INITIAL PRESENTATION
Chief Complaint: “My vision is blurry.”
History of Present Illness
33-year-old Caucasian female with a prior history of amelanotic left iris lesion for >6 years presented to the emergency department after developing sudden onset of progressively blurry vision while reading. She denied any flashes of light, floaters, curtaining of vision, trauma, or Valsalva-like event. She did not use anticoagulation.
Past Ocular History
Past Medical History
Medications
Allergies
Family History
Social History
Review of Systems
OCULAR EXAMINATION
| OD | OS | |
|---|---|---|
| Lids/lashes | Normal | Normal |
| Conjunctiva/sclera | Normal | 1+ Injection |
| Cornea | Clear | Clear and compact |
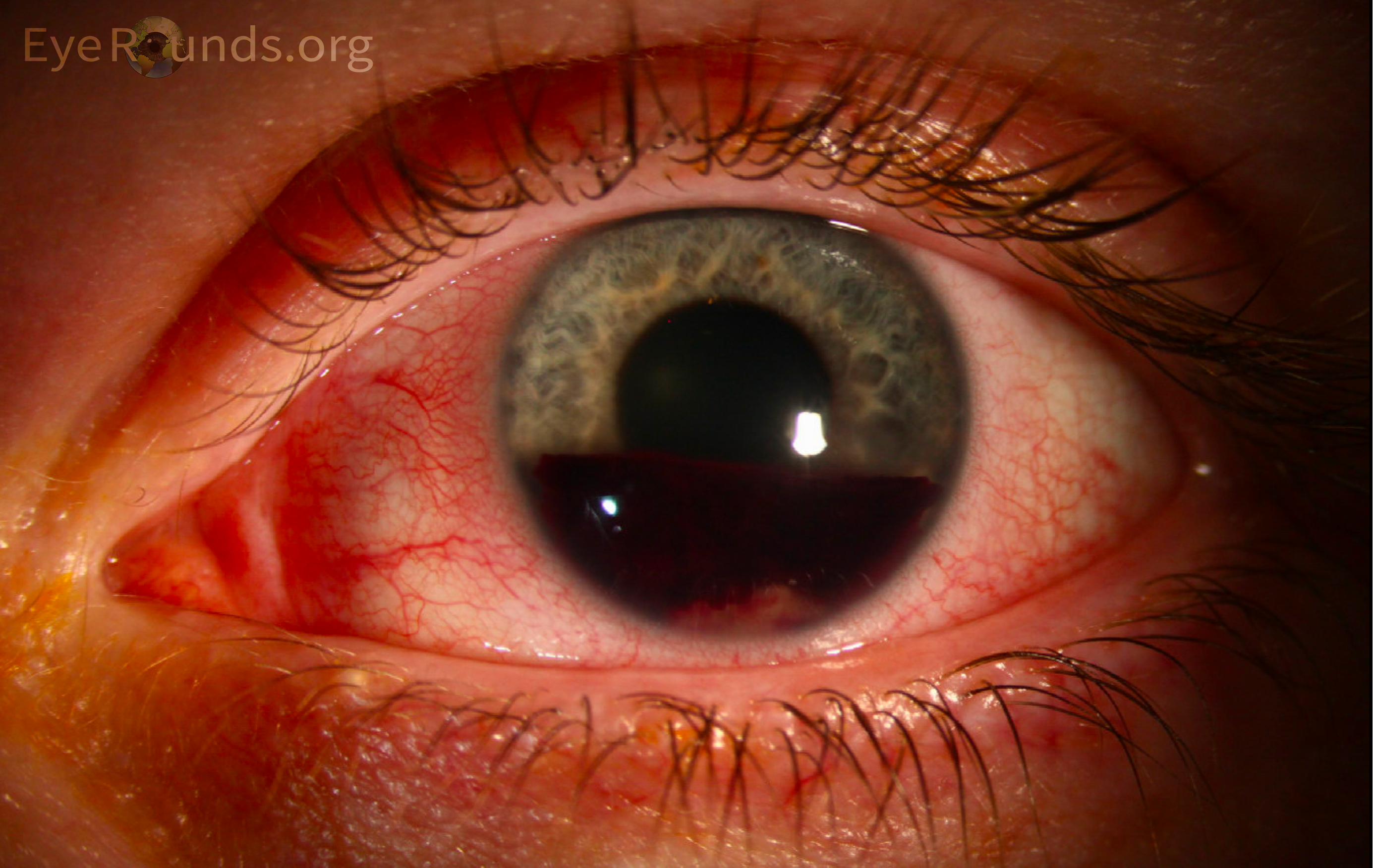
| Anterior Chamber | Normal | Inferior 40% layered hyphema with 3+ dispersed pigmented cell |
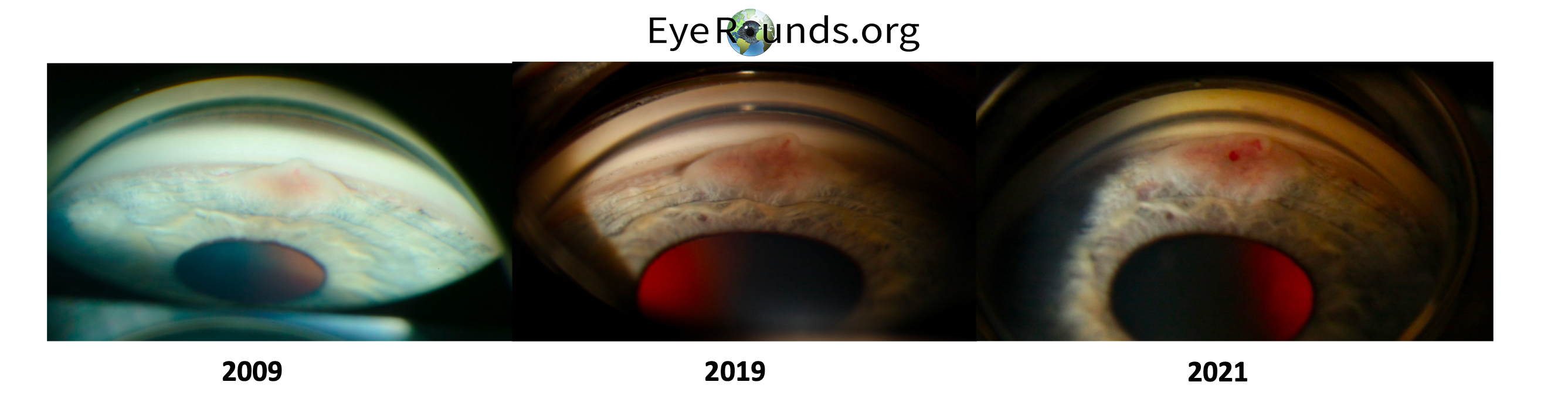
| Iris | Normal | Visible architecture appears unremarkable, inferiorly there is a raised vascular amelanotic lesion from about 5:30 to 6:30 that is partially obscured by hyphema |
| Lens | Normal | Phakic and clear |
| OD | OS | |
|---|---|---|
| Vitreous | Normal | Hazy view |
| Disc | Normal | Hazy view |
| Cup-to-disc ratio | Normal | Hazy view |
| Macula | Normal | Hazy view |
| Vessels | Normal | Hazy view |
| Periphery | Normal | Hazy view |
DIFFERENTIAL DIAGNOSIS
CLINICAL COURSE
The patient was evaluated in the emergency room and was diagnosed with hyphema in the setting of known amelanotic iris mass. She was advised to sleep with head of bed elevated to allow the anterior chamber blood to settle. Additionally, she was advised to limit physical activity and to avoid non-steroidal anti-inflammatory drugs as rebleeding precautions. She was started on cycloplegics for comfort, timolol 0.5% twice daily for elevated intraocular pressure, and prednisolone acetate four times daily for acute iritis.
