distraction and snanpback tests
If the eyelid is resistant to manual repositioning and reverts to its inverted position immediately upon release, the entropion is cicatricial [34].
Posterior lamella inspection
Inspect for shrinkage or scarring of the conjunctiva and tarsal plate.
Treatment
The goal in treating cicatricial entropion is to lengthen the posterior lamella. The choice of surgical treatment depends on the severity and extent of posterior lamellar scarring. Tarsal fracture may be appropriate for repairing mild cicatricial entropion, whereas mucous membrane grafting may be needed to correct moderate to severe forms of cicatricial entropion. Horizontal eyelid stabilization may also be needed if there is significant horizontal eyelid laxity.
Removes the scar tissue and lengthens the posterior lamella by a small amount
A horizontal incision is made midway across the posterior aspect of the tarsus. Then, the tarsal plate is fractured and angled anteriorly. Sutures are passed full thickness through the lid, entering the inferior edge of the cut tarsus and exiting just inferior to the lashes anteriorly, to evert the lid margin. Slight overcorrection is desirable, as some inversion will occur with healing.
Lengthens the posterior lamella and prevents its recurrent contracture
Graft materials can be either mucous membrane, such as the buccal or labial mucosa of the oral cavity, or amniotic membrane (AmnioGuard® or AmnioGraft ®) (34). The scarred conjunctiva is excised, then the mucous membrane is grafted over the defect.
Spastic Entropion
Spastic entropion classically occurs when there is sustained contraction of the orbicularis oculi muscle leading to inward turning of the eyelid margin. Spastic entropion can be seen in response to ocular surface issues, and can often be accompanied by involutional changes. In older patients with pre-existing lid laxity, ocular surgery and ensuing inflammation can cause a reflexive spasm of the orbicularis oculi muscle. The entropion is worsened by irritation due to voluntary squeezing of the eyes [36].
Etiology
Recent ocular surgery
Ocular irritation or inflammation
Dry eye
Clinical Presentation
Symptoms
Ocular irritation
Signs
Reflex blepharospasm
Involutional changes
Lower eyelid and canthal tendon laxity
Lower eyelid retractor laxity
Physical Exam
Orbicularis oculi muscle inspection
Inspect for the presence of eyelid spasms. Look for the orbicularis oculi muscle forcefully overriding the lower lid margin, pushing the lid margin inward [34].
Snapback and distraction tests for evaluation of lower lid laxity
Treatment
The goal in treating spastic entropion is to resolve the cycle that involves squeezing of the eyelids leading to worsened entropion. Conservative medical therapy consists of lubrication, a bandage contact lens, or eyelid taping to break the cycle [37]. Botulinum toxin injection into the pretarsal or preseptal orbicularis muscle is another effective temporary measure to prevent the reflexive muscle spasm [38]. Surgical treatment of choice for spastic entropion is Quickert sutures, possibly coupled with a lateral tarsal strip [35]. Occasionally, retractor reinsertion with a lateral tarsal strip and myectomy are also considered.
Congenital Entropion & Epiblepharon
Congenital lower lid entropion is extremely rare and thought to arise when both the anterior and posterior attachments of the capsulopalebral fascia are dysfunctional. However, rare case reports of congenital entropion with intact lower eyelid retractors suggest that retractor disinsertion is not a universal etiologic mechanism in congenital entropion [39]. Congenital lower eyelid entropion may also involve posterior lamella deficiency, canthal tendon laxity, overriding anterior lamella, and facial nerve palsies. If lower eyelid retractor disinsertion is present, it is repaired by a retractor reinsertion procedure, such as seen in the treatment for involutional entropion. Overriding anterior lamella is corrected by excision of redundant pretarsal orbicularis oculi muscle, as seen in this Eyerounds video.
Congenital entropion should be not confused with epiblepharon. In epiblepharon, redundant anterior lamella extends beyond the eyelid margin and presses the eyelashes vertically against the globe (Figure 4). There is no intrinsic malposition of the eyelid. The condition usually presents bilaterally shortly after birth, and resolves with normal facial growth [40]. Treatment is reserved for symptomatic cases and involves excision of the redundant anterior lamella [41]. For additional discussion on surgical management of epiblepharon, please refer to this Eyerounds video.
Lower eyelid retraction is a malposition in which the lower eyelid is inferiorly displaced, exposing sclera between the inferior limbus and the lower eyelid margin in the absence of eyelid eversion or inversion (Figure 5). The etiology of lower lid retraction is multifactorial. Any cicatricial process in the orbital septum that tethers the eyelid to the orbital rim will lead to lower eyelid retraction [7, 43]. There may be an ectropion or entropion component that correlates with a length discrepancy between the anterior and posterior lamella or scarring in either lamella [7]. Patients with eyelid retraction require thoughtful evaluation and surgical planning because they often need more complex surgical techniques to avoid complications. This section discusses the etiology, clinical presentation, and treatments for lower eyelid retraction.
Trauma involving the lower eyelids or midface that results in anterior or middle lamellar scarring and vertical shortening
Iatrogenic surgical scarring
Cosmetic surgeries such as lower eyelid blepharoplasty with excessive skin removal or excision of cutaneous malignancy may cause anterior lamellar insufficiency and middle lamellar scarring. Anterior lamella insufficiency, combined with middle lamellar scarring, leads to lower lid retraction rather than ectropion [43].
Surgical recession of the inferior rectus muscle can lead to lower eyelid retraction, due to the anatomic connection between the extraocular muscle and the retractors, i.e. capsulopalpebral fascia and inferior tarsal muscle [44].
Thyroid eye disease
Lower lid retraction is present at diagnosis in about 20% of Graves’ ophthalmopathy patients [45]. Inferior rectus muscle recession, excessive contraction of the inferior tarsal muscle with increased sympathetic tone, and/or proptosis can all contribute to lid retraction in patients with thryoid eye disease [45].
Midface hypoplasia
Patients with a hypoplastic midface have an inferior orbital rim that is posterior relative to the globe. These patients have less support for the lower lid and are thus prone to lower eyelid retraction or ectropion. Moreover, tightening of the lower eyelid can cause the lid to slide under the globe, causing or worsening existing lower eyelid retraction [46].
Facial nerve palsy
Paralytic ectropion is associated with lower eyelid retraction due to loss of the orbicularis oculi muscle support. Horizontal eyelid tightening alone is often insufficient to elevate the eyelid. Therefore, paralytic ectropion is best approached as a case of lower eyelid retraction rather than simple ectropion.
Clinical Presentation
Symptoms
Ocular irritation
Epiphora
Mattering
Signs
Margin-reflex distance 2 (MRD2) measurement of greater than 5 mm [36]
Inferior scleral show
Lagophthalmos
Exposure keratopathy
Horizontal lid laxity
Midface descent
Negative orbitomalar vector
Physical Examination
Lower eyelid inspection and margin-reflex distance quantification
MRD2 of greater than 5 mm is considered retraction [36].
Evaluation of anterior, middle, and posterior lamellar involvement
If anterior lamellar deficiency is present, pushing the eyelid margin and cheek superiorly against the globe to lengthen the lower eyelid anterior lamella should bring the eyelid margin to anatomic position. Failure to reposition the eyelid above the inferior corneal limbus or mid-pupillary line with this technique is indicative of middle and posterior lamellar involvement [47].
Pre-operative planning
A system of digital maneuvers (“finger test”) may be used for pre-operative planning based on severity and anatomic considerations [43].
One finger is placed at the lateral canthus and gently pushes it upward and laterally. If the maneuver repositions the lower eyelid to a satisfactory position, consider lateral tarsal strip or canthopexy to address horizontal laxity.
If placing one finger does not reposition the eyelid, place a second finger below the pupil at the lower eyelid margin. If two fingers reposition the lower eyelid, consider an anterior spacer graft and lateral canthal tightening.
If two fingers reposition the lower eyelid but midface descent is still present, place a third finger over the malar eminence and push up. If three fingers reposition the eyelid and cheek fat pad, then consider a hard palate/mucosal spacer graft, preperiosteal malar fat pad elevation, and lateral tarsal strip/canthopexy.
If three fingers do not reposition the eyelid and midface due to inadequate lower eyelid skin, place a fourth finger over the cheek pushing it superolaterally. If four fingers reposition the midface and the eyelid, consider subperiosteal midface elevation, the mucosal spacer graft, and lateral tarsal strip/canthopexy.