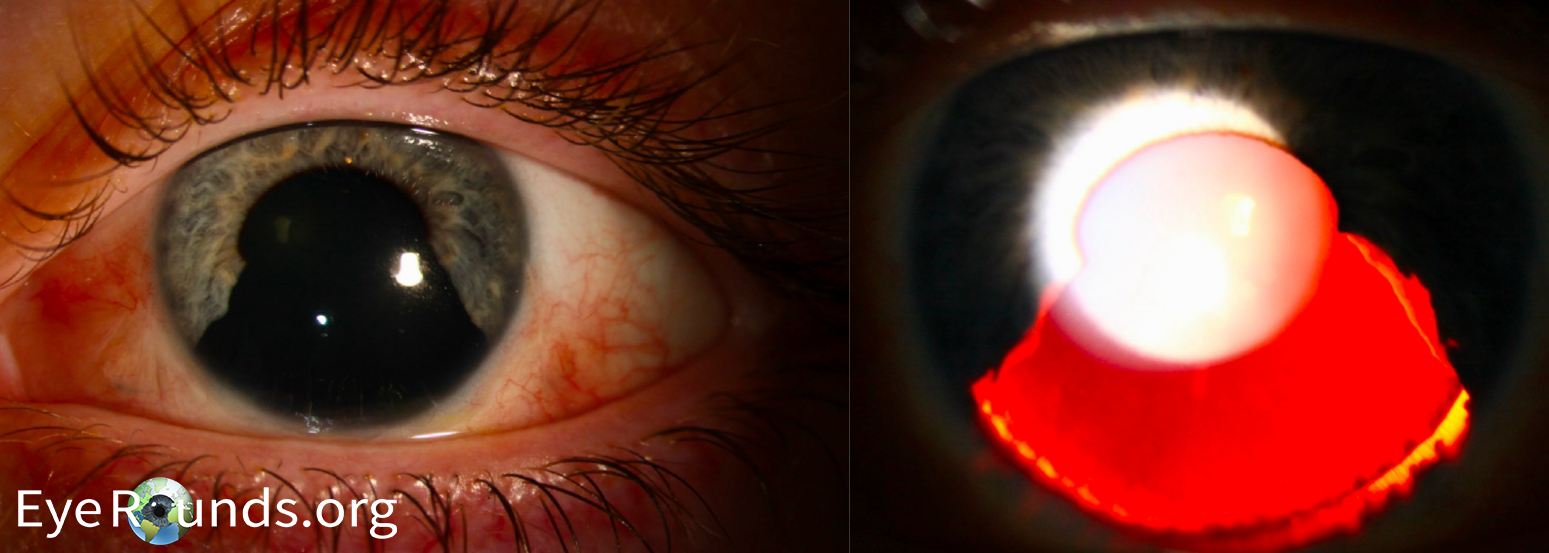
At her next-day follow-up appointment, her vision had improved to 20/20-2 in the left eye, intraocular pressure of the left eye had normalized to 16 mmHg by Goldmann applanation, and the view of the fundus was unremarkable. The decision was made at this time to allow the hyphema to self-resolve and then proceed with reevaluation of her lesion. The hyphema had decreased to a trace residual microhyphema by her one-week follow-up and had completely resolved at her 2-month follow-up appointment (see Figure 2 and 3 on date 2021).
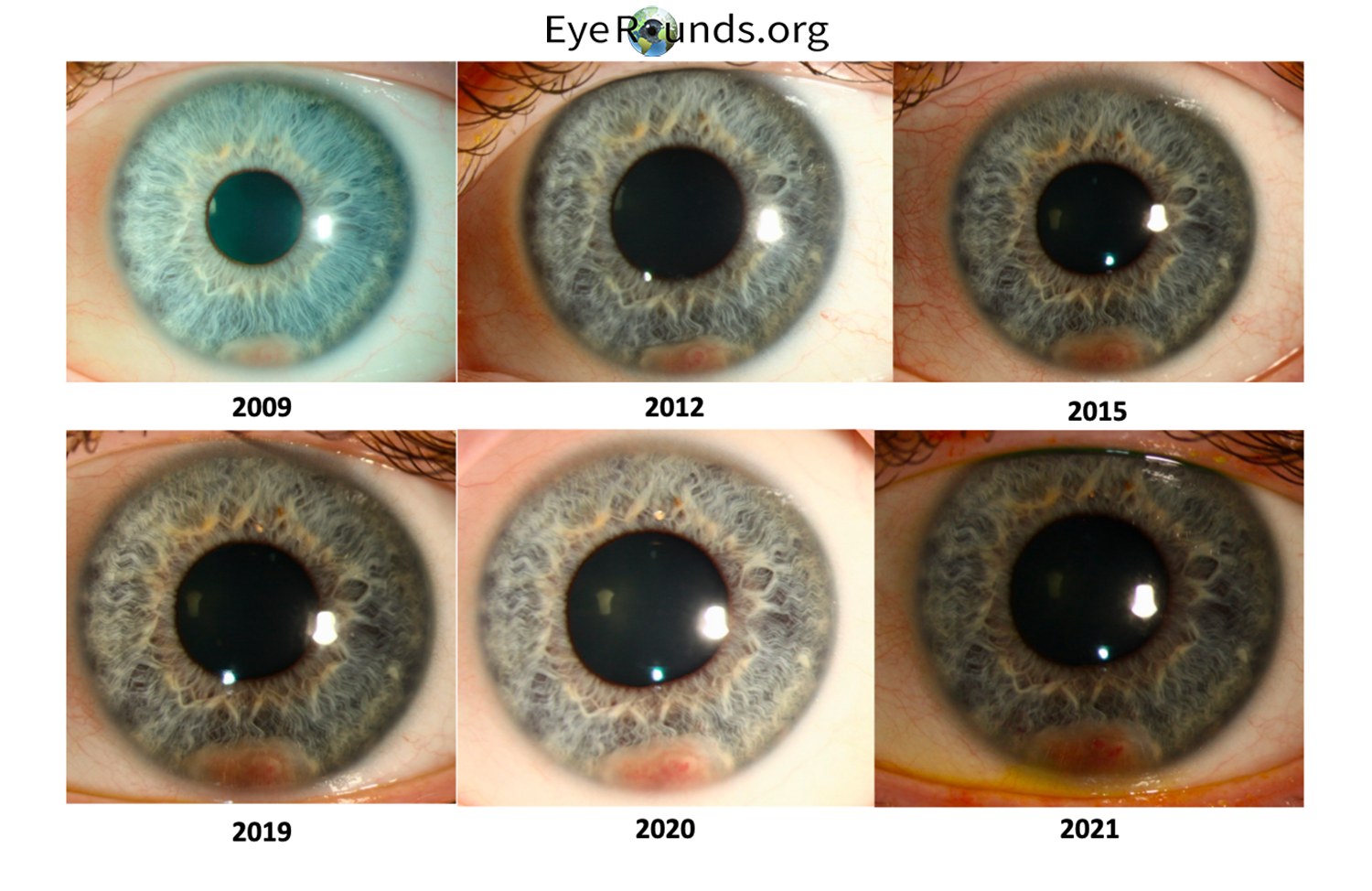
The patient had originally been evaluated for this iris lesion 10 years prior to presentation for hyphema. Given the atypical appearance of the lesion (elevation and vascularity) and the concern for melanoma, the patient was followed every 6 months to monitor for changes. After this period of initial observation, the patient elected to proceed with iridocyclectomy (See Figure 4 for postoperative appearance) 4 months after her presentation for hyphema due to concern for growth of the lesion and malignant transformation. Anatomic pathology evaluation of surgically resected tissue was read as amelanotic spindle cell nevus with surface plaque. A similar pathology image can be seen in Figure 7 in EyeRounds case, Iris-Ciliary Body Melanoma.
DIAGNOSIS: Spontaneous hyphema secondary to iris neoplasm
DISCUSSION
Etiology/Epidemiology
Hyphema is an accumulation of blood in the anterior chamber of the eye[1,2]. It can be divided by etiology, with the most common categories being traumatic, iatrogenic, and spontaneous[1,3]. Traumatic hyphemas carry an annual incidence of 12 injuries per 100,000 individuals[1,2,4-6]. Blunt force trauma (e.g. athletic injuries, workplace injury, assault, vehicle airbag deployment, recreational airsoft guns) is the most common traumatic mechanism, and occurs most frequently in individuals between age 10-20 years [1,2,5,6]. In the population less than 65 years of age, 66% of hyphemas occur in males, and among those 65 years of age or older, most cases occur in females (59.7%) [7].
Iatrogenic hyphema can develop following intraocular surgery or laser, especially in procedures that involve manipulation of the highly vascularized iris, such as laser peripheral iridotomy, angle-based procedures, and vitrectomy [1,2,5-14].