Treatment
The goal in treating lower eyelid retraction is to re-establish the lamellar relationship and stabilize the lid. Tissue shortage in the anterior lamella is corrected by advancing anterior lamella via non-surgical means including massage, recruitment of vertical skin from the midface, or supplementng with a skin graft. Middle and posterior lamellar scarring is corrected by release of scar tissue and insertion of a spacer graft to vertically elevate the lower eyelid. Rarely, in patients with marked proptosis, globe prominence may be addressed via orbital decompression.
Augmentation of the anterior lamella without use of spacer graft
Full thickness skin graft
Appropriate for treating lower lid retraction due only to a severe shortage of skin
Suborbicularis oculi fat (SOOF) lift is one of the many techniques to reposition the malar fat pad and cheek tissues. It is frequently combined with horizontal tightening procedures such as the lateral tarsal strip. In the transconjunctival subperiosteal approach, distal periosteum is released and sutures are passed through the arcus marginalis lifting the periosteum and SOOF. The SOOF is anchored superolaterally to the arcus marginalis and the superficial temporal fascia; alternatively, the SOOF may be anchored to the deep temporal fascia just lateral to the lateral orbital rim [48].
Hyaluronic acid gel injections
Hyaluronic acid gel injections to the lower lid and midface are a non-surgical alternative to treat lower eyelid retraction [49, 50].
Augmentation of the posteror lamella with spacer graft insertion
Appropriate for surgically correcting posterior lamella deficiency
May be combined with spacer graft insertion between the lower eyelid retractors and inferior tarsal border to lengthen the posterior lamella and give a more predictable result
For patients with significant lower eyelid retraction with exposure keratopathy, retractor recession with a spacer graft in addition to lateral tarsal strip and a small tarsorrhaphy is typically preferred [26]. See this EyeRounds video on retractor recession with medial and lateral tarsorrhaphy.
Damasceno RW, Osaki MH, Dantas PEC, Belfort RJ. Involutional entropion and ectropion of the lower eyelid: prevalence and associated risk factors in the elderly population. Ophthalmic Plast Reconstr Surg 2011;27(5):317-320. [PMID 21415800]
Damasceno RW, Osaki MH, Dantas PEC, Belfort RJ. Involutional Entropion and Ectropion of the Lower Eyelid: Prevalence and Associated Risk Factors in the Elderly Population. Ophthalmic Plastic & Reconstructive Surgery 2011;27(5):317-320. [PMID 00002341-201109000-00003]
Guthrie AJ, Kadakia P, Rosenberg J. Eyelid Malposition Repair: A Review of the Literature and Current Techniques. Seminars in plastic surgery 2019;33(2):92-102. [PMID 31037045]
Lenci LT, Clark TJE, Allen RC. Involutional ectropion: Options for surgical management of ectropion. Eyerounds.org, August 24, 2015; Available from: https://eyerounds.org/cases/218-ectropion.htm
Shah-Desai S, Collin R. Role of the lower lid retractors in involutional ectropion repair. Orbit 2001;20(2):81-86. [PMID 12045919]
Rudolf F, Guthoff JAK, editor. Oculoplastics and Orbit. Germany: Springer, 2007.
Bashour M, Harvey J. Causes of Involutional Ectropion and Entropion-Age-Related Tarsal Changes Are the Key. Ophthalmic Plastic & Reconstructive Surgery 2000;16(2)
Chee R-i, Lelli GJ. Snapback Test. In: Schmidt-Erfurth U, Kohnen T, editors. Encyclopedia of Ophthalmology. Berlin, Heidelberg: Springer Berlin Heidelberg; 2018; p. 1648-1650.
Vagefi MR, Anderson RL. The Lateral Tarsal Strip Mini-Tarsorrhaphy Procedure. Archives of Facial Plastic Surgery 2009;11(2):136-139
Georgescu D. Surgical preferences for lateral canthoplasty and canthopexy. Curr Opin Ophthalmol 2014;25(5):449-454. [PMID 25050757]
Korn BS, Kikkawa DO. Video atlas of oculofacial plastic and reconstructive surgery / edited by Bobby Korn, Don Kikkawa. Second edition.. ed. Place of publication not identified]: Place of publication not identified : Elsevier, 2017.
Smith B. The "Lazy-T" Correction of Ectropion of the Lower Punctum. Archives of Ophthalmology 1976;94(7):1149-1150
Tse DT, Kronish JW, Buus D. Surgical Correction of Lower-Eyelid Tarsal Ectropion by Reinsertion of the Retractors. Archives of Ophthalmology 1991;109(3):427-431
Nerad JA. Oculoplastic Surgery (The Requisites in Ophthalmology), 2002.
Berry-Brincat A, Burns J, Sampath R. Inverting sutures for tarsal ectropion (the leicester modified suture technique). Ophthalmic Plast Reconstr Surg 2013;29(5):400-402. [PMID 24022353]
Korn BS. 2020-2021 Basic and Clinical Science Course, Section 7: Oculofacial Plastic and Orbital Surgery. San Francisco, CA: American Academy of Ophthalmology, 2020.
Kopsachilis N, Tsaousis KT, Tourtas T, Tsinopoulos IT. Severe chronic blepharitis and scarring ectropion associated with discoid lupus erythematosus. Clin Exp Optom 2013;96(1):124-125. [PMID 22845188]
Chisholm SAM, Couch SM, Custer PL. Etiology and Management of Allergic Eyelid Dermatitis. Ophthalmic Plast Reconstr Surg 2017;33(4):248-250. [PMID 27333449]
Hegde V, Robinson R, Dean F, Mulvihill HA, Ahluwalia H. Drug-induced ectropion: what is best practice? Ophthalmology 2007;114(2):362-366. [PMID 17270684]
Jia Ern Ong TQ, Laageide L, Ko AC. Periocular Dermatitis and Cicatricial Ectropion Secondary to Cosopt (Dorzolamide-Timolol). Eyerounds.org, October 30, 2019
O'Donnell BA. Eyelid retractor surgery as an adjunct to cicatricial ectropion repair. Clin Exp Ophthalmol 2000;28(4):293-297. [PMID 11021560]
Lenci LT, Clark TJE, Allen RC. Involutional ectropion: Options for surgical management of ectropion. Eyerounds.org, posted August 24, 2015; Available from: https://eyerounds.org/cases/218-ectropion.htm
Mannis MJ, Holland EJ. Cornea / edited by Mark J. Mannis, Edward J. Holland. Fifth edition.. ed. Amsterdam: Amsterdam : Elsevier, 2022.
Tiemstra JD, Khatkhate N. Bell's palsy: diagnosis and management. Am Fam Physician 2007;76(7):997-1002. [PMID 17956069]
Welder JD AR, Shriver EM. Facial Nerve Palsy: Ocular Complications and Management. Eyerounds.org July 14, 2015,
House JW, Brackmann DE. Facial Nerve Grading System. Otolaryngology–Head and Neck Surgery 1985;93(2):146-147. [PMID 3921901]
Seift SR, Chang J. Management Of Ophthalmic Complications Of Facial Nerve Palsy. Otolaryngologic Clinics of North America 1992;25(3):669-690
Salmon JF. Kanski's clinical ophthalmology : a systematic approach / John F. Salmon, MD, FRCS, FRCOphth. Ninth edition.. ed. Edinburgh]: Edinburgh : Elsevier, 2020.
Custer PL. Ophthalmic management of the facial palsy patient. Seminars in plastic surgery 2004;18(1):31-38. [PMID 20574468]
Patel MP, Shapiro MD, Spinelli HM. Combined hard palate spacer graft, midface suspension, and lateral canthoplasty for lower eyelid retraction: a tripartite approach. Plast Reconstr Surg 2005;115(7):2105-2114; discussion 2115-2107. [PMID 15923862]
Clark TJE, Lenci LT, Allen RC, Shriver EM. Involutional entropion: options for surgical management of entropion. EyeRounds.org, Sept 14, 2015; Available from: https://eyerounds.org/cases/220-involutional-entropion.htm
Scheepers MA, Singh R, Ng J, Zuercher D, Gibson A, Bunce C, Fong K, Michaelides M, Olver J. A Randomized Controlled Trial Comparing Everting Sutures with Everting Sutures and a Lateral Tarsal Strip for Involutional Entropion. Ophthalmology 2010;117(2):352-355
Nerad JA. Techniques in ophthalmic plastic surgery : a personal tutorial / Jeffrey A. Nerad. Second edition.. ed. Philadelphia, PA: Philadelphia, PA : Elsevier, 2021.