Spontaneous hyphema can occur in individuals with other ocular disease or systemic conditions that affect the eye, such as neoplastic or inflammatory conditions, as well as vascular malformations and neovascularization[1,2]. Examples include melanoma of the iris, metastatic tumors involving intraocular structures, juvenile xanthogranuloma, retinoblastoma, and Fuchs’ heterochromic iridocyclitis[1,2]. Neovascularization of the iris or angle can also lead to spontaneous hyphemas, and usually occurs in the setting of underlying diabetic or vasoocclusive disorders (i.e. ocular ischemic syndrome)[1,2,15-18]. Underlying hematologic dyscrasias such as von Willebrand disease, sickle cell disease, leukemia, hemophilia, and thrombocytopenia can also lead to spontaneous hyphemas[1,2]. Due to their close association with underlying ocular pathology, spontaneous hyphemas occur more commonly in adults than in children, and do not demonstrate a strong gender predilection [1,2,15-18].
Substances and medications which alter platelet function, such as alcohol, anticoagulants, and aspirin, can predispose to hyphema formation [1,2,15-18].
Pathophysiology
The source of heme in hyphema is most commonly from the highly vascular ciliary body and iris[1,2]. However, trauma or iatrogenic forces can disrupt the fragile vessels from the major arterial circle of the iris, the recurrent choroidal arteries, and the veins within the suprachoroidal space[1,2,16]. Penetrating trauma can shear structures directly, while blunt trauma stretches the globe, causing a rapid increase in intraocular pressure, equatorial globe expansion, and stress on structures and vasculature, leading to hemorrhage into the anterior chamber [1,2,16]. Delayed, spontaneous hyphema following intraocular surgery can arise following accumulation of granulation tissue or damaged vessels near the wound site[1]. A child presenting with hyphema without accompanying ocular or systemic disease may suggest further evaluation for a non-accidental injury[1,19]. Similarly, hyphemas can be a presenting symptom in cases of intimate partner violence [19].
Hematologic disorders, especially sickle cell disease and sickle cell trait, increase the chance of blockage of aqueous outflow through the trabecular meshwork [1,4,20]. Patients with these conditions are more susceptible to increased IOP and permanent vision damage due to optic atrophy. Delayed secondary glaucoma can also arise in patients with a history of traumatic hyphema, and onset can occur weeks or even years after the initial injury and recovery [1]. The incidence of late-onset glaucoma secondary to hyphema is estimated to be between 0%-20%, and typically occurs following angle recession, anterior synechiae formation, trabecular meshwork fibrosis, or trabecular endothelial siderosis [1,5]. In the setting of traumatic hyphema, permanent visual damage can also arise from traumatic optic neuropathy [19].
Signs/Symptoms
Presenting symptoms include acute decrease in visual acuity, photophobia, and eye pain proportional to the volume of blood in the anterior chamber [1,5,21]. Pain may also be a result of increased IOP [1,5,21].
A hyphema is graded based on the quantity of anterior chamber blood[1,5,16] (see Table 1). Poor aqueous circulation in cases of total hyphema causes oxidation of anterior chamber blood, leading to a darkened appearance known as an “eight ball hyphema” [16,22]. Eight ball hyphemas tend to have a worse prognosis than total red-colored hyphemas at grade IV or lower, and the risk of secondary glaucoma in these cases is near 100% [1,16].
| Grade | Volume of blood in anterior chamber | Risk of IOP elevation/ secondary glaucoma |
|---|---|---|
| Grade 0: Microhyphema | Circulating erythrocytes | low risk |
| Grade I | Blood occupies <1/3 of the anterior chamber | ~10% chance of IOP increase |
| Grade II | Blood occupies 1/3-1/2 of the anterior chamber | ~10% chance of IOP increase |
| Grade III | Blood occupies 1/2 to < total of the anterior chamber | ~25% chance of IOP increase |
| Grade IV | Blood occupies the entire anterior chamber | ~50% chance of IOP increase |
| "Eight ball" hyphema | Blood occupies entire anterior chamber turns a darker color due to impaired circulation | 100% chance of IOP increase |
Testing/Laboratory Work-Up/Imaging
In the setting of trauma, workup must first be targeted at stabilizing the patient and assessing for other signs of intracranial or intraocular injury [1]. Notably, hyphema can be a presenting symptom of nonaccidental trauma in pediatric patients and intimate partner violence in adults [19]. Testing for hemoglobinopathies and bleeding disorders including prothrombin time, partial thromboplastin time, platelet count may be indicated [1,2,4,6,20]. Of note, spontaneous hyphemas in African American patients warrants sickle cell screenings in patients not previously tested. A thorough ophthalmic exam is recommended for all patients, including measuring IOP and assessment for other sequela of ocular trauma including open globe injury, retinal detachment, and retrobulbar hemorrhage [1,6]. In cases where the hyphema precludes view of the posterior chamber, a B-scan ultrasound can be performed [1,6]. Computed tomography (CT) may be warranted if there is suspicion of facial fractures, intracranial hemorrhages, retained intraocular foreign bodies, or other injuries [1,6].
Treatment/Management/Guidelines
Conservative management
Most hyphemas are self-resolving, and treatment is supportive in uncomplicated cases [1,5,6,8]. It is recommended to wear eye protection at all times, elevate the head of bed (HOB) above 30 degrees, minimize activity, and avoid anticoagulant and antiplatelet agents such as aspirin and ibuprofen to prevent rebleeding [1,5,6,8]. Anti-emetics may help control nausea, as Valsalva can increase the risk of rebleeding [1,5]. Hyphemas are typically managed on an outpatient basis, but hospitalization may be indicated in patients with severe hyphema (> grade II) or with additional ocular complications, patients with a high risk of rebleeding due to hematologic disorders, and patients who are at risk for noncompliance with bed rest at home, such as children [1,23]. Close follow up is important for all patients due to the risk of rebleeding and IOP spikes, which occurs most frequently in the first week after injury [1,23].
Medical management (see Table 2)
For patients with elevated IOP, topical aqueous suppressants, including beta-blockers (timolol) and alpha agonists (brimonidine) are first line therapies [1,2]. Topical carbonic anhydrase inhibitors (dorzolamide) can also be used but should be avoided in patients with suspected sickle cell hemoglobinopathies as they increase aqueous acidity and thus the risk of sickling [1,2,6]. For patients with severe IOP elevations, systemic carbonic anhydrase or hyperosmotic agents may be needed, with methazolamide recommended over acetazolamide in patients with sickle cell hemoglobinopathies [1,2].
Cycloplegics such as atropine 1% and cyclopentolate can be used in patients with ciliary spasm or symptomatic photophobia, and can reduce the risk of posterior synechiae formation [4-6,24].
Topical corticosteroids can reduce inflammation, decrease the rate of secondary rebleeding by inhibition of fibrinolysis, and help prevent formation of posterior synechiae[1,5,8]. Standard recommendations include a slow taper of topical prednisolone acetate 1%, but some patients may require a stronger regimen with dexamethasone or systemic steroids [6,25].
The role of antifibrinolytic agents remains controversial. Various studies have found that aminocaproic acid (ACA) and tranexamic acid (TXA) reduce the rate of rebleeding in patients with traumatic hyphema [1,5,6,26-28]. However, meta-analysis demonstrates that the rate of rebleeds is similar with the use of antifibrinolytic agents or corticosteroids, with no statistically significant difference in final visual outcomes between treated and untreated groups [20]. Furthermore, ACA and TXA can be associated with higher costs as well as serious side effects such as hypotension and retinovascular disease [29,30]. At time of publication, there are no commercially available topical formulations of ACA or TXA. ACA is contraindicated in pregnancy due to its teratogenic effects, as well as in patients with increased risk for thromboembolus, hepatic dysfunction, and renal dysfunction [1,5].