Rougraff PM, Tse DT, Johnson TE, Feuer W. Involutional entropion repair with fornix sutures and lateral tarsal strip procedure. Ophthalmic Plast Reconstr Surg 2001;17(4):281-287. [PMID 11476179]
Javier Servat J, Baylin EB. Surgical Anatomy of the Eyelid. In: Gladstone GJ, Nesi FA, Black EH, editors. Oculoplastic Surgery Atlas: Eyelid and Lacrimal Disorders. Cham: Springer International Publishing; 2018; p. 1-12.
Burkat CN. Malposition of the Eyelids. In: Mark J. Mannis EJH, editor. Cornea: Fundamentals, Diagnosis and Management: Elsevier Inc.; 2022; chapter 26; p. 259-275.
Cillino S, Raimondi G, Guépratte N, Damiani S, Cillino M, Di Pace F, Casuccio A. Long-term efficacy of botulinum toxin A for treatment of blepharospasm, hemifacial spasm, and spastic entropion: a multicentre study using two drug-dose escalation indexes. Eye 2010;24(4):600-607
Bartley GB, Maguire LJ, Nerad JA, Kersten RC. Congenital Entropion with Intact Lower Eyelid Retractor Insertion. American Journal of Ophthalmology 1991;112(4):437-441
Noda S, Hayasaka S, Setogawa T. Epiblepharon with inverted eyelashes in Japanese children. I. Incidence and symptoms. Br J Ophthalmol 1989;73(2):126-127. [PMID 2930758]
Yanoff M, Duker JS. Ophthalmology / lead editors, Myron Yanoff, Jay S. Duker
section editors, James J. Augsburger and [11 others]. Fifth edition.. ed. Edinburgh: Edinburgh : Elsevier Saunders, 2018.
Vislisel J. Epiblepharon. Ophthalmic Atlas Images: EyeRounds.org. Available from: https://eyerounds.org/atlas/pages/epiblepharon/index.htm
Patipa M. The evaluation and management of lower eyelid retraction following cosmetic surgery. Plast Reconstr Surg 2000;106(2):438-453; discussion 454-439. [PMID 10946945]
Meyer DR, Simon JW, Kansora M. Primary Infratarsal Lower Eyelid Retractor Lysis to Prevent Eyelid Retraction After Inferior Rectus Muscle Recession. American Journal of Ophthalmology 1996;122(3):331-339
Liao SL, Wei YH. Correction of lower lid retraction using tarSys bioengineered grafts for graves ophthalmopathy. Am J Ophthalmol 2013;156(2):387-392.e381. [PMID 23659973]
Ko AC, Korn BS, Kikkawa DO. The aging face. Survey of Ophthalmology 2017;62(2):190-202
Straka DG, Foster JA. Update on the Treatment of Postblepharoplasty Lower Eyelid Retraction. Advances in Cosmetic Surgery 2019;2(1):121-134
Olver JM. Raising the suborbicularis oculi fat (SOOF): its role in chronic facial palsy. Br J Ophthalmol 2000;84(12):1401-1406. [PMID 11090482]
Goldberg RA, Lee S, Jayasundera T, Tsirbas A, Douglas RS, McCann JD. Treatment of lower eyelid retraction by expansion of the lower eyelid with hyaluronic Acid gel. Ophthalmic Plast Reconstr Surg 2007;23(5):343-348. [PMID 17881981]
Zamani M, Thyagarajan S, Olver JM. Functional Use of Hyaluronic Acid Gel in Lower Eyelid Retraction. Archives of Ophthalmology 2008;126(8):1157-1159
Korn BS, Kikkawa DO, Cohen SR, Hartstein M, Annunziata CC. Treatment of lower eyelid malposition with dermis fat grafting. Ophthalmology 2008;115(4):744-751.e742. [PMID 18067964]
Suggested Citation Format
Lee G, Diel RJ, Simmons BA, Allen RC, Pham CM, Carter KD, Shriver EM. Lower Eyelid Malpositions. EyeRounds.org. April 3, 2024; Available from https://EyeRounds.org/tutorials/lower-eyelid-malpositions/index.htm
University of Iowa
Roy J. and Lucille A. Carver College of Medicine
Department of Ophthalmology and Visual Sciences
200 Hawkins Drive
Iowa City, IA 52242
University of Iowa
Roy J. and Lucille A. Carver College of Medicine
Department of Ophthalmology and Visual Sciences
200 Hawkins Drive
Iowa City, IA 52242