| Medication | Indication | Considerations |
|---|---|---|
| Beta blockers and alpha-2 agonists | Elevated IOP | First-line therapy – aqueous suppression |
| Topical carbonic anhydrase inhibitors | Elevated IOP | Increase aqueous humor acidity; Promote sickling in sickle cell hemoglobinopathies |
| Systemic carbonic anhydrase inhibitors | Elevated IOP | Promote systemic acidosis; Metronidazole is recommended over acetazolamide in patients with sickle cell hemoglobinopathies or severe renal disease |
| Cycloplegics | Ciliary spasm, photophobia | Reduces ciliary spasm and risk of posterior synechiae formation |
| Topical or systemic corticosteroids | Hyphema | Reduce inflammation, secondary rebleeding, posterior synechiae formation |
| Antifibrinolytic agents | Controversial | May reduce the rate of rebleeding; ACA contraindicated in pregnancy; Risk of serious side effects |
Surgical management
Surgical intervention may be indicated due to delayed clot resorption [6,31]. Surgical intervention should be considered when: IOP >60 mmHg for 48 hours (risk of optic atrophy), IOP >24 mmHg for the first 24 hours, repeated IOP measurements >30 mmHg in patients with sickle cell disease or trait, total hyphema with IOP >25 mmHg for 5 days (risk of corneal blood staining), corneal blood staining, or failure of hyphema resolution to <50% of the anterior chamber volume within 8 days (risk of anterior synechiae formation) [1,6,23,24,32]. Surgical management most commonly includes anterior chamber washout with irrigation and aspiration for clot removal [5,6,23]. Some patients may benefit from additional peripheral iridectomy (in cases of pupillary block) or glaucoma drainage implant placement (in cases of uncontrolled elevated IOP) [5,6,23].
Complications
Complications of hyphema include rebleeding, increased IOP, corneal blood staining, optic atrophy, and secondary glaucoma.
Rebleeding typically presents within one week of the original trauma [1,5]. Signs of rebleeding include increased size of the hyphema, accumulation of fresh, lighter-colored blood imposed on the older and darker blood, and dispersed erythrocytes within the anterior chamber [1]. Incidence of rebleeding varies in reports, ranging from 0.4% to 35%, although rebleeding is less likely with prompt and appropriate treatment [1,5,15,33,34]. Rebleeding can precipitate further complications including increased IOP, secondary glaucoma, and corneal blood staining [1,5,15]. Patients with a history of coagulopathy, delayed presentation to medical attention, presenting visual acuity of <20/200, initial hyphema grade of II or more, and elevated IOP at presentation are at greater risk of developing a rebleed [1,34].
Elevated IOP occurs in about 30% of posttraumatic hyphema cases due to obstruction of aqueous outflow[1]. Prolonged elevated IOP can lead to optic atrophy, notably with IOP ≥ 50 mmHg for 5 or more days, or ≥ 35 mmHg for 7 or more days[1,5]. Patients can also develop delayed secondary glaucoma, trabecular meshwork fibrosis, and trabecular endothelial siderosis [1,5].
Corneal blood staining following hyphema has an estimated incidence of at 2-11% [1]. Risk increases with higher grades of hyphema, rebleeding, slower resolution time, and a prolonged period of IOP elevation (IOP≥ 25 mmHg for ≥ 6 days) [1,5,15]. Corneal blood staining results from the release of hemoglobin into the aqueous humor and its diffusion into the corneal stroma, where it is metabolized into hemosiderin by keratocytes, which exerts a toxic effect on the corneal endothelium [1,5,9,15]. Blood staining is associated with corneal endothelial cell degeneration and endothelial cell loss over time [1,15]. Blood staining typically begins centrally, causing a yellow to brownish stromal discoloration which spreads peripherally [1,15]. Some cases of corneal blood staining can spontaneously resolve, with clearing of blood staining also beginning centrally and spreading outward over time, although some cases of blood staining may never clear completely. Patients with blood staining can experience photophobia due to accumulation of porphyrin throughout the corneal layers and subsequent production of cytotoxic oxygen radicals [1,15,21].
In pediatric patients within the amblyogenic age range, delayed hyphema clearance and corneal blood staining can lead to amblyopia [5].
In summary, hyphemas can result in long-term complications and require timely treatment and close monitoring for successful resolution.
EPIDEMIOLOGY OR ETIOLOGYTraumatic
Spontaneous
Iatrogenic |
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENTConservative
Medical
Surgical
Complications
|
Related Link
References
Hartness E, Garza Reyes A, Yu C, Sears N. Hyphema. EyeRounds.org. Feb. 20, 2024. Available from https://eyerounds.org/cases/345-hyphema.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links